Endometriosis in post pattum women
Reading File
Finding Sources
Searching PubMed
endometriosis postpartum
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Searching PubMed
endometriosis postpartum recurrence lactation breastfeeding
Finding Sources
Finding Sources
Reading Article
PMID: 39049473
Reading File
Reading Article
PMID: 34682348
Searching the Web
endometriosis postpartum recurrence scar endometriosis after cesarean section 2024 2025
Loading Image
Loading Image
I now have all the material needed for a comprehensive, well-sourced answer.
Endometriosis in the Postpartum Period
Background: What Endometriosis Is
Endometriosis is the presence of endometrial glands and stroma in extrauterine sites. It affects 5-10% of women of reproductive age, and nearly 50% of women with infertility. The three main phenotypes are:
- Superficial peritoneal endometriosis - red/brown/black "powder-burn" lesions
- Ovarian endometriosis (endometriomas) - chocolate cysts filled with old blood
- Deep infiltrating endometriosis (DIE) - tissue >5 mm beneath peritoneum, invading uterosacral ligaments, vagina, bowel, bladder, or ureters
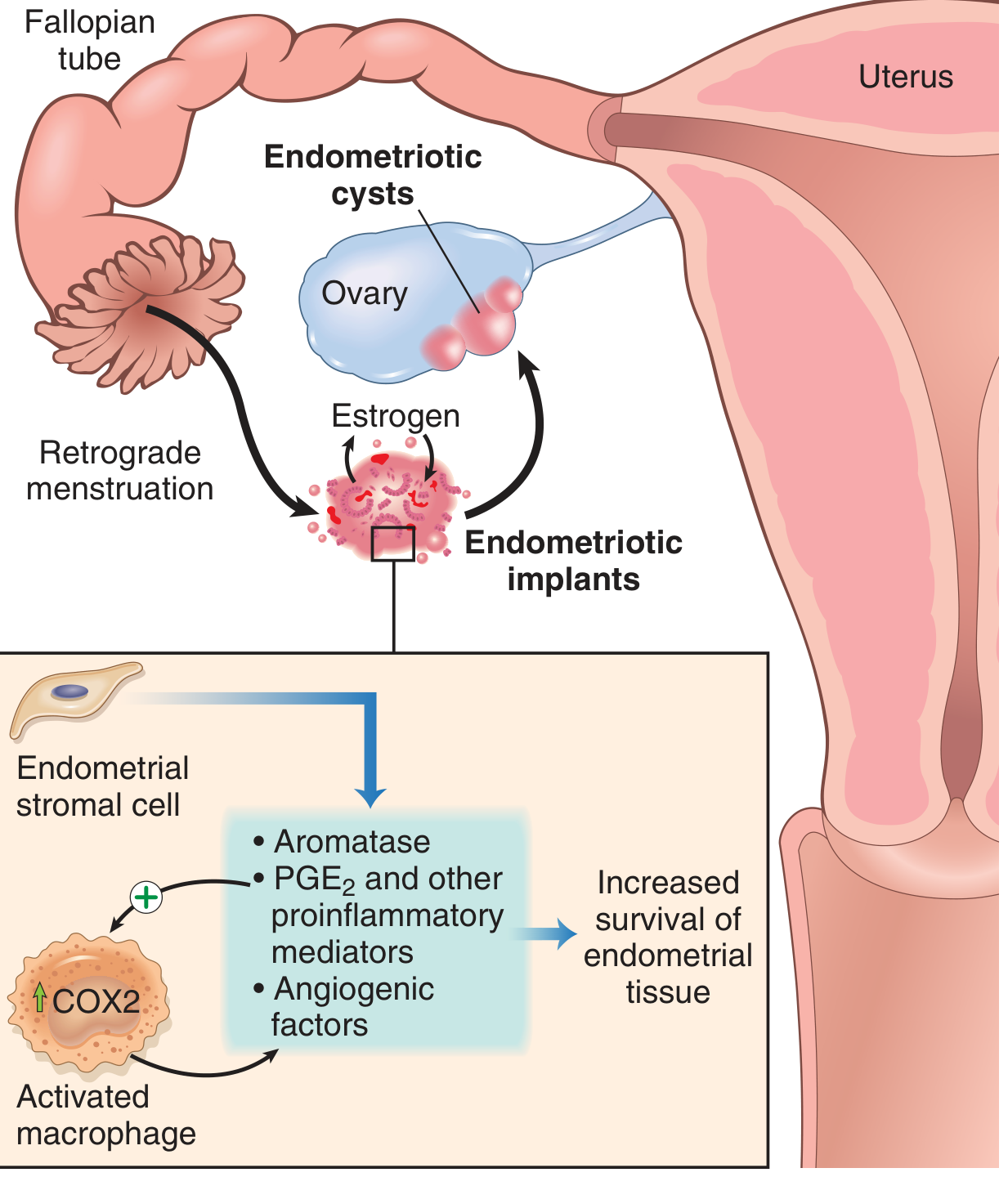
Pathogenesis: retrograde menstruation deposits endometrial tissue; implants survive by upregulating aromatase, PGE2, and VEGF via an activated macrophage loop (Robbins & Kumar Basic Pathology)
How Pregnancy Affects Endometriosis
During Pregnancy
- Lesions tend to enlarge during the first trimester but regress thereafter
- Studies in baboons found no change in lesion number or surface area during the first two trimesters; a beneficial effect may emerge in the third trimester or immediate postpartum period
- The classic "pseudopregnant state" theory - that high progesterone causes decidualization of implants and improvement - is not well substantiated
- The more likely explanation for pregnancy-associated symptom relief is simply amenorrhea, which removes the monthly cycle of retrograde menstrual seeding and hormonal stimulation
The Postpartum Period Specifically
Why symptoms return postpartum: Once menstruation resumes, estrogen levels rise again and the underlying driver of endometriosis is restored. The timing of return mirrors the resumption of ovulatory cycles.
Role of breastfeeding: A 2021 prospective observational study (PMID 34682348, n=123 postpartum women with endometriosis) found:
- All breastfeeding patients experienced significant reduction in dysmenorrhea, proportional to breastfeeding duration
- Chronic pelvic pain (CPP) was significantly reduced only in women who exclusively breastfed
- Ovarian endometriomas were significantly reduced in size
- Dyspareunia showed no significant improvement regardless of breastfeeding type
- The mechanism is lactational amenorrhea - suppression of the hypothalamic-pituitary-ovarian axis by prolactin, resulting in hypoestrogenism
Bottom line: Extended exclusive breastfeeding delays recurrence of endometriosis-related pain by prolonging the amenorrheic hypoestrogenic state.
Obstetric Complications in Women with Endometriosis
A major 2024 systematic review and meta-analysis (Busnelli et al., Human Reproduction Update, PMID 39049473, 34-43 studies) found:
| Complication | Odds Ratio | Notes |
|---|---|---|
| Placenta previa | OR 2.84 (95% CI 2.47-3.26) | Strongest risk; OR rises to 14.54 in deep endometriosis |
| Preterm birth | OR 1.43 (95% CI 1.32-1.56) | Particularly high in severe (stage III-IV) disease |
| Cesarean section | OR 1.52 (95% CI 1.41-1.63) | Increased across all subtypes |
These associations held regardless of whether conception was spontaneous or via ART.
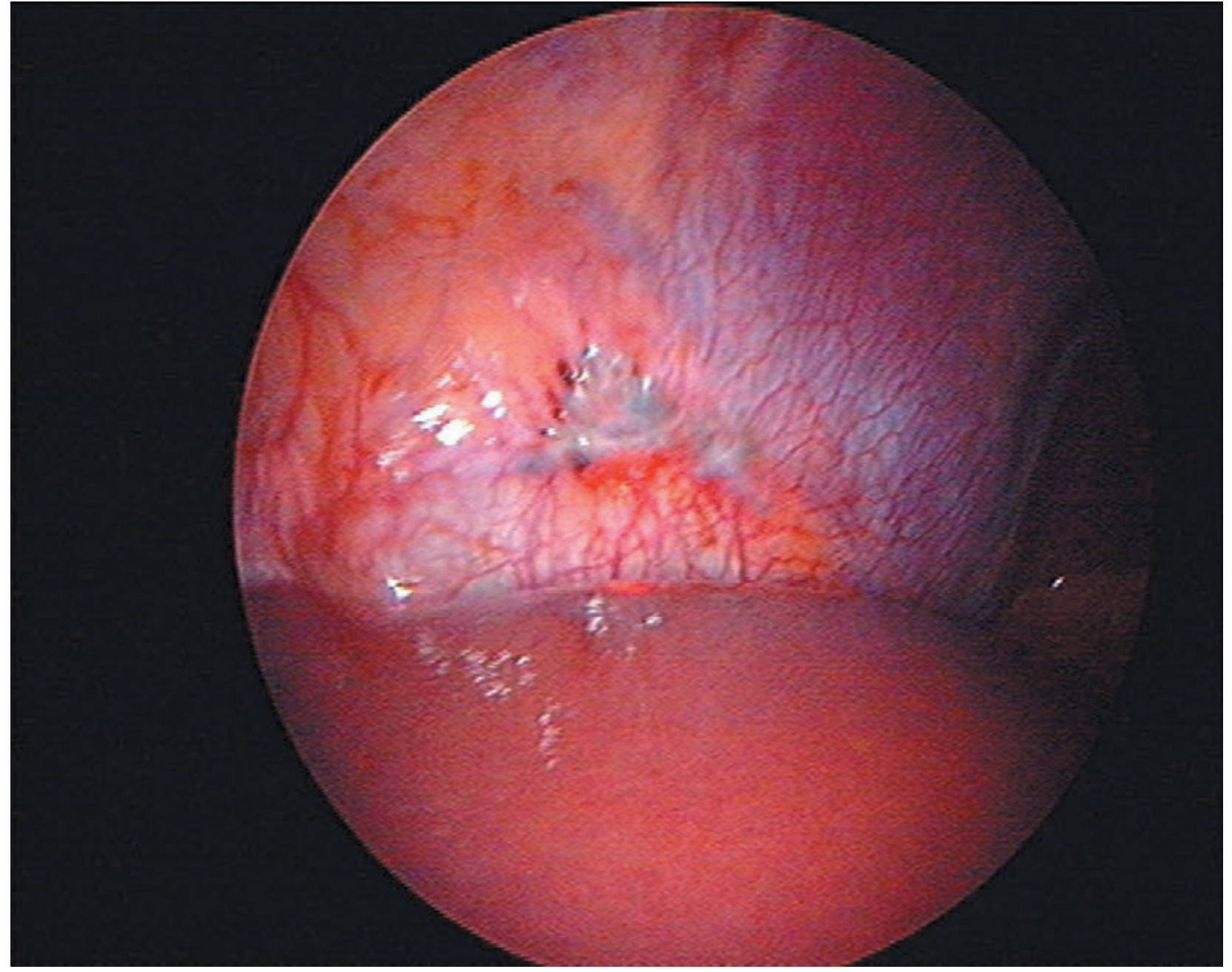
Endometriosis seen on the peritoneal surface of the diaphragm (Bailey & Love's Short Practice of Surgery, 28th ed.)
A Key Postpartum-Specific Entity: Cesarean Scar Endometriosis (CSE)
This is a form of iatrogenic / abdominal wall endometriosis unique to the postpartum period following cesarean delivery.
Mechanism
During cesarean section, endometrial cells are inadvertently transplanted into the abdominal wall at the incision site. These cells implant, establish a blood supply, and respond to subsequent hormonal cycles exactly like eutopic endometrium.
Epidemiology
- Incidence: 0.03-0.4% of all endometriosis cases arise in cesarean scars
- ~80% of cases occur at the corners of the Pfannenstiel incision (the scar corners concentrate implanted cells)
- Typically presents months to years postpartum (average ~3 years post-CS in reported cases)
Clinical Features
- Cyclically painful mass at or near the cesarean scar - pain waxes/wanes with menstrual cycle
- Palpable nodule, sometimes discolored or with surface bleeding
- May mimic poorly healed scar, stitch granuloma, hernia, or lipoma
- Deep infiltrating forms can involve underlying rectus muscle or fascia
Diagnosis
- Clinical history (prior CS, cyclical pain at scar site) is the most important clue
- Ultrasound - first-line imaging; shows a hypoechoic mass with internal flow on Doppler
- MRI - better delineates depth of invasion, relationship to fascial layers
- CT and MRI are not diagnostic for the endometriotic nature - biopsy confirms
- Biopsy / surgical excision with histology showing endometrial glands + stroma is diagnostic
Treatment
| Approach | Role |
|---|---|
| Surgical excision with 1 cm clear margins | Definitive treatment; recurrence rate ~4.3% post-excision |
| Hormonal suppression (OCPs, progestogens, GnRH agonists) | Temporary symptom control only; disease recurs on stopping |
| NSAIDs | Pain palliation for mild cases |
| Hormonal therapy pre-/post-op | Can shrink lesions pre-operatively or reduce recurrence risk post-operatively |
Surgery is the only curative option. Hormonal therapy alone does not eliminate scar endometriosis.
Postpartum Management Considerations for Pre-existing Endometriosis
When Symptoms Recur After Delivery
Once menstruation resumes (earlier in non-breastfeeding women, typically 6-8 weeks postpartum; later in exclusive breastfeeders), endometriosis-associated symptoms may return. Management options include:
Medical:
- Progestogens (norethisterone, dienogest, LNG-IUS) - first-line for pain, safe in breastfeeding women per most guidelines (low systemic absorption with LNG-IUS)
- Combined oral contraceptives - effective for pain suppression; contraindicated during active breastfeeding (estrogen reduces milk supply); can be used once breastfeeding is established
- GnRH agonists (leuprolide, nafarelin) + add-back HRT - for severe disease; generally deferred postpartum until after cessation of breastfeeding
- NSAIDs (ibuprofen, naproxen) - adjunct analgesia, caution re: breastfeeding timing
Surgical:
- Laparoscopic excision or ablation of lesions
- For women who have completed their family: hysterectomy + bilateral salpingo-oophorectomy with complete excision of endometriotic deposits offers best chance of cure
- For fertility-sparing surgery: aim to remove disease while preserving ovarian tissue (ovarian drainage + directed spot ablation preferred over cystectomy to minimize damage to ovarian reserve)
Fertility Considerations
Women with pre-existing endometriosis who have just delivered have improved prospects for subsequent pregnancy in the short window following delivery, before disease re-establishes. The decision for further pregnancy should factor in:
- Stage of disease (rASRM / ENZIAN classification)
- Endometriosis Fertility Index (EFI) score
- Ovarian reserve (AMH, AFC)
- Whether residual endometriomas persist
Summary Table
| Aspect | Key Points |
|---|---|
| Disease behavior during pregnancy | Lesions may enlarge in T1, regress in T2/T3; mechanism = amenorrhea |
| Postpartum symptom recurrence | Follows return of menstruation; earlier in non-breastfeeders |
| Breastfeeding benefit | Exclusive BF reduces dysmenorrhea and CPP; shrinks endometriomas |
| Obstetric risks | Placenta previa (OR 2.84), preterm birth (OR 1.43), cesarean (OR 1.52) |
| Scar endometriosis | Iatrogenic after CS; cyclical scar pain + mass; surgery curative |
| Medical treatment postpartum | Progestogens safest during BF; COCs after BF cessation; GnRH agonists reserved for severe disease |
| Surgical treatment | Laparoscopic excision; BSO + hysterectomy if family complete |
Sources:
- Berek & Novak's Gynecology (Spontaneous Evolution / Pregnancy sections, pp. 651-652)
- Bailey & Love's Short Practice of Surgery 28th ed., Ch. 87 (Endometriosis, pp. 1603-1604)
- Robbins & Kumar Basic Pathology (Pathogenesis, p. 689)
- Fischer's Mastery of Surgery 8th ed. (Abdominal wall endometriosis, p. 6206)
- Busnelli et al. 2024, Hum Reprod Update (PMID 39049473) - Systematic review/meta-analysis on endometriosis and adverse pregnancy outcomes
- Prosperi Porta et al. 2021, Int J Environ Res Public Health (PMID 34682348) - Breastfeeding effects on endometriosis pain
This is a shared conversation. Sign in to Orris to start your own chat.