Excellent. Now let me synthesize the updated clinical picture with these new findings.
Updated Localization — Critical Pivot
The new findings fundamentally expand and redirect the diagnosis:
| New Sign | What it Tests | Localizes to |
|---|
| Romberg positive | Proprioception / posterior column integrity | Posterior columns (dorsal funiculus) |
| Dysdiadochokinesia | Rapid alternating movements | Ipsilateral cerebellum (right side if bilateral hands tested) |
| Gait ataxia | Cerebellar vermis OR posterior columns | Cerebellum / dorsal columns |
| Undershooting (R UL) on finger-nose | Past-pointing = cerebellar dysmetria | Right cerebellar hemisphere |
Parsing Romberg vs. Cerebellar Ataxia
| Feature | Romberg-positive (Sensory) Ataxia | Cerebellar Ataxia |
|---|
| Eyes open | Compensates — walks better | Still ataxic — no compensation |
| Eyes closed | Falls (Romberg +ve) | No significant worsening |
| Gait character | Stamps feet, wide-based | Wide-based, lurching, titubation |
| Finger-nose | Normal (if eyes open) | Dysmetric regardless |
| Romberg test | Positive | Negative/mild |
This patient has BOTH:
- Romberg +ve → posterior column (proprioceptive) involvement
- Dysdiadochokinesia + undershooting (right UL) → right cerebellar hemisphere involvement
Revised Localization: Multi-System / Combined Tract Disease
The complete picture now spans three systems simultaneously:
1. Posterior Columns (Dorsal Funiculi)
- Romberg positive
- Paresthesia feet (4 years — earliest symptom, now explained)
- Sensory (proprioceptive) gait ataxia
2. Lateral Columns (Corticospinal Tracts)
- Extensor plantars (bilateral)
- Increased UL tone
- LL weakness (4+/4+)
- Bladder frequency (UMN bladder)
3. Cerebellar pathways (or spinocerebellar tracts)
- Dysdiadochokinesia
- Right-sided dysmetria (undershooting on F-N test)
- Gait ataxia
4. Anterior Horn / Nerve Root (LMN component)
- Absent knee jerks (bilateral) — L3–L4 LMN
This Is Now a Combined System Degeneration Picture
The combination of posterior column + lateral column + cerebellar involvement + LMN features in a chronic, progressive, bilateral, symmetric pattern with paresthesia as the earliest symptom points strongly to:
TOP DIAGNOSIS: Subacute Combined Degeneration (SCD) of the Spinal Cord
Due to Vitamin B12 (Cobalamin) Deficiency
"SCD represents the most common form of metabolic myelopathy. Vitamin B12 deficiency results in demyelination and eventually degeneration of the lateral and dorsal columns of the spinal cord."
— Bradley and Daroff's Neurology in Clinical Practice
"Subacute combined degeneration of the spinal cord is caused by deficiency of vitamin B12 and is marked by degeneration of the ascending and descending spinal tracts."
— Robbins & Kumar Basic Pathology
Why the Name "Subacute Combined Degeneration"?
- Posterior columns degenerate → sensory ataxia, Romberg +ve, paresthesia
- Lateral columns (corticospinal tracts) degenerate → UMN signs (extensor plantars, spasticity, bladder)
- "Combined" = both posterior AND lateral column involvement
Why the Cerebellar Signs?
In SCD/B12 deficiency:
- Demyelination extends to spinocerebellar tracts → cerebellar-type features
- Peripheral neuropathy co-exists (explains absent knee jerks — LMN component)
- The gait ataxia in SCD is a combination of sensory (proprioceptive) + cerebellar + motor deficit
Reconciling All Findings in SCD
| Finding | Explained by SCD |
|---|
| Paresthesia both feet × 4 yrs (earliest) | Posterior column + peripheral neuropathy |
| Absent knee jerks (bilateral) | Peripheral neuropathy (LMN) |
| Extensor plantars | Lateral column (corticospinal) degeneration |
| Increased UL tone | Corticospinal tract involvement |
| Romberg positive | Posterior column loss |
| Dysdiadochokinesia | Spinocerebellar tract involvement |
| Dysmetria right UL | Cerebellar pathway demyelination |
| Gait ataxia | Multi-component: sensory + cerebellar + motor |
| Bladder frequency | UMN bladder (lateral column) |
| Proximal LL weakness | Corticospinal tract weakness |
| Foot drop (slipping slippers) | Peripheral neuropathy + foot dorsiflexion weakness |
The Absent Knee Jerk + Extensor Plantar Combination
This is the classic paradox of SCD:
- Normally, UMN lesions produce hyperreflexia
- In SCD, the peripheral neuropathy abolishes the reflexes while the corticospinal tract lesion gives extensor plantars
- Result: absent/reduced DTRs + Babinski sign = pathognomonic of combined system disease
"In Friedreich ataxia and related forms of spinocerebellar degeneration, subacute combined degeneration of the spinal cord (vitamin B12 deficiency) ... [sensory tabetic gait is seen]" — Adams & Victor's Neurology
Differential Diagnosis (Updated)
| Diagnosis | Fit | Missing |
|---|
| SCD (B12 deficiency) | ✅ All features explained: posterior + lateral columns + peripheral neuropathy + cerebellar | Dietary history, macrocytic anemia |
| Friedreich's Ataxia | Absent knee jerks, cerebellar, posterior column, extensor plantars | Onset usually childhood/adolescence, pes cavus, scoliosis, family history; no bladder usually |
| Multiple Sclerosis | Multi-system, bladder, cerebellar | Typically relapsing-remitting, younger, optic neuritis; not this insidious progressive course without relapses |
| Spinocerebellar Ataxia (SCA) | Cerebellar + posterior column features | Would not fully explain absent K + extensor plantars + bladder |
| Compressive conus + separate cerebellar pathology | Possible but requires 2 diagnoses | Less parsimonious |
Revised Diagnostic Priority
Single unifying diagnosis: Subacute Combined Degeneration of the spinal cord (Vitamin B12 deficiency)
Immediate Investigations
Confirmatory (first priority):
- Serum Vitamin B12 — may be low, but can be normal even with deficiency
- Serum methylmalonic acid (MMA) + homocysteine — elevated even when B12 borderline; most sensitive markers
- CBC + peripheral smear — macrocytic anemia, hypersegmented neutrophils (may be absent if concurrent iron deficiency)
- Serum folate — folate deficiency can cause similar but less severe picture
Identifying the cause of B12 deficiency:
5. Anti-parietal cell antibodies + anti-intrinsic factor antibodies → pernicious anemia
6. Serum gastrin — elevated in atrophic gastritis / pernicious anemia
7. Upper GI endoscopy with biopsy — atrophic gastritis
8. Dietary history — strict vegetarianism/veganism (common cause in South Asian populations)
9. Schilling test (rarely done now) — absorption defect
Neuroimaging:
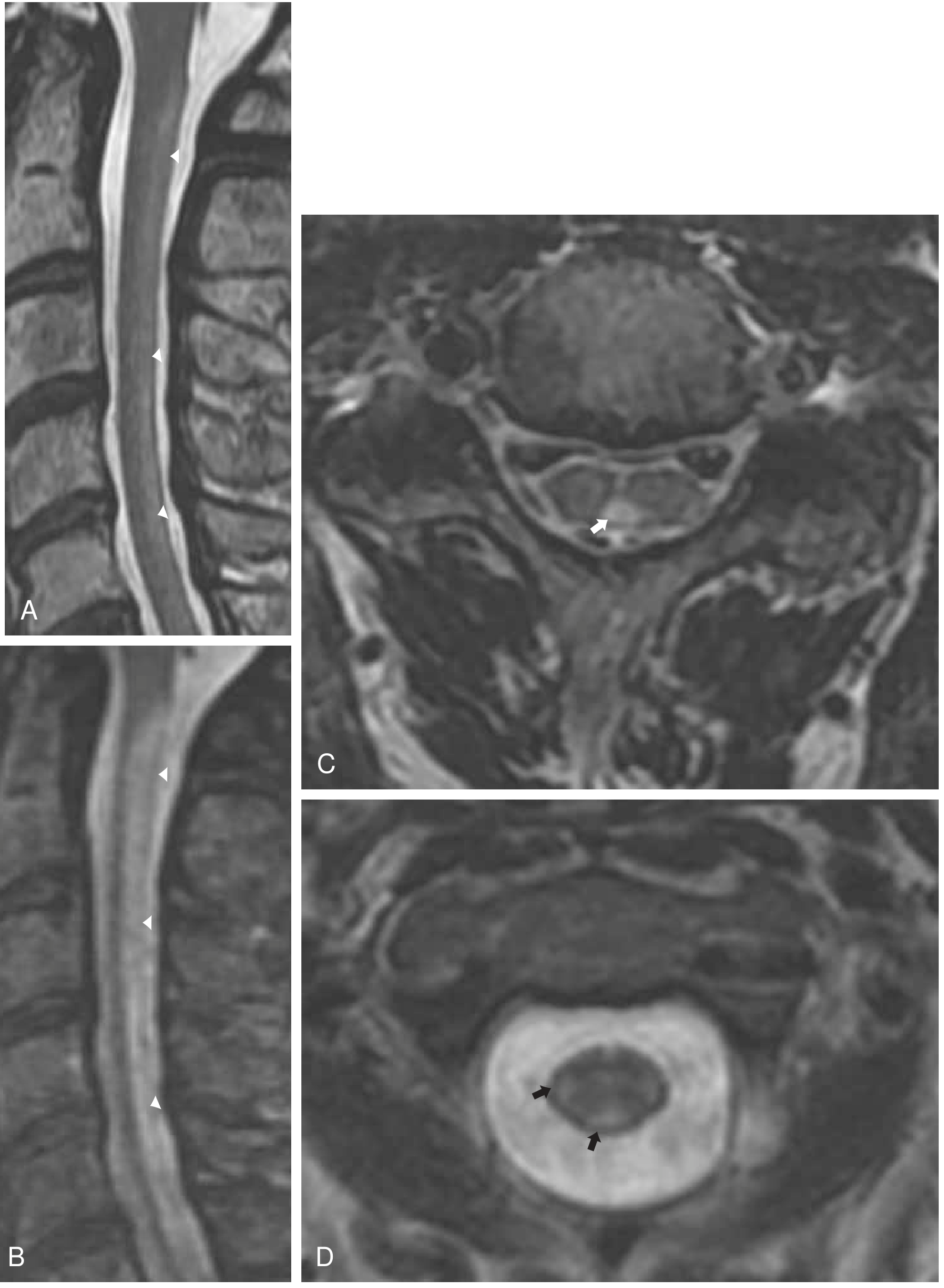
10. MRI spine (T2) — "inverted V" or "inverted U" sign: symmetric T2 hyperintensity in posterior and lateral columns, most prominent in the cervical/thoracic cord; does not enhance with gadolinium
Other:
- LFTs, TFTs (hypothyroidism can contribute)
- Serum protein electrophoresis (myeloma causing malabsorption)
MRI Finding in SCD
"On T2-weighted images, hyperintense signal change is seen, typically involving the dorsal columns, sometimes also the lateral columns ... T1 may reveal hypointensity in the dorsal columns."
— Bradley and Daroff's Neurology
The characteristic MRI sign is the "inverted V" sign on axial T2 — bilateral posterior column hyperintensity.
T2-weighted MRI in SCD showing longitudinal hyperintensity in the posterior columns — Bradley and Daroff's Neurology
Treatment (if B12 deficiency confirmed)
- IM Hydroxocobalamin (preferred) or cyanocobalamin: loading doses daily × 1 week, then weekly × 4 weeks, then monthly for life (if pernicious anemia/malabsorption)
- If dietary deficiency only: high-dose oral B12 1000–2000 μg/day is effective
- Neurological improvement begins within weeks but may take months; recovery is incomplete if delayed
- Do NOT give folate alone without B12 (worsens neurological picture)
Summary
The addition of Romberg +ve, dysdiadochokinesia, gait ataxia, and right-sided dysmetria transforms this from a pure conus/structural diagnosis to a metabolic combined system degeneration. The single most parsimonious diagnosis is Subacute Combined Degeneration of the spinal cord due to Vitamin B12 deficiency — which elegantly unifies every finding: 4-year paresthesia, absent knee jerks, extensor plantars, bladder symptoms, posterior column loss, cerebellar features, and progressive disability leading to job loss.
Stat investigation: Serum B12, MMA, homocysteine, CBC with smear, MRI spine.