Ecg changes in copd
Reading File
Finding Sources
Finding Sources
Searching the Web
ECG changes in COPD electrocardiogram findings
Finding Sources
Finding Sources
Searching Images
ECG changes in COPD chronic obstructive pulmonary disease electrocardiogram
Reading File
Searching Images
P pulmonale right axis deviation low voltage ECG emphysema cor pulmonale
Reading Web Page
ECG findings COPD emphysema P pulmonale right axis deviation low voltage multifocal atrial tachycardia
Loading Image
I now have comprehensive information to provide a thorough answer. Here is a complete, structured overview of ECG changes in COPD:
ECG Changes in COPD
ECG changes in COPD arise from two main mechanisms: mechanical effects of hyperinflation (lung overdistension displacing and rotating the heart) and hemodynamic effects on the pulmonary vasculature and right heart (cor pulmonale).
1. P-Wave Changes
P Pulmonale
- Peaked, tall P waves (>2.5 mm) in leads II, III, and aVF
- Reflects right atrial enlargement/overload from chronically elevated pulmonary pressures
- One of the most commonly reported findings in COPD studies (present in ~33% of patients)
Vertical P-wave Axis
- The frontal plane P-wave axis shifts toward vertical (>+60°), highly sensitive and specific for emphysema
- Correlates with spirometric severity (FEV₁) and CT-based emphysema scoring
- Considered among the most diagnostically useful solitary ECG criteria for COPD
Other P-wave changes
- Increased P-wave amplitude in inferior leads ("Gothic P waves")
- Increased P-terminal force in V1
- PR segment depression (due to atrial repolarization abnormalities from atrial enlargement)
2. QRS Changes
Low Voltage Complexes
- QRS amplitude <5 mm in limb leads and/or <10 mm in precordial leads
- Caused by hyperaeration acting as an insulator between the heart and recording electrodes
- Very characteristic of emphysema
Poor R-Wave Progression (PRWP)
- Diminished or absent R waves in V1–V4 (slow R-wave progression)
- Results from downward displacement of the diaphragm and heart due to lung hyperinflation
- Important: Chronic cor pulmonale from COPD does not typically produce tall right precordial R waves (as seen in other causes of RVH) — instead it shows PRWP. This is a key distinction emphasized in Harrison's:
"Chronic cor pulmonale due to obstructive lung disease usually does not produce the classic ECG patterns of right ventricular hypertrophy noted above. Instead of tall right precordial R waves, emphysema is more typically associated with diminished r waves in right to mid-precordial leads (slow R-wave progression) due in part to downward displacement of the diaphragm and the heart." — Harrison's Principles of Internal Medicine, 22nd Ed.
Right Axis Deviation (RAD)
- The most common ECG abnormality in some series (present in ~41% of patients)
- QRS axis >+90° in the frontal plane
- Worsens with disease severity — present in 82% of very severe (GOLD Stage 4) COPD
S1S2S3 Pattern
- Persistent S waves in leads I, II, and III
- Reflects clockwise cardiac rotation from right heart enlargement and diaphragmatic depression
Lead I Sign
- Small or absent R wave + prominent S wave in lead I (vertical heart/axis)
Right Bundle Branch Block (RBBB)
- Complete or incomplete RBBB may develop with right ventricular pressure overload
3. Repolarization Changes
ST-T Wave Abnormalities
- ST-segment and T-wave changes (often called "sagging PR and ST segments")
- PR segment depression particularly characteristic
- T-wave inversions in right precordial leads (V1–V3) with RVH
Right Ventricular Hypertrophy (RVH) Pattern
- When cor pulmonale develops: dominant R wave in V1, deep S in V5/V6, right axis deviation
- Present in ~36% of COPD patients overall; much more common in severe/very severe disease
4. Arrhythmias
Multifocal Atrial Tachycardia (MAT)
- Pathognomonic association with COPD and hypoxia
- Irregular, narrow-complex tachycardia with ≥3 distinct P-wave morphologies
- Driven by hypoxia, hypercapnia, catecholamines, and theophylline toxicity
- Rate typically 100–180 bpm
Sinus Tachycardia
- Common — due to hypoxia, dyspnea, or bronchodilator therapy (β₂-agonists)
Atrial Fibrillation / Atrial Flutter
- Increased prevalence compared to general population
- Related to right atrial dilatation and hypoxemia
Other Atrial Arrhythmias
- Atrial tachycardia, PACs common with severe disease
5. Correlation with COPD Severity (GOLD Stages)
| GOLD Stage | % with ECG Abnormalities | Common Findings |
|---|---|---|
| Mild (Stage 1) | ~17–20% | Vertical P-axis, mild RAD |
| Moderate (Stage 2) | ~43% | P pulmonale, low voltage, PRWP |
| Severe (Stage 3) | ~60% | RVH pattern, RAD, PRWP |
| Very Severe (Stage 4) | ~78–88% | RVH, RAD, low voltage, MAT, arrhythmias |
ECG changes correlate strongly with FEV₁, hyperinflation on CT, and pulmonary artery pressures.
ECG Example — COPD with Cor Pulmonale
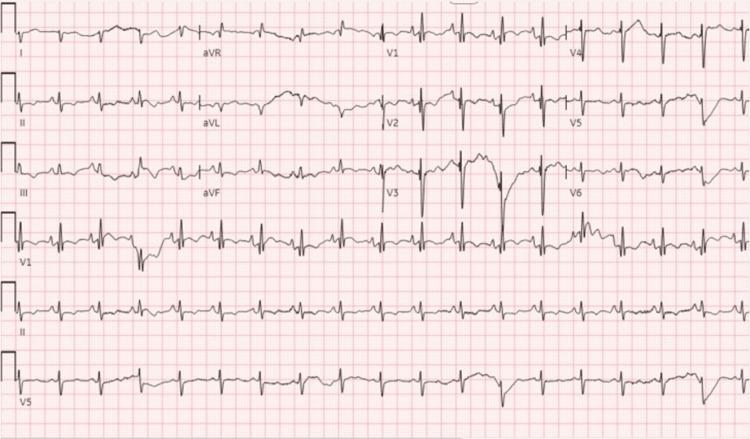
12-lead ECG showing sinus tachycardia with right axis deviation, P-pulmonale (peaked P waves inferiorly), right ventricular hypertrophy pattern (tall R in V1, deep S in lateral leads), and low lateral lead voltage — classic features of COPD with cor pulmonale.
Summary Table
| Category | Finding | Mechanism |
|---|---|---|
| P-wave | P-pulmonale, vertical P-axis, PR depression | RA enlargement, atrial stretch |
| QRS axis | Right axis deviation | RV enlargement, clockwise rotation |
| QRS amplitude | Low voltage | Hyperinflation as insulator |
| Precordial | Poor R-wave progression | Diaphragm/heart displacement |
| RVH | Only in severe disease; often absent tall R in V1 | Atypical RVH pattern in COPD |
| Conduction | Incomplete/complete RBBB | RV pressure overload |
| Arrhythmia | MAT (classic), AF, sinus tachycardia | Hypoxia, catecholamines, atrial enlargement |
| Repolarization | ST sagging, T inversions V1–V3 | RV strain, repolarization abnormality |
Key clinical point: The ECG in COPD is routinely ordered during exacerbation assessment alongside ABG, SpO₂, and CXR — it helps identify coexisting ischemia, arrhythmias, and degree of right heart strain.
This is a shared conversation. Sign in to Orris to start your own chat.