What is Tall R waves in V1–V3 * Upright T waves in V1–V3 in ecg and why
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Here is the full detailed answer:
Tall R Waves in V1-V3 + Upright T Waves in V1-V3 on ECG
These two findings are closely related and almost always point toward the same group of underlying causes. Understanding them together is more useful than treating them separately.
What Is a "Tall R Wave in V1-V3"?
Normally, V1 has a small R wave and a deep S wave (rS pattern), with the R wave growing progressively taller as you move from V1 to V5/V6 - this is called normal R-wave progression. A "tall R wave" in V1-V3 means the R wave is disproportionately large, with one or more of these criteria:
- R wave ≥ S wave in V1 (R:S ratio > 1)
- R wave ≥ 0.04 s (40 ms) in V1 and V2
- Loss of the expected small-r/deep-S pattern
What Are "Upright T Waves in V1-V3"?
Normally, T waves in V1 (and sometimes V2) are inverted or flat. Finding tall, upright (positive) T waves in V1-V3 is abnormal and often accompanies tall R waves in the same leads.
The Physiology: Why Do These Occur Together?
The right precordial leads (V1-V3) look at the anterior surface, right ventricle, and the posterior wall of the left ventricle - but from the front, so the posterior LV wall appears as a mirror image.
When V1-V3 show tall R + upright T, there are two main mechanisms:
1. Mirror-Image Effect (Reciprocal Changes) - Posterior MI
The posterior LV wall is not directly seen by standard leads. V1 and V2 sit anteriorly and record the mirror image of posterior events:
| Posterior event | What V1-V2 shows |
|---|---|
| Q wave (necrosis) | Tall R wave |
| ST elevation | ST depression |
| T-wave inversion (in recovery/chronic phase) | Upright (positive) T wave |
So tall R + upright T in V1-V2 = reciprocal image of a Q wave + T-wave inversion posteriorly.
ECG criteria for posterior MI:
- R wave ≥ 0.04 s in V1-V2
- R:S ratio ≥ 1 in V1
- Upright T wave in V1-V2
- Horizontal ST depression in V1-V2 (in acute phase)
"R wave ≥ 0.04 second in V1 and V2 and R/S ratio ≥1 with a positive T wave suggest prior posterior MI (in the absence of RV hypertrophy or RBBB)."
- Washington Manual of Medical Therapeutics
The image below from Rosen's Emergency Medicine shows the ECG pattern of acute posterior MI - note the tall R waves, horizontal ST depression (label A), and upright T wave (label C) in V2:
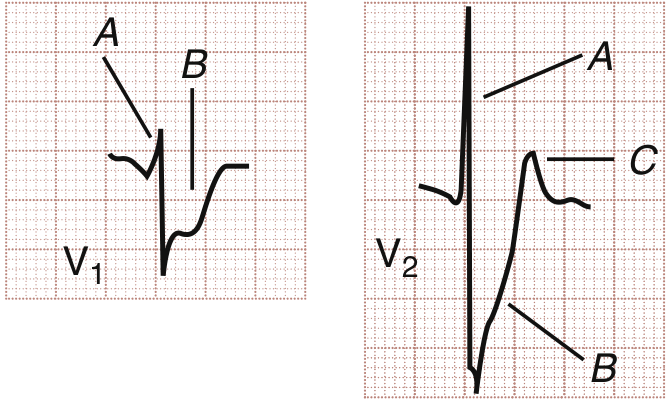
In acute posterior MI: A = ST depression, B = deep R (mirror of posterior Q), C = upright T wave (mirror of posterior T inversion)
2. Right Ventricular Hypertrophy (RVH)
In RVH due to pressure overload (pulmonary hypertension, pulmonic stenosis), the hypertrophied RV dominates V1 electrically:
- Tall R wave in V1 (R ≥ S), often with right axis deviation
- qR pattern in V1 in severe RVH
- BUT T waves are typically inverted (not upright) in V1-V3 in RVH, due to "strain" (repolarization abnormality in the overloaded muscle)
- Prominent S waves in V5-V6
"Right ventricular hypertrophy due to a sustained, severe pressure load is characterized by a relatively tall R wave in lead V1 (R ≥ S wave), usually with right axis deviation. ST depression and T-wave inversion in the right to mid-precordial leads are also often present."
- Harrison's Principles of Internal Medicine 22E
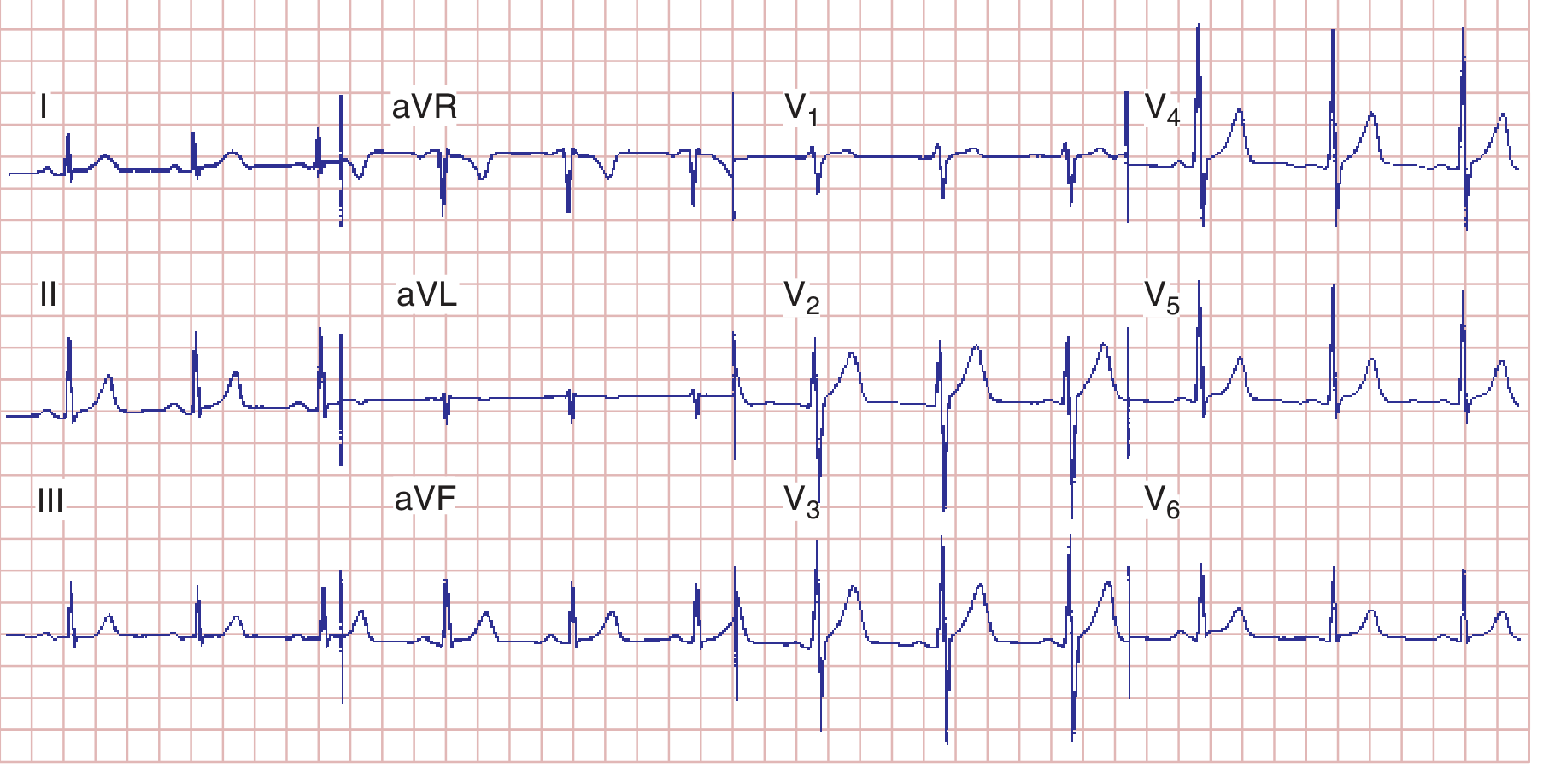
The ECG below shows RVH with early R-wave predominance in V1-V3 and T-wave inversion (strain pattern) - note this is different from posterior MI where T waves are upright:
Full Differential Diagnosis: Causes of Tall R Wave in V1-V3
| Cause | R Wave | T Wave in V1-V3 | Key Distinguishing Feature |
|---|---|---|---|
| Posterior MI (chronic) | Tall, wide, R:S > 1 | Upright | History, associated inferior/lateral changes, ST depression acutely |
| Right Ventricular Hypertrophy | Tall, R:S > 1 | Inverted (strain) | Right axis deviation, P pulmonale, clinical RV overload |
| Right Bundle Branch Block (RBBB) | RSR' (rabbit ear) pattern | Inverted (secondary) | Wide QRS >120ms, terminal S wave in I, V6 |
| Wolff-Parkinson-White (WPW) - Type A | Tall R (delta wave) | Variable | Short PR, delta wave, wide QRS |
| Hypertrophic Cardiomyopathy | May be tall | Variable | Deep septal Q waves in lateral leads, clinical picture |
| Normal variant / Early R progression | Mildly tall | Normal | No other abnormalities, normal cardiac exam |
| Duchenne Muscular Dystrophy | Tall R in V1 | Variable | Tall R + deep Q in lateral leads |
| Dextrocardia | Progressive R decrease V1 to V4 | Varies | Reversed limb leads, P axis |
"Other causes of prominent upright anteroseptal forces include right ventricular hypertrophy, ventricular preexcitation variants (Wolff-Parkinson-White syndrome), cardiomyopathies, right bundle branch block, and normal variants with early R wave progression."
- Goldman-Cecil Medicine
The Key Clinical Point: Tall R + UPRIGHT T in V1-V3
When you specifically see tall R waves with upright T waves (not inverted), the top differential narrows significantly:
- Posterior MI (most important - do not miss) - the upright T is the mirror of T-wave inversion posteriorly
- WPW Type A - delta wave, short PR, wide QRS
- Normal variant with early transition
- RBBB can occasionally have upright T in V1-V2 early in the complex
RVH typically gives inverted T waves, so if T waves are upright, posterior MI must be actively considered, especially if the patient has chest pain.
Practical Tip
When you see tall R + upright T in V1-V2:
- Get posterior leads V7-V9 - ST elevation >0.5mm confirms posterior MI with high specificity
- Check for associated inferior changes (II, III, aVF) - posterior MI often accompanies inferior or lateral STEMI
- Compare with old ECGs - new appearance of tall R in V1 is more significant than a longstanding finding
Sources:
- Rosen's Emergency Medicine, Concepts and Clinical Practice
- Harrison's Principles of Internal Medicine 22E (2025)
- Goldman-Cecil Medicine, International Edition
- Washington Manual of Medical Therapeutics
- Murray & Nadel's Textbook of Respiratory Medicine
Summaries this
Summary: Tall R Waves + Upright T Waves in V1-V3
What's Normal?
- V1 normally has a small R, deep S (rS pattern)
- T waves in V1 are normally flat or inverted
- So both findings are abnormal
Why Do They Occur? (Core Mechanism)
V1-V3 see the posterior LV wall as a mirror image. A posterior MI produces:
| Posterior Wall | V1-V2 Shows (Mirror) |
|---|---|
| Q wave | → Tall R wave |
| T-wave inversion | → Upright T wave |
Top Causes
| Cause | R Wave | T Wave | Clue |
|---|---|---|---|
| Posterior MI | Tall, R:S > 1 | Upright | ST depression acutely; get V7-V9 |
| RVH | Tall | Inverted (strain) | Right axis deviation |
| RBBB | RSR' pattern | Inverted | Wide QRS >120ms |
| WPW Type A | Tall (delta wave) | Variable | Short PR, wide QRS |
| Normal variant | Mildly tall | Normal | No other findings |
Key Takeaway
Tall R + UPRIGHT T in V1-V3 = think Posterior MI first
- RVH gives inverted T waves, not upright
- Always get posterior leads V7-V9 to confirm
- Check for associated inferior changes (II, III, aVF)
This is a shared conversation. Sign in to Orris to start your own chat.