Pulmonary tuberculosis
Reading File
Finding Sources
Finding Sources
Searching PubMed
"pulmonary tuberculosis"[MeSH Terms] AND "treatment"[MeSH Terms]
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Only pathology answer 5 marks
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
I now have comprehensive pathology content from Robbins (the gold standard for pathology). Here is the complete 5-mark answer:
Pathology of Pulmonary Tuberculosis
1. Causative Organism and Route of Entry
Pulmonary TB is caused by Mycobacterium tuberculosis, an obligate aerobe transmitted by inhalation of infectious droplet nuclei. The bacilli are ingested by alveolar macrophages, where they block phagosome-lysosome fusion and resist acidification, allowing intracellular multiplication.
2. Primary Tuberculosis
The initial infection (primary TB) almost always begins in the lungs in adults. Key morphological events:
- Inhaled bacilli implant in the distal airspaces of the lower upper lobe or upper lower lobe, close to the pleura
- A 1-1.5 cm gray-white area of consolidation develops - the Ghon focus - with central caseous necrosis
- Bacilli drain to regional hilar/mediastinal lymph nodes, which also caseate
- The parenchymal lesion + lymphangitis + caseous lymphadenopathy = Ghon complex (Ranke complex)
- In ~95% of immunocompetent individuals, cell-mediated immunity controls infection; the Ghon complex undergoes progressive fibrosis and calcification
- Despite hematogenous seeding of other organs during this phase (liver, spleen, kidneys, lung apices), no lesions develop if immunity is adequate
3. The Tuberculous Granuloma (Hallmark Lesion)
The characteristic microscopic lesion is the caseating granuloma (tubercle):
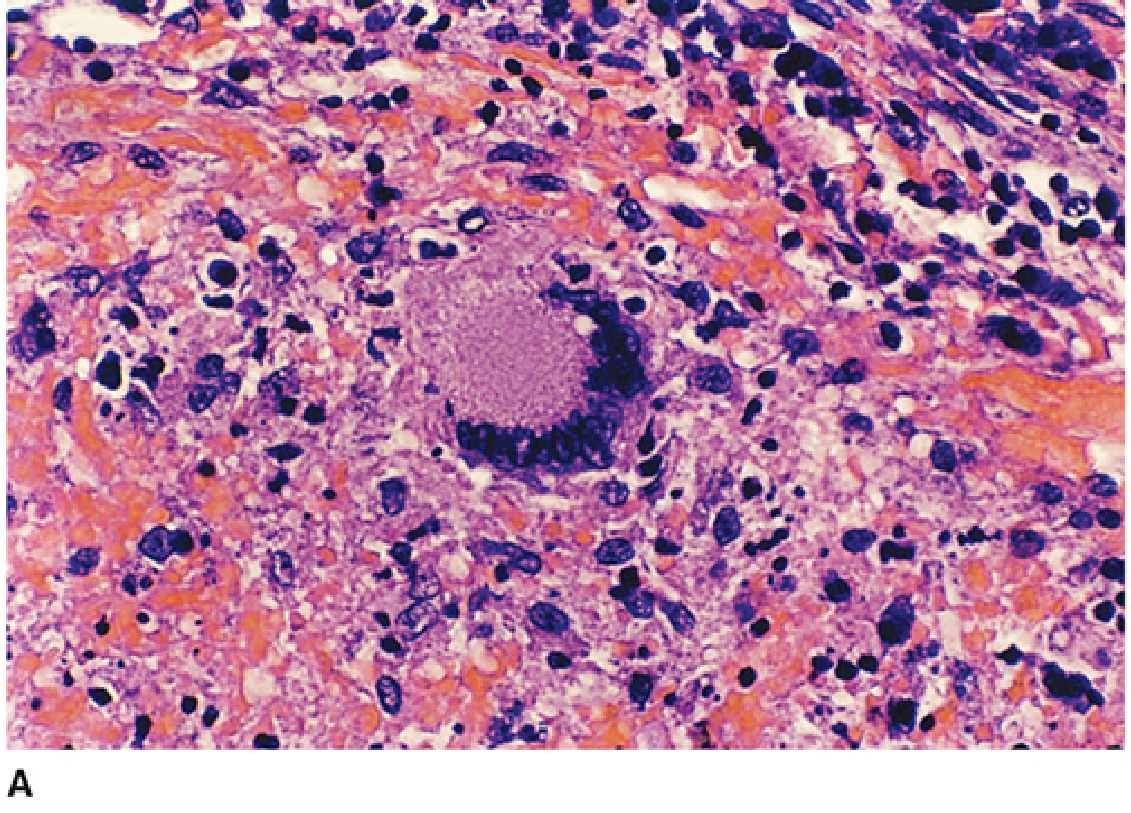
Composition of a tubercle (from center outward):
| Layer | Cell Type |
|---|---|
| Center | Caseous necrosis - cheesy, amorphous, acellular |
| Inner zone | Epithelioid cells (activated macrophages with abundant pink cytoplasm) |
| Middle | Langhans-type giant cells (fused macrophages, nuclei arranged in horseshoe/peripheral pattern) |
| Outer rim | Lymphocytes (CD4+ Th1, CD8+ CTLs) and fibroblasts |
- Individual granulomas are microscopic; they become macroscopically visible only when multiple coalesce
- Caseous necrosis is the hallmark - named for the cheese-like, semisolid appearance grossly; it results from the destructive delayed-type hypersensitivity (DTH) response driven by IFN-γ
- In immunocompromised individuals, granulomas fail to form; macrophages instead contain sheets of bacilli without organized reaction
4. Secondary (Postprimary/Reactivation) Tuberculosis
Reactivation occurs in 10% of latently infected persons, preferentially at aerobic high-oxygen-tension sites (lung apices, renal cortex):
- Apical lesion: small (<2 cm), sharply circumscribed, firm, gray-white to yellow focus within 1-2 cm of apical pleura
- Histology: coalescent caseating tubercles; acid-fast bacilli identifiable by Ziehl-Neelsen stain in early phases
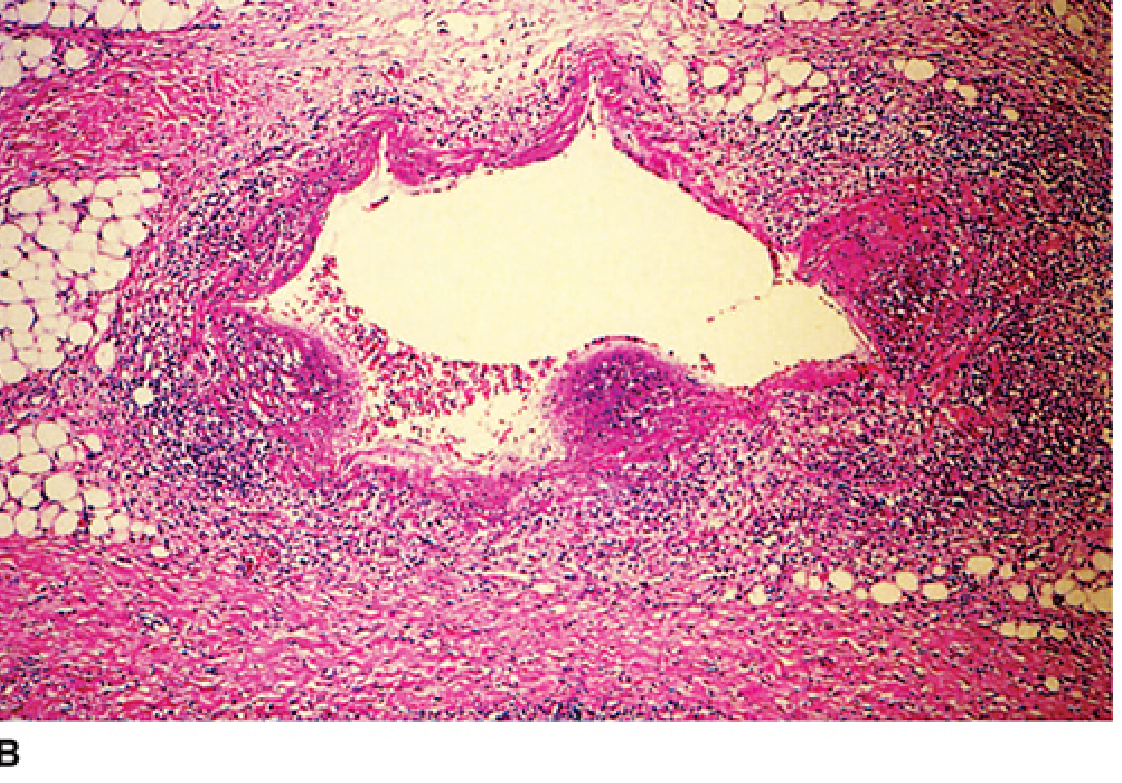
- Outcomes of progressive disease:
| Pathway | Morphology |
|---|---|
| Cavity formation | Caseous center liquefies and drains into bronchus → ragged, irregular cavity with poorly walled fibrous tissue; erosion of vessels → hemoptysis |
| Bronchogenic spread | Spread to other lobar segments via airway secretions |
| Miliary TB | Lymphohematogenous spread → 1-2 mm yellow-white foci throughout lung parenchyma resembling millet seeds |
| Pleural involvement | Serous effusion, empyema, or obliterative fibrous pleuritis |
| Healing | Fibrosis, calcification, architectural distortion; sterile cavities may persist |
5. Summary of Key Pathological Distinctions
| Feature | Primary TB | Secondary TB |
|---|---|---|
| Site | Lower upper / upper lower lobe, subpleural | Apex of upper lobe |
| Ghon focus | Present | Absent |
| Lymphadenopathy | Prominent | Minimal |
| Cavitation | Rare | Common |
| Spread | Hematogenous | Bronchogenic |
| Granulomas | Yes (if immunocompetent) | Yes, coalescent |
Sources: Robbins & Cotran Pathologic Basis of Disease (10th Ed.), Sherris & Ryan's Medical Microbiology (8th Ed.)
This is a shared conversation. Sign in to Orris to start your own chat.