Appendix in detail according to beliy and lovely
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from Bailey and Love's. Let me compile the full, detailed answer.
The Appendix - According to Bailey and Love's Short Practice of Surgery (28th Edition)
1. ANATOMY
General
The vermiform appendix is present only in humans, certain anthropoid apes, and the wombat. It is a blind muscular tube with mucosal, submucosal, muscular, and serosal layers. Morphologically, it is the undeveloped distal end of the large caecum found in many lower animals.
At birth, the appendix is short and broad at its junction with the caecum, but differential growth of the caecum produces the typical tubular structure by about age 2 years. During childhood, continued growth of the caecum commonly rotates the appendix into a retrocaecal but intraperitoneal position (most common). In approximately one-quarter of cases, rotation does not occur, resulting in a pelvic, subcaecal or paracaecal position.
Occasionally, the tip becomes extraperitoneal, lying behind the caecum or ascending colon. Rarely, when the caecum fails to migrate to the right lower quadrant (e.g., in intestinal malrotation), the appendix can be found near the gallbladder or even in the left iliac fossa, causing diagnostic difficulty.
Gross Anatomy
The base of the appendix is constant in position - found at the confluence of the three taeniae coli of the caecum, which fuse to form the outer longitudinal muscle coat of the appendix. This is surgically useful: gentle traction on the taeniae coli (particularly the anterior taenia) will guide the surgeon to the base of an elusive appendix.
The mesoappendix arises from the lower surface of the mesentery of the terminal ileum. The distal one-third of the appendix may be bereft of mesoappendix. In childhood, the mesoappendix is thin and transparent (vessels visible). In adults, it may become laden with fat.
The appendicular artery is a branch of the posterior caecal artery (from the ileocolic artery). It runs in the mesoappendix, is an end artery, and can easily thrombose during appendicitis, producing gangrene of the appendix. A small accessory artery runs near the base.
The length of the appendix varies from 2 cm to >20 cm (mean ~9 cm). The position of the tip is variable (see figure description below):
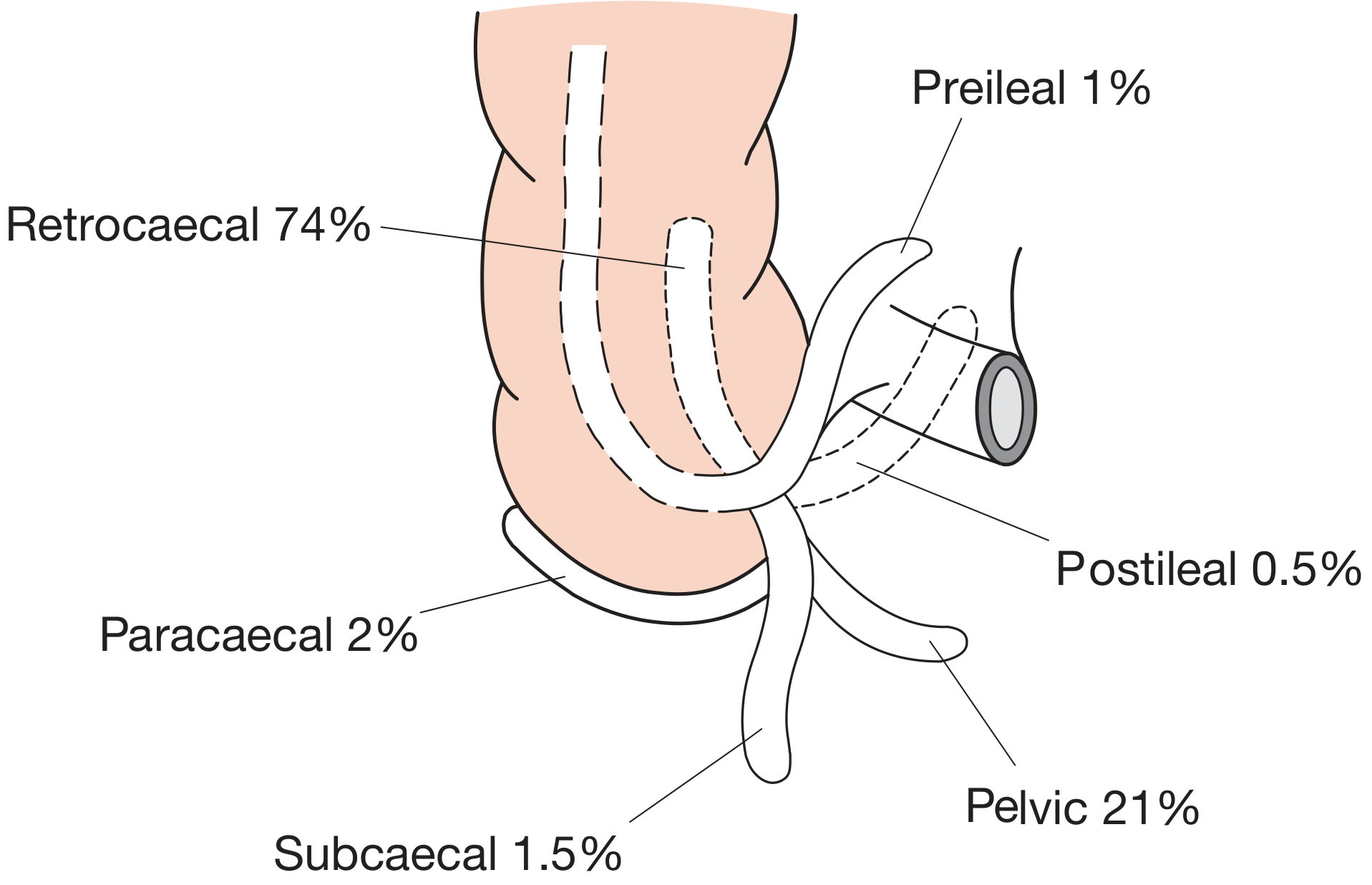
Positions of the Appendix (Wakeley's Classification)
| Position | Frequency |
|---|---|
| Retrocaecal (most common) | ~65% |
| Pelvic / descending | ~31% |
| Subcaecal | ~2% |
| Pre-ileal | ~1% |
| Post-ileal | ~0.5% |
| Paracaecal | rare |
Microscopic Anatomy / Function
The mucosa resembles that of the colon but is notably infiltrated with lymphoid follicles (similar to Peyer's patches of the small intestine). Peak lymphoid tissue is present in the second decade of life and then regresses - this correlates with the peak incidence of appendicitis in teenagers and young adults.
The function of the appendix remains debated. It may act as a "safe house" for commensal bacteria and play a role in gut immune function through its lymphoid tissue.
2. ACUTE APPENDICITIS
Historical Note
Recognition of acute appendicitis as a clinical entity is attributed to Reginald Fitz, who presented a paper at the first meeting of the Association of American Physicians in 1886, entitled "Perforating inflammation of the vermiform appendix". Charles McBurney subsequently described the clinical manifestations, including the point of maximum tenderness in the right iliac fossa (McBurney's point).
Incidence
- Incidence rose greatly in the first half of the 20th century (up to 16% of the population underwent appendicectomy)
- The past 30 years have seen a dramatic fall in incidence in Western countries
- Lifetime risk of appendicectomy: 8.6% in males, 6.7% in females
- Rare in infants; peaks in teens and early twenties
- Equal sex incidence before puberty; male:female ratio rises to 3:2 at age 25, then declines
Aetiology
No single unifying hypothesis exists. Proposed factors include:
- Low dietary fibre / refined carbohydrate diet - parallels the geography of incidence; lowest incidence in high-fibre societies
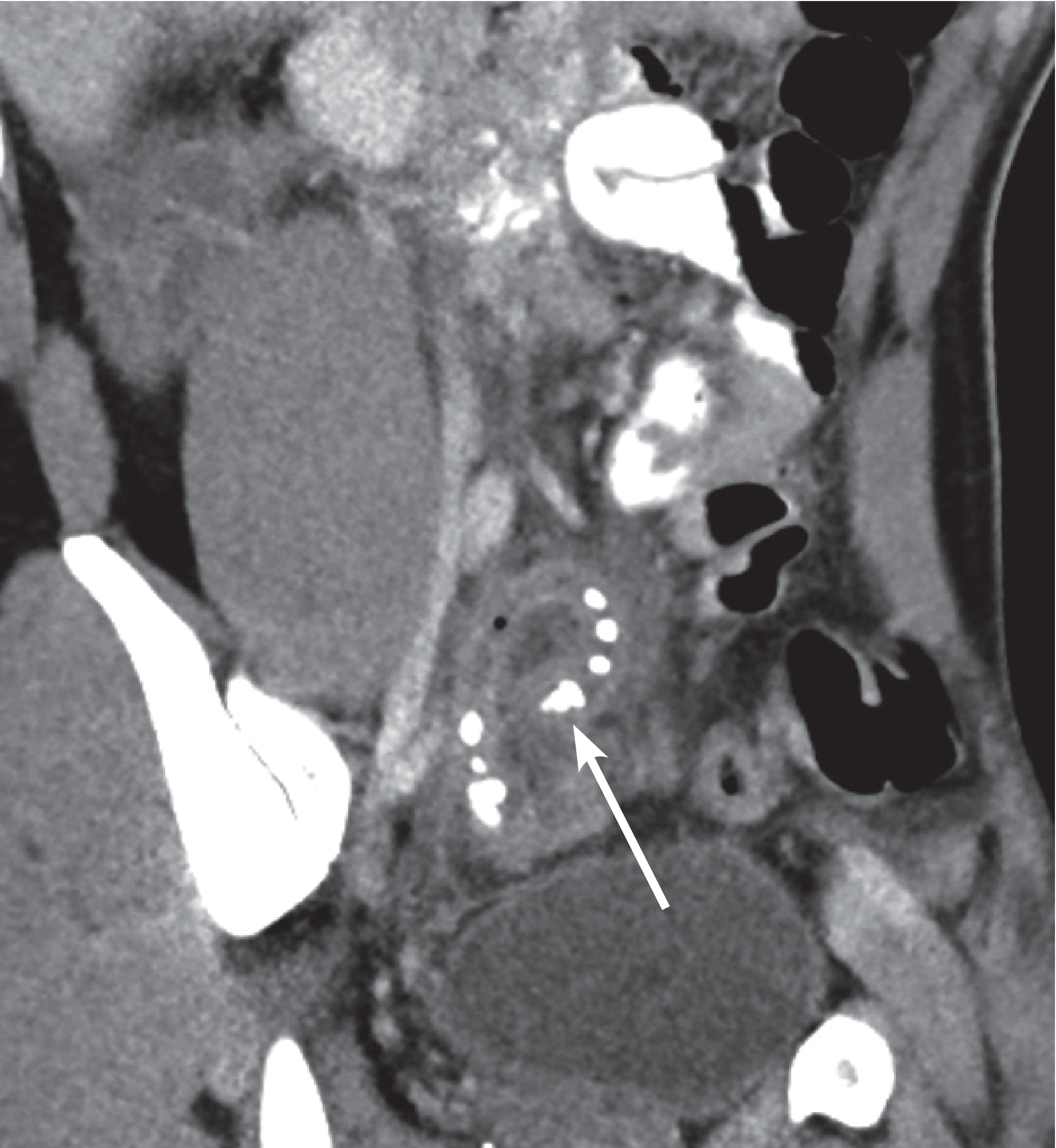
- Luminal obstruction - the most widely held initiating mechanism:
- Faecolith (appendicolith) - inspissated faecal material, calcium phosphates, bacteria, and epithelial debris. CT scan demonstration:
- Fibrotic stricture (previous resolved appendicitis)
- Caecal carcinoma obstructing the appendiceal orifice (in middle-aged/elderly)
- Intestinal parasites (e.g., Enterobius vermicularis/pinworm)
- Bacterial proliferation - mixed aerobic and anaerobic organisms; no single organism responsible
- Viral infection - occasional clustering in children/young adults and seasonal variation (May-August in northern Europe) suggests a viral initiating factor
Pathology
The sequence of events:
- Lymphoid hyperplasia narrows the appendix lumen
- Obstruction → continued mucus secretion → raised intraluminal pressure → obstructed lymphatic drainage
- Oedema and mucosal ulceration develop → bacterial translocation to submucosa
- Resolution may occur spontaneously or with antibiotics at this stage
- If it progresses → further distension → venous obstruction and ischaemia of the appendix wall
- Bacterial invasion through the muscularis propria and submucosa (gangrene)
- Perforation → faecal peritonitis or localised abscess formation
Symptoms
Classically:
- Central abdominal (periumbilical) pain initially - colicky or continuous, due to appendix distension (visceral pain, T10)
- Pain migrates to the right iliac fossa (RIF) - as parietal peritoneum becomes involved (somatic pain)
- Anorexia - almost universal; if the patient is hungry, appendicitis is unlikely
- Nausea and vomiting - occur after the onset of pain (important: if vomiting precedes pain, consider gastroenteritis)
- Fever - low grade (37.5-38°C); high fever suggests perforation or alternative diagnosis
- Constipation is common; diarrhoea may occur if inflamed appendix is in contact with bowel
Clinical Signs
Classic signs:
| Sign | Description |
|---|---|
| McBurney's point tenderness | Maximum tenderness at junction of lateral 1/3 and medial 2/3 of line from ASIS to umbilicus |
| Rovsing's sign | Palpation of LIF causes pain in RIF (due to shift of bowel gas) |
| Psoas sign | Pain on passive extension of hip (retrocaecal appendix irritating psoas) |
| Obturator sign | Pain on internal rotation of flexed right hip (pelvic appendix near obturator internus) |
| Guarding and rebound | Peritoneal irritation in RIF |
| Dunphy's sign | Increased pain on coughing |
Special features according to position:
- Retrocaecal appendix: Tenderness may be more lateral/posterior; psoas sign positive; flank/loin tenderness
- Pelvic appendix: Tenderness may be minimal anteriorly; rectal/vaginal examination reveals tenderness; diarrhoea and urinary symptoms more common
- Pre-ileal/post-ileal: May cause diarrhoea due to proximity to small bowel
Differential Diagnosis
The differential diagnosis differs by age and sex:
Children:
- Acute gastroenteritis (most common mimic - but vomiting/diarrhoea precede pain)
- Mesenteric lymphadenitis (colicky pain, cervical lymph nodes)
- Meckel's diverticulitis (clinically identical but may be central/left-sided)
- Intussusception (age <2 years, palpable mass)
- Henoch-Schönlein purpura (ecchymotic rash, normal platelets, microscopic haematuria)
- Right basal pneumonia (high fever, pleural signs, chest X-ray diagnostic)
Adults:
- Terminal ileitis (Crohn's / Yersinia - history of cramping, weight loss, diarrhoea)
- Perforated peptic ulcer
- Right ureteric colic
- Acute cholecystitis (high, more lateral)
- Psoas abscess
Women (additional):
- Ruptured ectopic pregnancy (ALWAYS exclude - do hCG)
- Mittelschmerz (mid-cycle, resolves quickly)
- Torsion/rupture of ovarian cyst
- Acute salpingitis/PID (bilateral, vaginal discharge, cervical excitation)
- Endometriosis
Scoring Systems
Alvarado Score (MANTRELS):
| Feature | Score |
|---|---|
| Migration of pain to RIF | 1 |
| Anorexia | 1 |
| Nausea/vomiting | 1 |
| RIF tenderness | 2 |
| Rebound tenderness | 1 |
| Elevated temperature (>37.3°C) | 1 |
| Leucocytosis (>10,000) | 2 |
| Shift to left (neutrophilia) | 1 |
| Total | 10 |
Score ≥7 = likely appendicitis; Score ≤4 = appendicitis unlikely.
Investigations
- WBC: Leucocytosis (10,000-18,000) with neutrophilia is typical. Normal WBC does not exclude appendicitis
- CRP: Elevated; more sensitive than WBC in later presentations
- Urine dipstick: 20-30% may show mild pyuria or haematuria (inflamed appendix near ureter/bladder) - does NOT exclude appendicitis
- Pregnancy test (hCG): Mandatory in all women of childbearing age
- Ultrasound: Operator-dependent; useful to exclude gynaecological pathology. Shows non-compressible tubular structure >6 mm in diameter
- CT scan (gold standard for adults): Sensitivity ~95%, specificity ~95%. Shows enlarged, enhancing appendix, periappendiceal fat stranding, faecolith. Preferred when diagnosis is uncertain
- MRI: Preferred in pregnancy (no radiation), useful in children
Risk Factors for Perforation
- Extremes of age (young children, elderly)
- Delay in presentation / diagnosis
- Faecolith present
- Immunocompromise
- Pelvic or retrocaecal position (delayed diagnosis)
3. MANAGEMENT
Preoperative
- IV fluids, NBM, analgesia (opiates do not mask signs and should not be withheld)
- IV antibiotics (reduce wound infection and intra-abdominal sepsis)
- Anti-emetics, DVT prophylaxis
Non-operative (Antibiotic) Treatment
- Increasingly supported by evidence for uncomplicated appendicitis
- Short-term resolution in ~70% of adults and ~90% of children
- Failure rate is high (~30% at 1 year requiring appendicectomy); patients must be fully counselled
- Patients >40 years treated conservatively must be followed up to exclude underlying malignancy
Appendicectomy (Surgical Treatment)
Open (Conventional) Appendicectomy
Incisions:
- Gridiron (McArthur) incision - at right angles to the spinoumbilical line, centred on McBurney's point
- Lanz (transverse/skin crease) incision - 2 cm below umbilicus, centred on midclavicular-midinguinal line; better cosmesis, easier extension
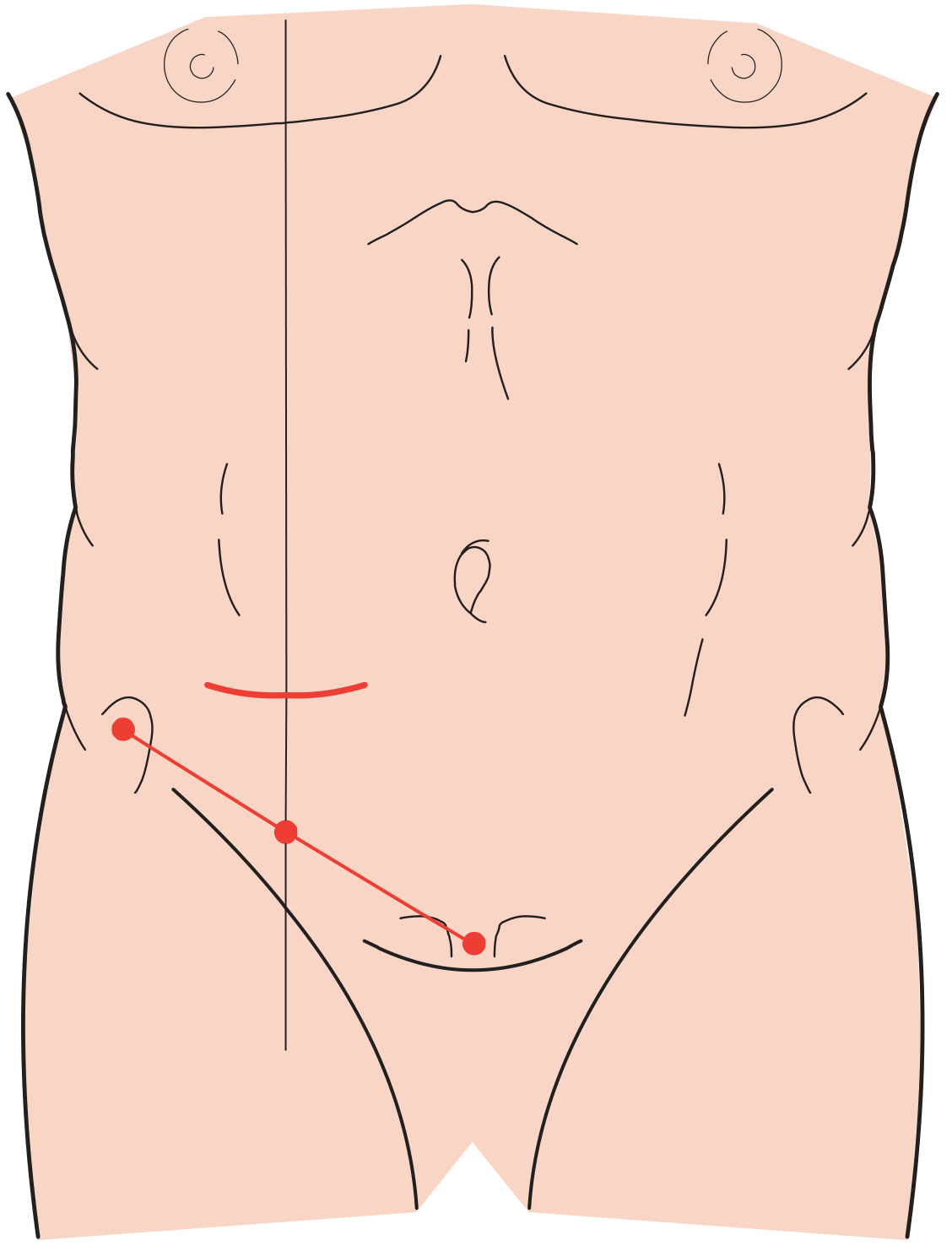
- Rutherford Morison incision - extends the gridiron by splitting internal oblique and transversus muscles in the line of the incision; used for retrocaecal appendix or when more access is needed
- Lower midline incision - when diagnosis is in doubt, particularly if peritonitis is present
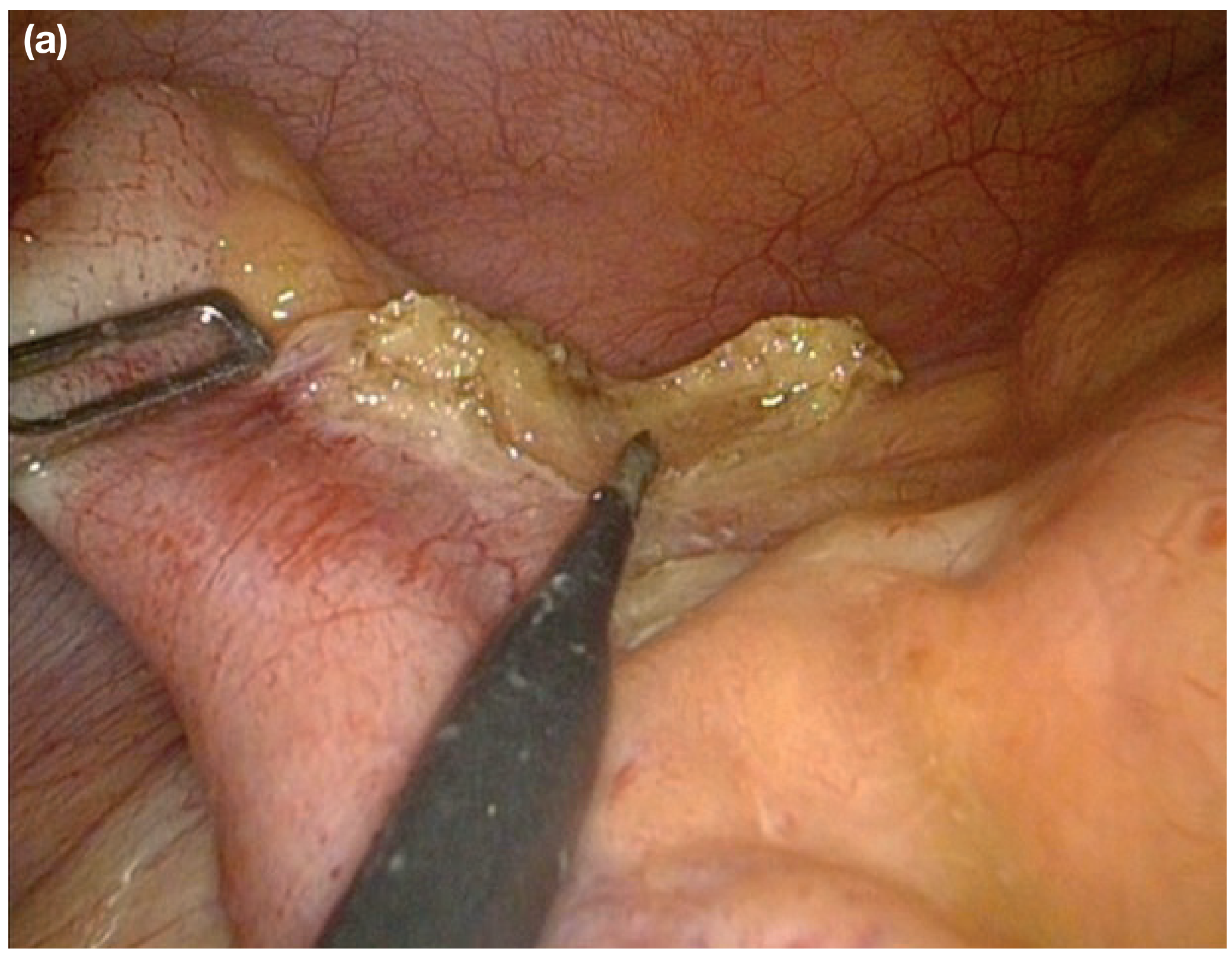
Laparoscopic Appendicectomy
Now the standard of care at most centres. Advantages include:
- Better diagnostic accuracy (especially in women)
- Reduced wound infection and hospital stay
- Faster return to work
- Superior visualisation of the peritoneal cavity
Steps include hook diathermy dissection of the mesoappendix, clipping/ligation of the appendicular artery, and ligation of the appendix base with absorbable ties or stapler.
4. COMPLICATIONS
Postoperative Complications Checklist (Bailey and Love's Summary Box 76.7)
- Examine wound and abdomen for wound abscess
- Perform rectal examination to exclude pelvic abscess
- Examine lungs for pneumonitis or collapse
- Examine legs for deep vein thrombosis
- Check conjunctivae/liver for jaundice and ask about rigors (pyelophlebitis - portal vein thrombosis)
- Examine urine for organisms (pyelonephritis)
- Suspect subphrenic abscess
Wound infection - most common complication; reduced with prophylactic antibiotics; more common after perforation.
Pyelophlebitis - septic thrombophlebitis of the portal vein. Presents with high swinging pyrexia, rigors, jaundice, and hepatomegaly. May lead to hepatic abscess. Treated with prolonged IV antibiotics.
5. APPENDIX MASS
- Forms when the inflamed appendix becomes walled off by omentum and adjacent bowel
- Standard treatment is the Ochsner-Sherren conservative regime
- Premise: inflammation is already localised; operating is difficult and may be dangerous
- IV antibiotics, IV fluids, 4-hourly temperature and pulse, mark mass extent on skin
- CT scan to identify abscess (drain radiologically if found)
- Clinical improvement expected in 24-48 hours (~90% resolve)
- Failure to resolve should raise suspicion of carcinoma or Crohn's disease
Criteria to STOP conservative treatment (Summary Box 76.6):
- Rising pulse rate
- Increasing or spreading abdominal pain
- Increasing size of the mass
- → Proceed to early laparotomy
Interval appendicectomy after resolution is debated; most patients will not develop recurrent appendicitis, but studies show interval appendicectomy may identify unsuspected neoplasms (especially in patients >40 years).
6. APPENDICITIS IN SPECIAL SITUATIONS
Appendicitis in Pregnancy
- Most common surgical emergency in pregnancy
- Diagnosis is difficult as the caecum and appendix migrate upward with the uterus
- Pain may be in the right upper quadrant in later pregnancy
- Perforation risk is higher due to delayed diagnosis
- Immediate surgery is indicated (no conservative approach)
- Laparoscopic approach is safe in any trimester (use open Hasson technique)
- Obstetric complications occur in ~5% of pregnant women undergoing abdominal surgery
7. RECURRENT ACUTE APPENDICITIS
- Rare; presents as chronic recurrent lower abdominal pain
- Arises from incomplete, self-limiting obstruction of the appendix lumen
- Attacks every few months; majority culminate in severe acute appendicitis
- Appendix shows thickening and fibrosis from previous inflammation
8. NEOPLASMS OF THE APPENDIX
Tumours occur in up to 0.97 per 100,000 of the population. Most are found incidentally at appendicectomy.
Classification
-
Neuroendocrine tumours (NETs) - ~30% of appendix neoplasms
- Slightly more common in females
- Incidence: 0.15-0.6 per 100,000/year
- Arise from subepithelial neuroendocrine cells
- 70% located at the appendix tip
- Average age at presentation: 40-50 years
- Mostly asymptomatic; carcinoid syndrome is extremely rare
- Diagnosed by immunohistochemistry for synaptophysin and chromogranin A; graded 1-3 by Ki-67 index and mitotic rate
- Treatment: Simple appendicectomy for tumours <2 cm (cured in >95%); right hemicolectomy for tumours >2 cm or with mesoappendiceal invasion
-
Epithelial tumours - most of the remainder
- Range from low-grade appendiceal mucinous neoplasm (LAMN) to high-grade invasive adenocarcinoma with signet ring features
- Perforation of a mucinous appendix tumour causes Pseudomyxoma Peritonei (PMP) - dissemination of epithelial cells and mucin production throughout the peritoneum
- Treatment ranges from appendicectomy (low-grade, confined) to cytoreductive surgery (CRS) + hyperthermic intraperitoneal chemotherapy (HIPEC) for PMP
-
Mesenchymal tumours - rare
- Lymphoma, neuroma, GIST, Kaposi's sarcoma, granular cell tumour
Management of Unexpected Appendix Tumour at Surgery
- If tumour is <2 cm and resection margins are clear, appendicectomy is sufficient
- If tumour is >2 cm, patient should be referred for right hemicolectomy after histological confirmation
- Bailey and Love's Short Practice of Surgery, 28th Edition, Chapter 76
Umbical hernia according to bealiy and lovely
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have all the content. Here is the comprehensive, detailed answer:
Umbilical Hernia - According to Bailey and Love's Short Practice of Surgery (28th Edition)
DEFINITION
A hernia is an abnormal protrusion of an organ or tissue through an opening in the layer that normally confines it.
The umbilical hernia is a primary ventral hernia - a protrusion through the umbilical cicatrix (scar/ring) of the anterior abdominal wall.
Classification of Ventral Hernias (European Hernia Society, 2009):
| Primary Ventral Hernias | Secondary Ventral Hernias |
|---|---|
| Umbilical | Incisional |
| Epigastric | Parastomal |
| Spigelian | |
| Lumbar | |
| Traumatic |
ANATOMY AND PATHOGENESIS
The umbilical defect is present at birth but normally closes as the stump of the umbilical cord heals, usually within a week of birth. This process may be delayed, leading to herniation in the neonatal period. The umbilical ring may also stretch and reopen in adult life.
In adults, conditions that cause stretching and thinning of the midline raphe (linea alba) predispose to reopening of the umbilical defect:
- Pregnancy
- Obesity
- Liver disease with cirrhosis and ascites
The defect in adults can occur:
- Directly through the umbilicus
- In the linea alba immediately adjacent to (most often above) the true umbilicus - these are commonly called paraumbilical hernias; however, under current guidelines, any hernia in the immediate vicinity of the umbilicus can now be called 'umbilical'
UMBILICAL HERNIA IN CHILDREN
Epidemiology
- Occurs in up to 10% of infants
- Higher incidence in premature babies
- Sexes equally affected
- Incidence in black infants is up to 8 times higher than in white infants
Clinical Features
- Appears within a few weeks of birth
- Often symptomless
- Increases in size on crying; assumes a classic conical shape
- Obstruction and/or strangulation is extremely uncommon below the age of 3 years
Treatment
Summary Box 64.14 (Bailey and Love):
- Common in infants; most resolve spontaneously
- Rarely strangulate
Conservative management is indicated under the age of 2 years when the hernia is symptomless. Parental reassurance is all that is necessary as 95% will resolve spontaneously.
If the hernia persists beyond the age of 2 years, surgical repair is indicated.
Surgery (in Children)
A small, curved incision is made immediately below the umbilicus. The neck of the sac is defined, opened, and any contents returned to the peritoneal cavity. The sac is closed and redundant sac excised. The defect in the linea alba is closed with interrupted sutures of slowly absorbable material.
UMBILICAL HERNIA IN ADULTS
Clinical Features
- Commonly seen in overweight men with a thinned and attenuated midline raphe
- Also in postpartum women with a weakened abdominal wall
- Women are affected more than men
- The bulge is typically slightly to one side of the umbilical depression, creating a crescent-shaped appearance to the umbilicus

Contents
- Small hernias often contain extraperitoneal fat or omentum
- Larger hernias can contain small or large bowel
Why Adult Umbilical Hernias are Dangerous
Because the hernia neck is relatively narrow in relation to the size of the sac, they are prone to become:
- Irreducible (incarcerated)
- Obstructed
- Strangulated
Symptoms
Most patients complain of:
- Pain due to tissue tension
- Symptoms of intermittent bowel obstruction
- In large hernias, the overlying skin may become very thin; overlying skin irritation and ulceration may occur
- Spontaneous rupture is extremely rare
TREATMENT IN ADULTS
As a result of the high risk of strangulation, surgery should be advised in cases where the hernia contains bowel. Small hernias may be left alone if asymptomatic, but may enlarge and require surgery later.
Surgery may be performed open or laparoscopically.
OPEN UMBILICAL HERNIA REPAIR
For defects <1 cm:
- Simple suture repair, provided the fascia is not closed under tension
- Alternative: darn suture technique - a non-absorbable monofilament suture is criss-crossed across the defect and anchored firmly to the fascia all around
For defects up to 2 cm - Mayo Repair:
- A transverse incision is made over the hernia
- Hernia sac dissected, opened, contents reduced
- Peritoneum closed
- The defect in the linea alba is extended transversely
- Fascial edges closed in an overlapping style with the superior flap on top - the "waistcoat over trousers" technique
- Non-absorbable sutures used
- Redundant skin may need to be excised for cosmesis
Current evidence:
- The Mayo repair remains popular for defects up to 2 cm, but the larger the defect the more tissue tension
- Current evidence advises the use of mesh even in small defects, and certainly for all defects larger than 2 cm, due to high likelihood of recurrence
LAPAROSCOPIC UMBILICAL HERNIA REPAIR
Technique:
- A camera port and two working ports are placed laterally on the abdominal wall, well away from the defect
- Contents of the hernia are reduced by traction and external pressure
- The falciform ligament above and the median umbilical fold below may need to be taken down to create a smooth, firm surface for mesh placement
- A disc of non-adherent mesh designed for intraperitoneal use is introduced and positioned on the undersurface of the abdominal wall, centred on the defect
- Fixed to the peritoneum and posterior rectus sheaths using staples, tacks, or sutures
Advantages:
- Fewer wound complications than open repair
- Allows large pieces of mesh
- Should be considered for obese patients, those with concomitant rectus divarication, and those with multiple ventral hernia defects
Disadvantages:
- Requires specialised equipment and expensive tissue-separating mesh
- Risk of bowel adhesion, erosion, and fistulation
- Intraperitoneal meshes can cause severe pain lasting 24-48 hours post-op that can mimic peritonitis
- Tacks/sutures used to fix the mesh can be a source of chronic pain
SPECIAL CIRCUMSTANCES
Pregnancy:
- Women often develop umbilical hernias during pregnancy; may present in the early postpartum period
- There is often a degree of rectus divarication
- Advised to exercise, lose weight, and increase abdominal muscle tone before surgery is considered
- These may resolve completely within a few months
- Strongly recommended to avoid surgery for umbilical hernia repair before or during pregnancy
Liver Cirrhosis:
- Patients with liver cirrhosis have extremely high mortality and morbidity after primary ventral hernia repair, especially with Child's B and C disease
- Patient selection is very important, with appropriate hepatology support if surgery is contemplated
- Fascial repair is best done with fine continuous sutures to minimise the risk of postoperative ascites leakage
EMERGENCY REPAIR OF UMBILICAL HERNIA
Incarceration, bowel obstruction, and strangulation are frequent because of the narrow neck and the fibrous edge of the defect in the midline raphe. Delay to surgery can lead to gangrene of the omentum or bowel.
Key points:
- Large hernias are often multiloculated - there may be strangulated bowel in one component while other areas appear clinically soft and non-tender
- Most emergency repairs are performed by open surgery
- In the presence of established strangulation, mesh should be avoided (risk of infection is too high)
- The focus of the emergency operation is to deal with the strangulated tissue
- A suture repair is advised, with a more definitive repair to be performed at a later date if necessary
SUMMARY TABLE
| Feature | Children | Adults |
|---|---|---|
| Incidence | Up to 10% of infants | Common; women > men |
| Predisposing factors | Prematurity, black race | Obesity, pregnancy, cirrhosis/ascites |
| Risk of strangulation | Extremely rare (<3 years) | High (narrow neck, fibrous edge) |
| Spontaneous resolution | 95% by age 2 | Does not resolve |
| Treatment <2 yrs | Conservative (reassurance) | - |
| Treatment >2 yrs | Surgery (suture repair) | Surgery (mesh preferred) |
| Surgical repair | Curved infra-umbilical incision, suture | Mayo / mesh open or laparoscopic |
- Bailey and Love's Short Practice of Surgery, 28th Edition, Chapter 64
This is a shared conversation. Sign in to Orris to start your own chat.