Ischemic stroke
Reading File
Finding Sources
Searching PubMed
"ischemic stroke"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have enough information for a comprehensive response. Let me compile this into a thorough, well-structured answer.
Ischemic Stroke
Definition and Epidemiology
Ischemic stroke results from severe disruption of local cerebral blood flow (CBF) due to either in situ thrombosis or embolic obstruction from a proximal source. About 600,000 first-ever ischemic strokes occur annually in the US, with strokes being more common in Black and Hispanic populations compared to non-Hispanic whites. Approximately one-third of cases have no identifiable cause. - Rosen's Emergency Medicine, p. 1426
Pathophysiology and Classification
Ischemic strokes are classified by mechanism:
1. Thrombotic (~33%):
- Large-vessel occlusion (LVO): Clot forms at ulcerated atherosclerotic plaque, especially at vessel bifurcations in the internal carotid artery (ICA) territory. Significant flow reduction occurs when stenosis exceeds 90% of vessel diameter.
- Small-vessel / lacunar strokes: Involve terminal small vessels; infarcts range from a few mm to 2 cm, located in the basal ganglia, thalamus, pons, and internal capsule. Strongly associated with hypertension (80-90% of cases) and diabetes. Caused by lipohyalinosis (hypertensive cerebral vasculopathy) or small emboli.
2. Cardioembolic (~25%):
Most commonly from mural thrombus in atrial fibrillation - the leading cardiac cause. Patients with AF have an approximately 5-fold increased stroke risk. Non-cardiac embolic sources include diseased extracranial arteries (artery-to-artery embolism), and aortic atheromas.
3. Cryptogenic (~>33%):
No definite cause identified. Includes embolic stroke of undetermined source (ESUS).
4. Other causes:
- Young stroke (age 15-45, ~3-4% of all strokes): Pregnancy, oral contraceptives, antiphospholipid antibody syndrome, sickle cell anemia, polycythemia, cocaine/amphetamines, fibromuscular dysplasia, prolonged migraine vasospasm, infectious vasculopathies (varicella, fungal meningitis)
- Carotid/vertebral dissection: Leading determined cause in the young; may follow mild trauma (sneezing), or be associated with fibromuscular dysplasia or connective tissue disorders - Rosen's Emergency Medicine, p. 1427
Ischemic penumbra: Tissue that is critically hypoperfused but not yet infarcted, surrounding the ischemic core. This is the therapeutic target for reperfusion therapy. - Bradley and Daroff's Neurology, p. 858
Clinical Presentation
Symptoms appear suddenly or with a stuttering onset. They reflect the vascular territory involved:
Anterior Circulation (ICA, ACA, MCA)
| Territory | Key Deficits |
|---|---|
| MCA | Contralateral hemiplegia + hemisensory loss (arm/face > leg), contralateral homonymous hemianopia, ipsilateral gaze preference. If dominant hemisphere: aphasia (Broca = expressive; Wernicke = receptive) |
| ACA | Contralateral leg weakness > arm, altered mentation, impaired judgment, primitive reflexes (grasp, suck), bowel/bladder incontinence, apraxia of gait |
Aphasia vs. Dysarthria: Aphasia (wrong words/poor comprehension) localizes to dominant cortex (MCA territory). Dysarthria (poor articulation, intact word choice) is a motor speech deficit - can occur with any stroke. Do not confuse either with dysphagia (swallowing difficulty). - Rosen's Emergency Medicine, p. 1428
Posterior Circulation (vertebrobasilar)
Wide variety of symptoms reflecting cranial nerve deficits, cerebellar involvement, and sensory tract disruption. Consciousness may be lost (reticular activating system in brainstem). Posterior strokes may progress for up to 3 days (vs. 24 hours for anterior). Classic posterior circulation syndromes include:
- Lateral medullary (Wallenberg) syndrome: Ipsilateral facial numbness, Horner's syndrome, hoarseness, dysphagia, ataxia + contralateral body pain/temperature loss
- Basilar artery occlusion: Locked-in syndrome, quadriplegia, coma
Temporal Patterns
- Stroke in evolution: Worsening deficits over minutes to hours (~20% anterior, ~40% posterior)
- TIA: Transient focal symptoms, fully resolving, no infarction on imaging - high risk of subsequent stroke
Differential Diagnosis
Conditions that mimic ischemic stroke:
- Hypoglycemia - most important to exclude (may cause sustained focal deficits lasting days)
- Todd's postictal paralysis (post-seizure)
- Subdural/epidural hematoma (especially in elderly on anticoagulation)
- Brain tumor or abscess
- Wernicke encephalopathy (ophthalmoplegia, ataxia, confusion - mimics posterior fossa stroke)
- Complex migraine with focal aura
- Bell's palsy / vestibular neuronitis / labyrinthitis
- Giant cell arteritis (in elderly)
- Hypertensive encephalopathy
- Rosen's Emergency Medicine, p. 1430-1431
Diagnosis and Imaging
Initial Workup
- Immediate blood glucose (to rule out hypoglycemia)
- Non-contrast CT head (NCCT) - first-line, rapidly rules out hemorrhage
- ECG (identify AF, arrhythmias)
- Labs: CBC, BMP, coagulation studies, troponin
CT Findings
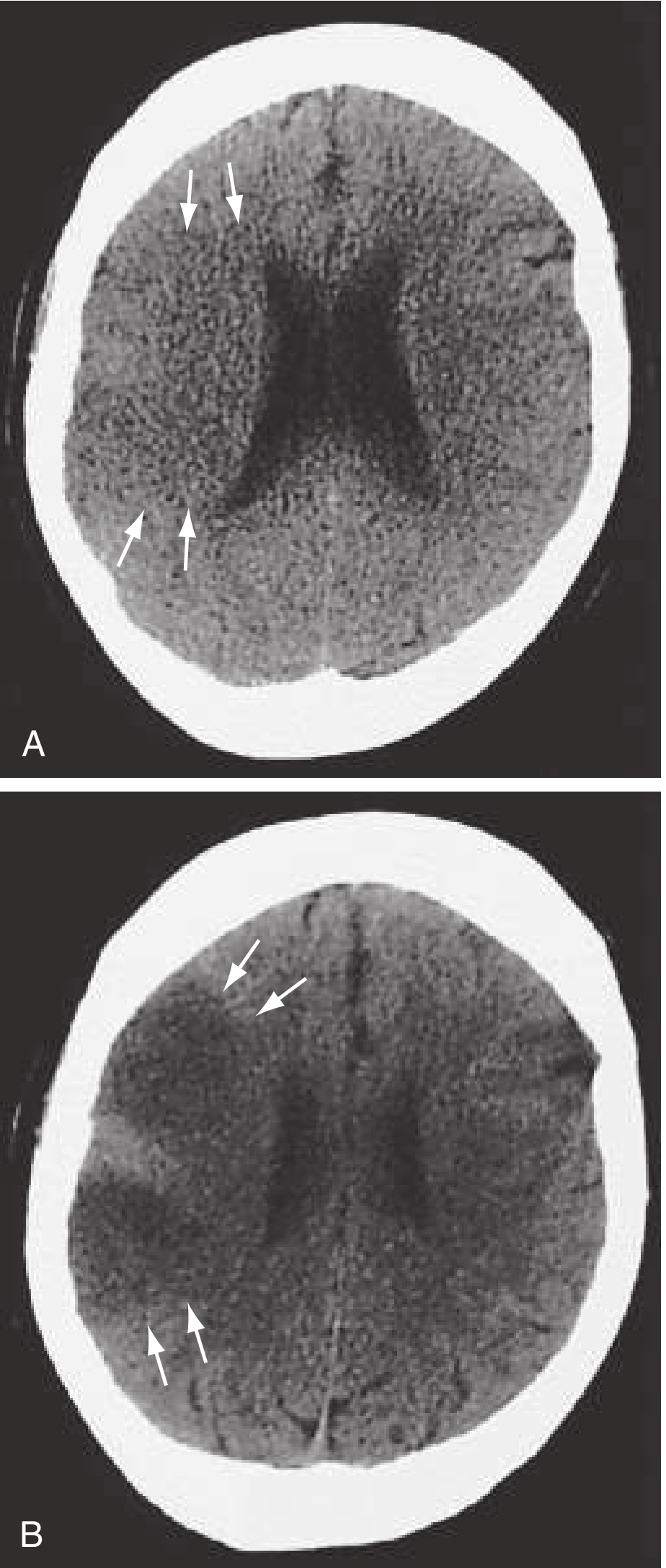
Early CT signs of ischemia (within first 3 hours, seen in up to 67% of scans):
- Hyperdense artery sign - acute thrombus visible as focal hyperdensity in MCA ("hyperdense MCA sign") or dot sign in distal vessels
- Sulcal effacement and loss of the insular ribbon
- Loss of gray-white interface
- Acute hypodensity (appears by 6-12 hours)
CT is insensitive for posterior fossa ischemia (streak artifact at skull base). Only acute hypodensity and mass effect are associated with increased hemorrhagic transformation risk after thrombolysis. - Rosen's Emergency Medicine, p. 1431-1432
Advanced Imaging
- CTA: Identifies LVO - essential for mechanical thrombectomy triage. Also detects dissection and stenosis.
- CT Perfusion (CTP): Identifies penumbra vs. core; most useful for extended time windows (6-24h). Should NOT delay tPA.
- MRI DWI with ADC mapping: Most sensitive for acute ischemia - detects restricted diffusion within minutes of onset. ADC helps distinguish true diffusion restriction from T2 shine-through. - Bradley and Daroff's Neurology, p. 701
NIHSS Scoring
The National Institutes of Health Stroke Scale (NIHSS) quantifies deficits and guides treatment eligibility. A single low score may be insufficient; serial NIHSS should be performed for evolving strokes.
Emergency Management
ABCs and Supportive Care
- Withhold oral intake until swallowing assessment (aspiration risk)
- Treat fever aggressively (even mild hyperthermia worsens neurologic injury; target normothermia)
- Correct hypoglycemia/hyperglycemia
- Cardiac monitoring for AF detection
Blood Pressure Management
| Scenario | Target | Agents |
|---|---|---|
| No thrombolysis indicated | Treat only if SBP >220 or DBP >120 or MAP >130 mmHg | Oral or parenteral agents |
| Prior to tPA/thrombectomy | SBP ≤185, DBP ≤110 mmHg | IV labetalol 10-20mg; nicardipine 5mg/h infusion; clevidipine 1-2mg/h |
| After tPA (first 24h) | SBP <180, DBP <105 mmHg | Aggressive monitoring q15min x2h, then q30min x6h, then q1h x16h |
| Hypotension | Correct with fluids; vasopressors if needed | Maintain cerebral perfusion |
- Rosen's Emergency Medicine, p. 1433-1434
Reperfusion Therapy
IV Thrombolysis
Alteplase (tPA):
- Dose: 0.9 mg/kg IV (max 90 mg); 10% as bolus over 1 min, remainder over 60 min
- Time window: within 4.5 hours of clearly defined symptom onset
- Approved by FDA; remains standard of care based on NINDS trial
- ENCHANTED trial showed low-dose (0.6 mg/kg) non-inferior with fewer sICH events - currently standard only in Japan; AHA/ASA still recommends 0.9 mg/kg
- Symptomatic ICH rate: ~6.4% in treated patients
Tenecteplase:
- Dose: 0.25 mg/kg IV (max 25 mg) as a single bolus - easier to administer
- Moderate-high quality evidence of non-inferiority to alteplase for functional outcome and sICH at 90 days
- EXTEND-IA TNK trial: tenecteplase showed higher reperfusion rates and better functional outcomes vs. alteplase when used before endovascular therapy
- Can be used in place of alteplase for patients also eligible for mechanical thrombectomy
- Rosen's Emergency Medicine, p. 1435
Mechanical Thrombectomy (Endovascular)
- Indicated for LVO in anterior circulation (ICA, MCA M1/M2)
- Standard time window: up to 24 hours with appropriate imaging selection (CTP or DWI/PWI mismatch)
- Key trials: MR CLEAN, DAWN, DEFUSE-3 established benefit
- A recent meta-analysis (2025) confirms thrombectomy benefit even in large ischemic core strokes
- Prior tPA should not be delayed in eligible patients who will proceed to thrombectomy
- BP target pre-thrombectomy (without prior tPA): ≤185/110 mmHg
Secondary Prevention
Antithrombotic therapy:
| Drug | Indication |
|---|---|
| Aspirin | All non-cardioembolic ischemic stroke/TIA |
| Clopidogrel | Alternative to aspirin; may be combined short-term after minor stroke/TIA (POINT/CHANCE trials) |
| Aspirin + extended-release dipyridamole | Non-cardioembolic prevention |
| DOACs (apixaban, rivaroxaban, dabigatran, edoxaban) | AF-related stroke (superior to warfarin for non-valvular AF) |
| Warfarin | Valvular AF or when DOACs not feasible |
| Heparin/LMWH | NOT indicated for acute ischemic stroke (negative evidence) |
Note: Glycoprotein IIb/IIIa antagonists and unfractionated heparin have negative evidence for cerebral ischemia prevention. - Bradley and Daroff's Neurology, Table 65.5
Carotid revascularization:
- Carotid endarterectomy (CEA) or stenting for symptomatic high-grade (>70%) carotid stenosis
- ESO guidelines (2024) address patent foramen ovale (PFO) closure after cryptogenic stroke
Risk factor modification: Hypertension control, statin therapy, diabetes management, smoking cessation, AF anticoagulation, lifestyle modifications
Key Stroke Mimics to Exclude Immediately
- Hypoglycemia - check glucose first in every patient
- Todd's paralysis - history of seizure
- Subdural hematoma - history of falls, anticoagulant use
- Wernicke encephalopathy - thiamine deficiency (give thiamine first)
Summary of Time-Critical Actions
| Time | Action |
|---|---|
| 0-10 min | Triage, ABCs, glucose, NIHSS |
| 0-25 min | Non-contrast CT head |
| 0-45 min | CTA (LVO screening) |
| ≤60 min | IV alteplase/tenecteplase if eligible ("door-to-needle") |
| ≤90 min (LVO) | Transfer/activate endovascular suite |
Key recent evidence:
- Thrombectomy for large ischemic core: Liu et al., Neurology 2025 (PMID 40245349) - systematic review/meta-analysis confirms benefit from EVT even in large-core strokes
- PFO after cryptogenic stroke: ESO Guidelines 2024 (PMID 38752755) - closure recommended in selected patients <60 years
- Chinese 2024 reperfusion guidelines: Xiong et al. 2025 (PMID 39832918) - tenecteplase recommended as an option over alteplase given ease of administration and non-inferiority data
Sources: Rosen's Emergency Medicine (9th ed.) | Bradley and Daroff's Neurology in Clinical Practice (8th ed.) | Plum and Posner's Diagnosis and Treatment of Stupor and Coma
This is a shared conversation. Sign in to Orris to start your own chat.