Chalazoin
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a thorough overview of chalazion based on multiple ophthalmology and primary care textbooks.
Chalazion (Meibomian Cyst)
Definition
A chalazion is a sterile, chronic granulomatous inflammatory lesion (lipogranuloma) of the meibomian gland (or occasionally the gland of Zeis), caused by obstruction and retention of lipid-rich sebaceous secretions within the eyelid. It is distinct from a hordeolum (stye), which is an acute bacterial abscess.
- Goldman-Cecil Medicine, p. 302
- Wills Eye Manual, p. 381
Pathogenesis
The retained lipid-rich material acts as a foreign body, triggering a lipogranulomatous foreign-body inflammatory reaction. Histopathology shows:
- Extracellular fat deposits (appear as clear spaces after processing dissolves the fat)
- Lipid-laden epithelioid cells and multinucleated giant cells
- Surrounding lymphocytes
Histopathology - lipogranuloma:
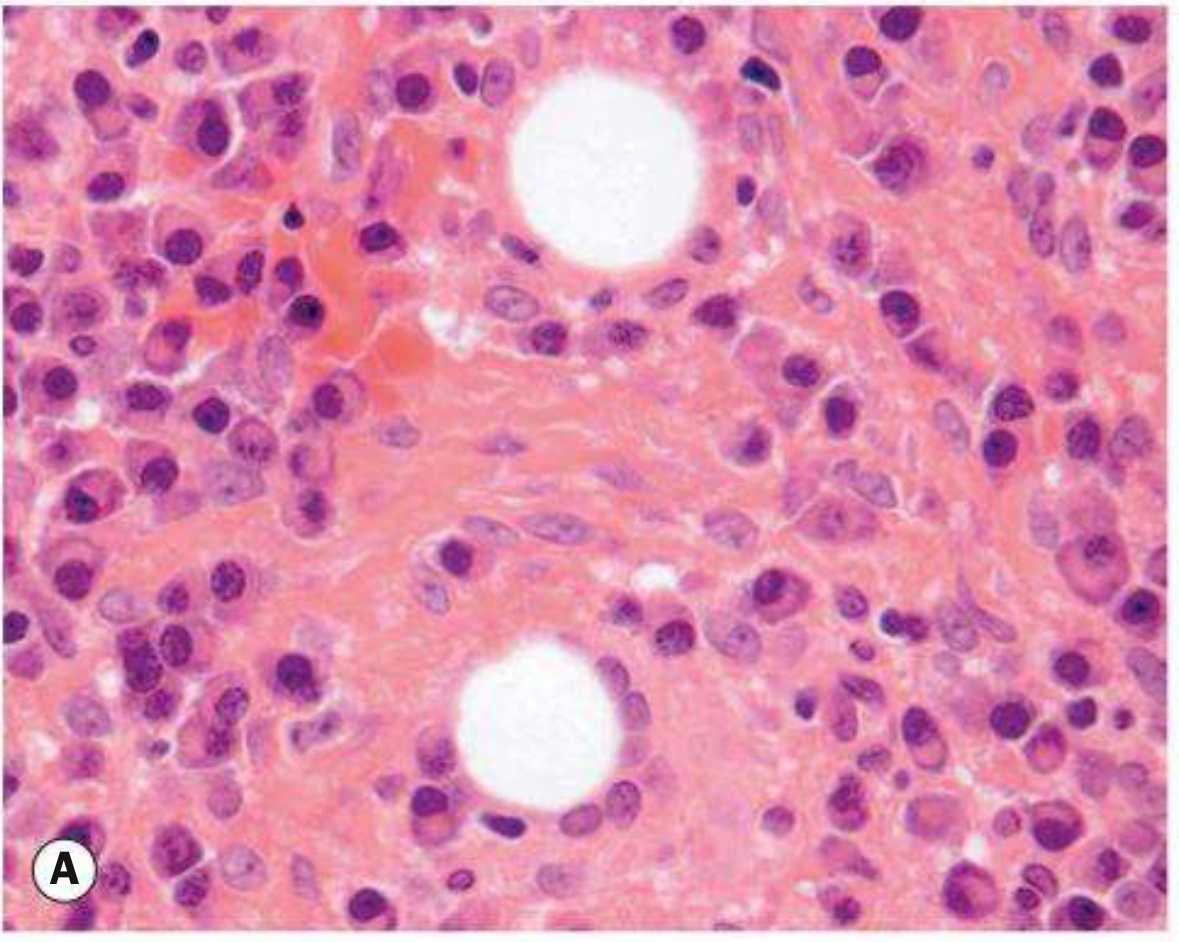
- Kanski's Clinical Ophthalmology 10th ed., p. 54
Associated conditions:
- Blepharitis (commonly present)
- Acne rosacea (associated with multiple/recurrent chalazia)
- Bortezomib (proteasome inhibitor used in myeloma) can predispose to chalazia within 3 months of starting treatment
Key warning: A recurrent chalazion in the same lid position - especially in older patients - must be biopsied to exclude sebaceous carcinoma masquerading as a chalazion.
Clinical Features
Bilateral chalazia in upper eyelids (clinical photo):

Symptoms
- Gradual onset of a painless or mildly tender eyelid lump (subacute/chronic form)
- Acute form: localized cellulitis and sterile inflammation; if secondarily infected, becomes an internal hordeolum
Signs
| Feature | Description |
|---|---|
| Critical | Well-defined, palpable subcutaneous nodule within the tarsal plate |
| Meibomian gland | Blocked orifice, inspissated secretions may be visible |
| Associated | Eyelid swelling, erythema, focal tenderness, blepharitis, acne rosacea |
| Possible | Conjunctival granuloma, or lesion pointing/draining mucopurulent material |
Differential Diagnosis
| Condition | Key distinguishing feature |
|---|---|
| Hordeolum (stye) | Acute, painful, bacterial; external (gland of Zeis) or internal (meibomian gland) |
| Sebaceous carcinoma | Recurrent chalazion same spot; madarosis, eyelid thickening, chronic unilateral blepharitis in older patient |
| Preseptal cellulitis | Diffuse eyelid/periorbital erythema, edema, warmth |
| Pyogenic granuloma | Deep-red, pedunculated conjunctival lesion, often post-chalazion/surgery |
| Forniceal foreign body | Eyelid swelling, history of contact lens use or trauma |
- Wills Eye Manual, p. 382
Workup
- History - prior chalazia, ocular surgery, trauma, medications (bortezomib)
- External examination - palpate eyelid for nodule; inspect for madarosis or ulceration
- Slit lamp - evert eyelid, evaluate meibomian gland inspissation; assess for signs suggesting malignancy
- Screen for rosacea (look at skin, check for telangiectasias)
Treatment
Step 1 - Conservative (first-line)
- Warm compresses for at least 10 minutes 4x daily with gentle massage over the lesion
- At least 1/3 resolve spontaneously - observation alone is appropriate if improving
- Expression: compression between two cotton-tipped applicators can express contents of a fresh, superficial lesion
Step 2 - Medications
- Topical antibiotic/steroid (e.g., neomycin/polymyxin B/dexamethasone ointment b.i.d. for 1-2 weeks)
- Doxycycline 20-50 mg orally daily to b.i.d. (low-dose, for its anti-inflammatory effect) - indicated for multiple/recurrent chalazia or associated ocular rosacea
Step 3 - If no resolution after 3-4 weeks: Choose one
A. Intralesional steroid injection
- Triamcinolone acetonide 40 mg/mL mixed 1:1 with 2% lidocaine with epinephrine (0.2-1.0 mL)
- Alternatives: betamethasone or dexamethasone formulations
- ~80% success rate with one injection; can repeat 1-2 weeks later
- Preferred for marginal lesions or lesions near the lacrimal punctum
- Risks: skin depigmentation and fat atrophy (less common via conjunctival approach); rare retinal vascular occlusion from retrograde intra-arterial infiltration - discuss with patient before use
B. Incision and curettage (I&C) - surgical
- Administer local anesthesia; evert the eyelid with a specialized chalazion clamp
- Incise vertically through the tarsal plate
- Curette the cyst contents; excise solid inflammatory material with fine scissors if needed
- No suture required
- Apply topical antibiotic 3x daily for 5 days post-procedure
- All excised tissue (especially recurrent or atypical chalazia) should be sent for histopathology
Follow-Up
- If medical therapy is used: review only if lesion persists beyond 3-4 weeks
- After I&C: re-examine as needed
- Recurrent chalazion at the same site = biopsy mandatory to rule out malignancy (sebaceous carcinoma)
Sources: Kanski's Clinical Ophthalmology 10th ed. | Wills Eye Manual | Goldman-Cecil Medicine | Textbook of Family Medicine 9e
This is a shared conversation. Sign in to Orris to start your own chat.