Osteoarthritis knee clinical features
Reading File
Finding Sources
Finding Sources
Searching PubMed
"knee osteoarthritis"[MeSH Terms] AND "clinical features"
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive review of the clinical features of knee osteoarthritis, drawn from Harrison's (22nd ed.), Goldman-Cecil Medicine, and Robbins Pathology.
Osteoarthritis of the Knee — Clinical Features
Epidemiology
Symptomatic knee OA affects ~12% of persons aged ≥60 and 6% of all adults ≥30 in the United States. The lifetime risk is ~40% in men and ~47% in women, rising to 60% in those above a healthy weight. Knee OA accounts for approximately 85% of the total global burden attributable to OA. Prevalence rises sharply between ages 50 and 75 and is substantially more common in women than men in middle-aged and elderly groups. — Harrison's Principles of Internal Medicine 22E
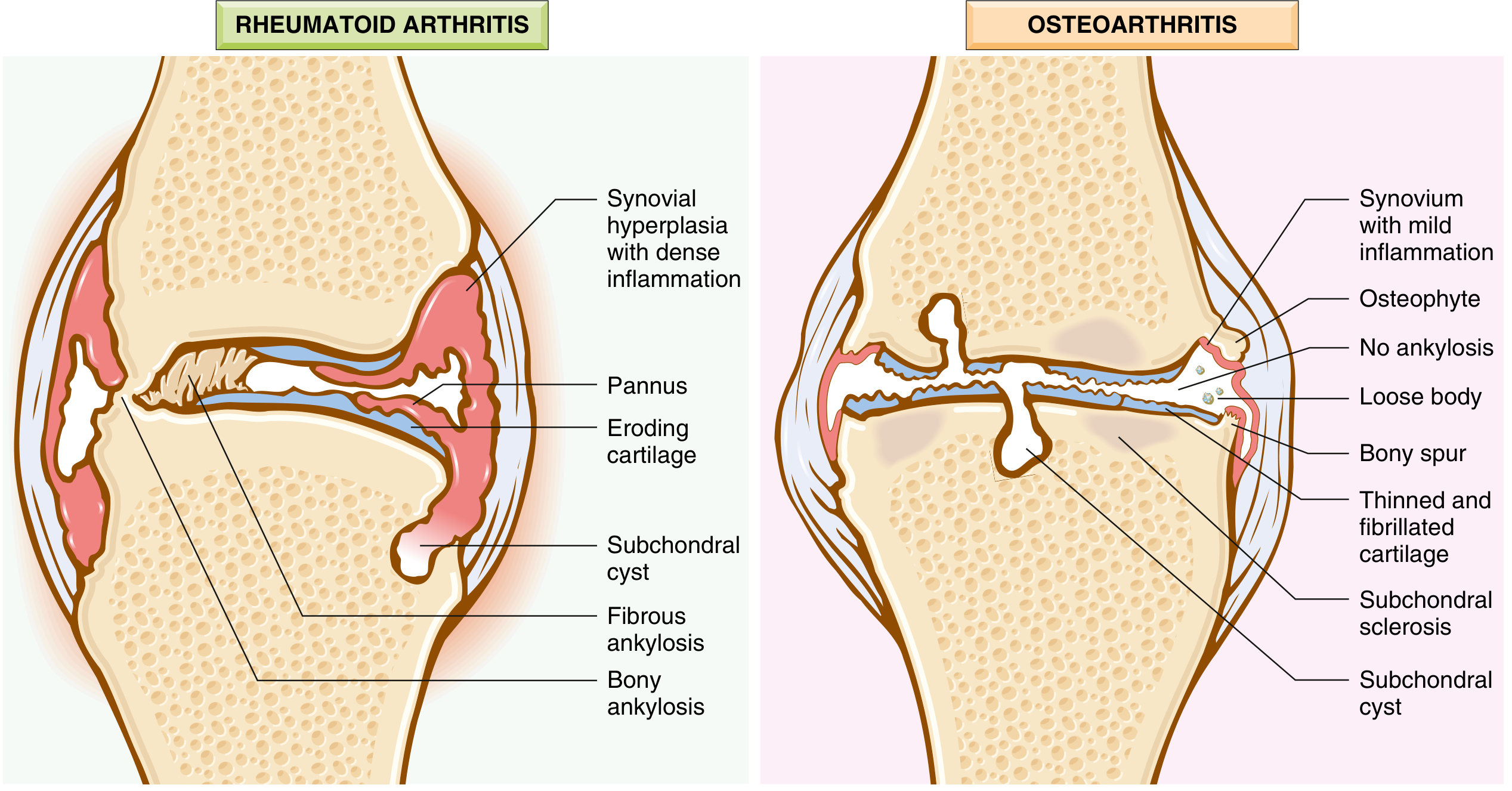
Pathological Background (What Drives the Symptoms)
The joint changes that underlie clinical features include:
- Cartilage loss — focal fibrillation, erosions, and eventual full-thickness ulceration
- Subchondral bone sclerosis — thickening and eburnation (ivory-like polished surface where cartilage is lost)
- Osteophyte formation — bony outgrowths at joint margins
- Meniscal degeneration — integral to knee OA
- Synovitis — mild-to-moderate, with macrophage infiltration and cytokine release
- Subchondral cysts — formed by synovial fluid forced through microfractures (ball-valve mechanism)
- Capsular stretching and fibrosis
- Periarticular muscle weakness — especially quadriceps
Symptoms
1. Pain (cardinal feature)
- Mechanically driven: occurs with or just after joint use; typically worse toward the end of the day
- Activity-specific examples: stair climbing, arising from a chair (patellofemoral compartment, active >35° flexion), walking, prolonged standing
- Early disease: episodic — triggered by overuse, resolves with rest
- Advanced disease: continuous pain, present at rest, nocturnal pain
- Patellofemoral pain: predominates with knee bending activities; pain with squatting or descending stairs
2. Morning stiffness
- Usually brief: <15–30 minutes (contrast with RA where >1 hour is typical)
- Also present as "gelling" — stiffness after any period of inactivity that loosens with movement
3. Crepitus
- Audible and/or palpable grating or clicking during joint movement
- Most prominent under the patella on flexion and extension
- Results from irregular articular surfaces
4. Mechanical symptoms
- Buckling / giving way — from quadriceps weakness and/or ligamentous laxity; associated with falls
- Catching / locking — may reflect loose bodies (joint mice) or meniscal pathology; requires further evaluation only if arising after acute injury
5. Functional limitation
- Difficulty with stair climbing, rising from a chair, prolonged walking
- Progressive reduction in range of motion
Signs on Examination
| Sign | Detail |
|---|---|
| Joint line tenderness | Palpation along the medial or lateral joint line |
| Crepitus | Palpable on passive/active knee movement, maximal on patellofemoral compression |
| Bony enlargement | Periarticular osteophytes, palpable at joint margins |
| Joint effusion | Soft tissue swelling; synovial fluid white count usually <1000/μL (non-inflammatory) |
| Reduced range of motion | Loss of full flexion/extension |
| Deformity | Varus (most common in medial compartment disease), fixed flexion deformity, less commonly valgus |
| Malalignment | Varus → increased medial compartment loading → accelerates medial cartilage loss; valgus → lateral compartment damage |
| Muscle wasting | Quadriceps atrophy (from disuse, arthrogenous inhibition, and pain-related avoidance) |
| Instability | Ligamentous laxity testing; medial/lateral or anteroposterior instability in advanced disease |
| Peri-articular tenderness | Including pes anserine bursa region (medial, distal to joint line) |
| Patellofemoral compression pain | Reproduction of anterior knee pain on compressing patella against femur |
X-ray and MRI Findings
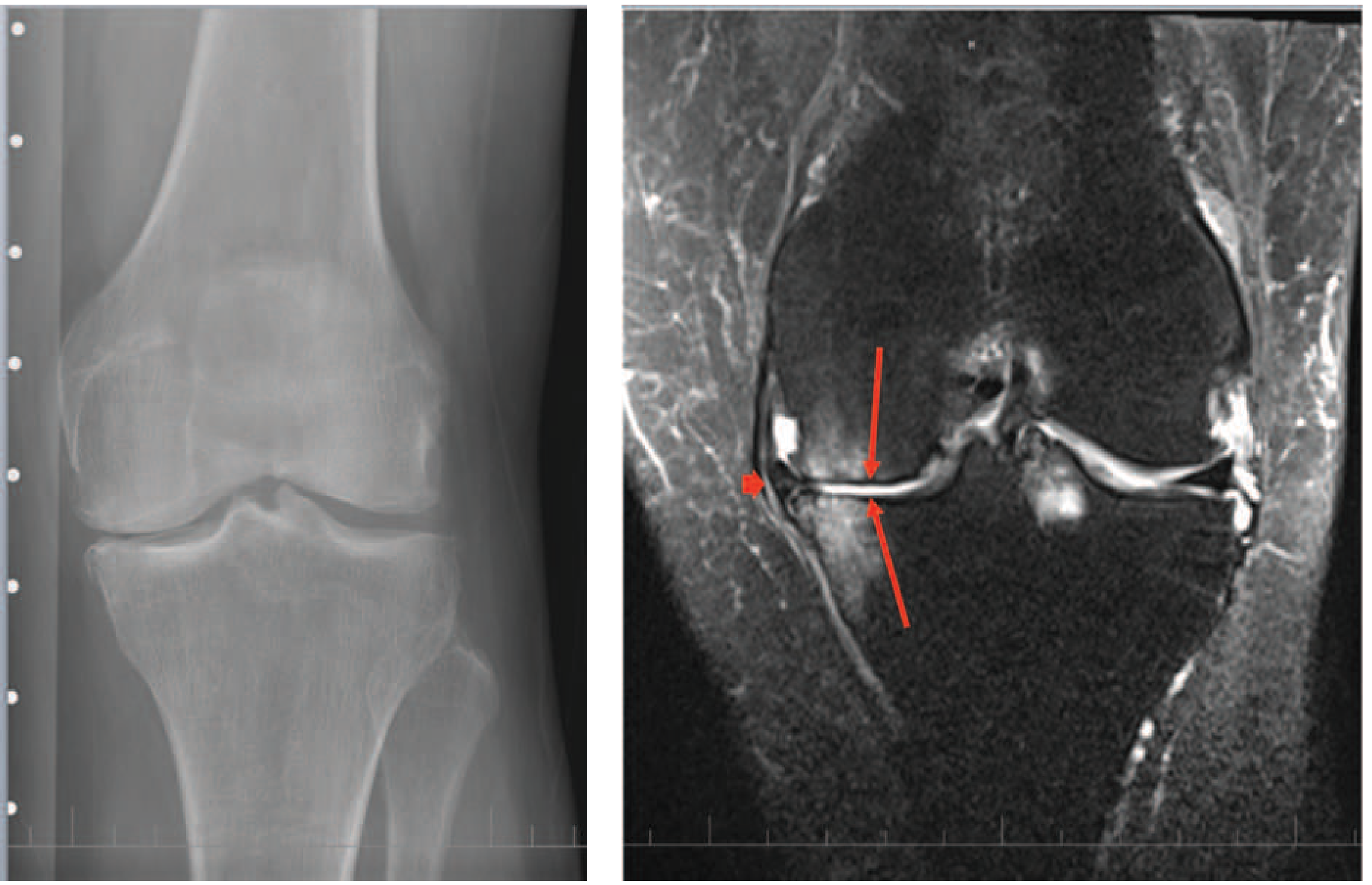
Classical radiographic features (LOSS mnemonic):
- L — Loss of joint space (asymmetric, medial > lateral in varus knee)
- O — Osteophyte formation at joint margins
- S — Subchondral sclerosis
- S — Subchondral cysts
Important: Radiographic severity correlates poorly with pain and disability. Many with advanced X-ray changes have no pain; some with severe pain show only mild X-ray changes. MRI is not routinely indicated diagnostically. — Harrison's 22E; Goldman-Cecil
Pain Sources in the Knee
Since cartilage is aneural, pain arises from innervated structures:
| Structure | Mechanism |
|---|---|
| Subchondral bone | Bone marrow edema/lesions from microcracks and trauma; stimulate bone nociceptors |
| Synovium | Mild-to-moderate synovitis; correlated with pain severity on MRI |
| Joint capsule | Capsular stretch from effusion stimulates nociceptors |
| Periarticular bursae | Pes anserine bursitis (medial, distal), iliotibial band syndrome |
| Central sensitization | Peripheral and central sensitization in advanced/chronic cases; allodynia and hyperalgesia |
Diagnosis
Diagnosis is clinical, based on:
- Pain + brief morning stiffness (<30 min) + functional limitation
- Physical signs: crepitus, restricted/painful movement, joint tenderness, bony enlargement
No blood tests are routinely indicated unless inflammatory arthritis is suspected.
Plain radiographs are not necessary for typical presentations; order only for atypical presentations or diagnostic uncertainty.
Plain radiographs are not necessary for typical presentations; order only for atypical presentations or diagnostic uncertainty.
Features suggesting an alternative diagnosis:
- Morning stiffness >30–60 minutes → consider RA
- Recent trauma → exclude fracture/internal derangement
- Hot, swollen joint → consider gout, pseudogout, septic arthritis
- Synovial fluid WBC >1,000/μL → inflammatory arthritis
- Prominent nocturnal pain in non-end-stage disease → distinct workup warranted
Clinical Phenotypes of Knee OA (Goldman-Cecil)
Knee OA is a heterogeneous syndrome with recognised phenotypes:
- Chronic pain phenotype (central sensitization prominent)
- Inflammatory phenotype (synovitis-driven)
- Metabolic syndrome phenotype (obesity, diabetes, dyslipidaemia)
- Bone and cartilage metabolism phenotype
- Mechanical overload phenotype (malalignment, occupation-related)
- Minimal joint disease phenotype (pain disproportionate to structural change)
Sources: Harrison's Principles of Internal Medicine 22E (Felson & Neogi); Goldman-Cecil Medicine (Hunter); Robbins & Kumar Basic Pathology
Examination findings osteoarthritis knee inspection, palpation and range of movements
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.