Presentation of partial seizures
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content. Let me compile the full answer.
Presentation of Partial (Focal) Seizures
Terminology and Classification
The term "partial seizure" has been largely replaced by "focal seizure" in the ILAE 2017 classification, though both terms remain in use. The key update maps as follows:
| Old (1981) Term | New (2017) Term |
|---|---|
| Partial seizure | Focal seizure |
| Simple partial seizure | Focal aware seizure (FAS) |
| Complex partial seizure | Focal impaired awareness seizure (FIAS) |
| Secondarily generalized seizure | Focal to bilateral tonic-clonic seizure |
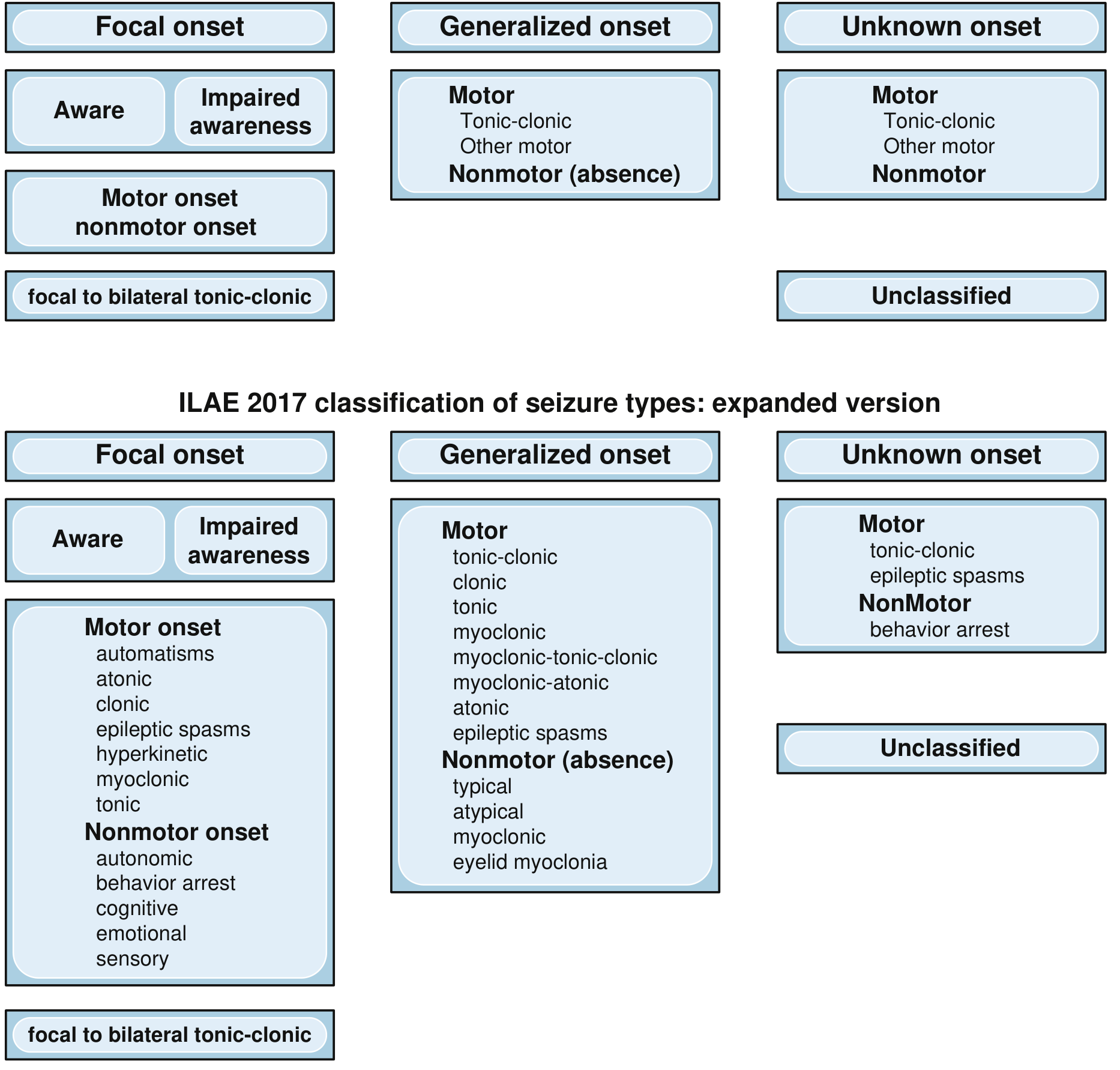
The 2017 ILAE classification of seizure types:
Pathophysiology
Focal seizures begin in a localized area of one cerebral hemisphere and reflect the function of that region. Common causes include:
- Scar tissue pulling on adjacent neurons
- Tumors compressing cortical areas
- Destroyed brain tissue
- Congenitally disordered local circuitry
When neuronal discharge rate rises above a threshold, synchronous waves spread to adjacent cortical regions at rates ranging from a few mm/minute to several cm/second. Spread can also occur remotely via thalamic projections to the contralateral cortex.
- Guyton and Hall Textbook of Medical Physiology
1. Focal Aware Seizures (Simple Partial Seizures)
Consciousness is fully preserved throughout the seizure. The clinical manifestations depend on the brain region involved.
Motor symptoms
- Jacksonian march: rhythmic clonic jerking that spreads progressively along the motor homunculus (classically starting at the mouth or hand, then marching down the limb). Activity is contralateral to the epileptic hemisphere.
- Focal tonic stiffening of a limb
- Versive head/eye turning (contralateral)
Somatosensory / Special sensory symptoms
- Tingling, numbness, or electric sensations (contralateral body)
- Visual: flashing lights, formed hallucinations (occipital lobe)
- Auditory: buzzing, tones, or complex sounds (lateral temporal/Heschl gyrus)
- Olfactory/gustatory auras (usually mesial temporal; also with tumoral etiology)
- Vertiginous auras (posterior temporal or parietal)
Autonomic symptoms
- Epigastric rising sensation (most common aura in temporal lobe epilepsy)
- Pallor, flushing, piloerection ("gooseflesh"), tachycardia, palpitations
Psychic (cognitive/emotional) symptoms
- Fear or anxiety (amygdala involvement)
- Deja vu or jamais vu (hippocampal/temporal)
- Depersonalization, dream-like states
- Forced thinking, speech arrest (dominant hemisphere)
Auras
FAS of purely subjective character are called auras or isolated auras. They are typically brief (seconds to minutes). A prolonged aura is termed aura continua, which is focal nonconvulsive status epilepticus without impaired consciousness.
- Bradley and Daroff's Neurology in Clinical Practice
2. Focal Impaired Awareness Seizures (Complex Partial Seizures)
Characterized by altered awareness at some point during the seizure. Impairment can range from subtle (mild confusion, slowing of responses) to complete amnesia for the event.
Typical features:
- May begin with an aura (as above), followed by loss of awareness
- Behavior arrest: sudden cessation of ongoing activity, staring
- Automatisms: semi-purposeful, stereotyped movements, the patient has no recollection of
- Oroalimentary: lip smacking, chewing, swallowing (most common)
- Manual: fumbling, picking, rubbing hands
- Ambulatory: walking, trying to stand up
- Duration: typically 1-2 minutes (range 30 seconds to 3 minutes)
- Postictal phase: gradual return to consciousness with confusion, fatigue, and possible amnesia (contrast with absence seizures, which terminate abruptly)
Key comparison - Complex Partial vs. Absence Seizures:
| Feature | Absence Seizure | Complex Partial Seizure |
|---|---|---|
| Age at onset | Childhood/adolescence | Any age |
| Aura or warning | None | Common |
| Onset | Abrupt | Gradual |
| Duration | Seconds | 1-2 minutes |
| Automatisms | Simple | Complex |
| Postictal phase | None | Confusion, fatigue |
| Provocation by hyperventilation | Common | Uncommon |
| EEG | 3 Hz generalized spike-and-wave | Focal discharges or focal slowing |
| Neuroimaging | Usually normal | May show focal lesion |
- Bradley and Daroff's Neurology in Clinical Practice
3. Focal to Bilateral Tonic-Clonic Seizures (Secondary Generalization)
Formerly called "secondarily generalized seizures." Either a FAS or FIAS may evolve into bilateral tonic-clonic activity.
Sequence of evolution:
- Versive head turning contralateral to the hemisphere of onset
- Figure-of-four posturing: contralateral arm extended, ipsilateral arm flexed - lateralizes to the hemisphere contralateral to the extended arm
- Bilateral tonic phase (may be asymmetrical)
- Clonic phase: decreasing frequency of jerks over time, may end asymmetrically
- Postictal period: limpness, stertorous (snoring) respiration, gradual recovery
- Bradley and Daroff's Neurology in Clinical Practice
4. Localization-Based Presentations
Temporal Lobe (most common)
Mesial temporal (amygdalohippocampal):
- Epigastric rising aura (most common)
- Fear, anxiety, deja/jamais vu
- FIAS with oroalimentary automatisms and contralateral arm dystonic posturing
- Ipsilateral extremity automatisms (contralateral arm is "frozen" in dystonia)
- Postictal aphasia after dominant temporal lobe seizures
Lateral (neocortical) temporal:
- Auditory auras, vertigo, complex visual hallucinations
- Shorter duration, greater tendency to secondarily generalize
Frontal Lobe
- Motor cortex: focal clonic activity +/- Jacksonian march
- Supplementary motor area (SMA): asymmetrical tonic/postural seizures (fencing posture), usually with preserved consciousness despite bilateral motor involvement - this is an important exception to the rule; these are short, often arise from sleep, occur in clusters
- Anterior cingulate/hypermotor: thrashing, kicking, cycling leg movements, may appear bizarre
- Frontal lobe seizures: brief, often nocturnal, may have minimal postictal state
Parietal Lobe
- Contralateral somatosensory symptoms (tingling, numbness, pain)
- May spread to produce motor features
Occipital Lobe
- Contralateral visual phenomena (phosphenes, scotomas, formed hallucinations)
5. EEG Findings
- Interictal: focal spikes, sharp waves, or focal slowing over the epileptogenic zone
- Ictal: focal high-frequency rhythmic discharge evolving in frequency/amplitude over time
- Complex partial seizures: focal epileptic discharges or focal slowing (contrast with 3 Hz spike-and-wave of absence seizures)
- Psychomotor (complex partial) seizures: low-frequency rectangular wave 2-4/sec with superimposed 14/sec waves
Summary
Partial/focal seizures arise from a localized cortical area and their semiology directly reflects the function of that region. The key clinical distinction is whether awareness is preserved (FAS) or impaired (FIAS). Secondary generalization can occur in either type and carries additional lateralizing signs. Temporal lobe seizures are the most common type in adults and typically present with an epigastric aura, altered awareness, and oroalimentary automatisms.
Bulbar and pseudobapbar palsy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Excellent - I now have rich content from multiple authoritative sources. Let me compile the comprehensive answer.
Bulbar Palsy and Pseudobulbar Palsy
These two syndromes both cause dysarthria, dysphagia, and dysphonia involving the lower cranial nerves (V, VII, IX, X, XI, XII), but differ fundamentally in the level of the lesion - LMN vs. UMN - producing opposite signs on examination.
Anatomy: What is the "Bulb"?
The term bulb refers to the medulla oblongata (an old anatomical term for the brainstem's lower portion). The motor nuclei of cranial nerves IX, X, XI, and XII reside within it, controlling:
- Tongue (XII - hypoglossal)
- Pharynx and larynx (IX, X - glossopharyngeal, vagus)
- Palate (X)
- Sternocleidomastoid and trapezius (XI - accessory)
- Jaw and face (V, VII - technically outside the medulla but included clinically)
These nuclei receive bilateral corticobulbar input from both motor cortices, with one exception: the lower face (facial nerve) receives predominantly contralateral supranuclear innervation.
1. Bulbar Palsy (LMN)
Definition
A lower motor neuron syndrome resulting from direct damage to the motor nuclei of the lower brainstem (CN V, VII, IX, X, XI, XII) or their peripheral axons.
Causes
- Motor neurone disease (progressive bulbar palsy - most common current cause)
- Guillain-Barre syndrome (acute)
- Poliomyelitis (historical)
- Diphtheritic neuropathy
- Syringobulbia
- Brainstem tumors, infarcts affecting nuclei directly
- Kennedy disease (bulbospinal muscular atrophy)
- Myasthenia gravis (neuromuscular junction - mimics bulbar palsy)
Clinical Features
Speech:
- Nasal dysarthria (palatal weakness - air escapes through nose)
- Difficulty with lingual consonants (r, n, l), labial consonants (b, m, p, f), dental (d, t) and palatal (k, g) consonants
- Syllables lose clarity and run together until speech becomes unintelligible
- Voice may be "wet" sounding due to pooled secretions
- Eventually aphonia
Swallowing (dysphagia):
- Initial difficulty with fluids (coughing, spluttering)
- Progresses to all consistencies
- Nasal regurgitation of liquids (palatal failure)
- Aspiration - repeated aspiration pneumonia
- Food lodges between cheek and teeth; bolus cannot be propelled into esophagus
Tongue:
- Atrophy (wasting - shriveled, lies on floor of mouth)
- Fasciculations - visible wriggling movements; may also be seen in facial muscles and palpated in masseter
- Weakness of tongue movement
Jaw:
- Weakness of jaw closure and opening
- Jaw jerk: absent or reduced (LMN)
Palate:
- Absent or reduced movement on phonation
- Absent gag reflex
Face:
- Facial muscle weakness and sagging (lower face)
- Chin fasciculations may be visible
Key LMN signs:
-
Muscle wasting/atrophy
-
Fasciculations
-
Hypotonia (flaccid)
-
Absent/reduced reflexes (jaw jerk, gag reflex)
-
No emotional lability
-
Adams and Victor's Principles of Neurology, Scott-Brown's Otorhinolaryngology
2. Pseudobulbar Palsy (UMN)
Definition
A bilateral upper motor neuron syndrome resulting from damage to the corticobulbar tracts - the descending pathways that provide supranuclear control to the brainstem motor nuclei. Because a single unilateral corticobulbar lesion is insufficient (bilateral cortical representation), both hemispheres must be damaged for pseudobulbar palsy to develop.
The prefix "pseudo" indicates the bulbar muscles themselves are not primarily affected and do not show atrophy.
Why Bilateral Lesions Are Required
Most lower cranial nerve nuclei receive equal bilateral supranuclear innervation. A unilateral corticobulbar lesion causes minimal or transient deficit. Only after a second contralateral lesion deprives the nuclei of the remaining 50% of supranuclear input does pseudobulbar palsy appear. - Scott-Brown's Otorhinolaryngology
Causes
- Bilateral cerebrovascular disease (bilateral capsular lacunar infarcts - most common; successive strokes)
- Multiple sclerosis (bilateral plaques)
- Motor neurone disease (UMN predominant - primary lateral sclerosis)
- Progressive supranuclear palsy (Steele-Richardson-Olszewski syndrome)
- Bilateral subdural hematomas
- Severe traumatic brain injury
Clinical Features
Speech:
- Spastic dysarthria - slow, strained, "hot potato" quality (as if food too hot in mouth)
- Harsh, strangled voice
- Slurred, monotonous, effortful speech
- Low pitch, reduced volume
Swallowing:
- Dysphagia - present but generally milder than in bulbar palsy
- Aspiration risk still present
- Saliva may accumulate in mouth (pooling)
Tongue:
- Small, spastic - slow movements
- No atrophy
- No fasciculations
- Tongue moves slowly but is not wasted
Jaw:
- Brisk jaw jerk (exaggerated) - pathological
- "Bulldog reflex" - jaw snaps shut involuntarily on mouth opening attempt (rare, severe cases)
- Jaw clonus may be elicited
Reflexes:
- Hyperactive gag reflex
- Brisk jaw jerk
- Snout reflex (pursing of lips when tapped)
- Suck reflex (regression of primitive reflexes)
- Forced/pathological yawning
Pathognomonic Feature - Emotional Lability (Pseudobulbar Affect):
- Involuntary, uncontrollable episodes of crying and laughing that are disproportionate to or incongruent with the patient's emotional state
- Also called: emotional incontinence, pathological laughter and crying (PLAC), involuntary emotional expression disorder
- The patient cannot control these outbursts and is often embarrassed
- In severe cases, laughing and crying are the only available forms of emotional expression - intermediate expressions (smiling, frowning) are lost
- Laughter and crying may merge into each other
Mechanism of pseudobulbar affect:
Two supranuclear pathways control laughing and crying:
- Corticobulbar pathway (posterior internal capsule limb) - controls volitional facial/vocal movements
- Anterior pathway (just rostral to genu of internal capsule) - contains facilitatory and inhibitory fibers
Bilateral damage to these descending pathways disinhibits pontomedullary laughing/crying circuits, producing uncontrolled emotional outbursts. Antidepressants (fluoxetine, imipramine) and dextromethorphan/quinidine (Nuedexta) can help suppress these episodes.
- Adams and Victor's Principles of Neurology
Other UMN signs may coexist:
- Bilateral limb spasticity and hyperreflexia
- Bilateral extensor plantar responses (Babinski)
- Small, brisk steps (marche à petits pas) if bilateral anterior circulation disease
- Cognitive slowing if severe bilateral white matter disease
3. Comparison Table
| Feature | Bulbar Palsy (LMN) | Pseudobulbar Palsy (UMN) |
|---|---|---|
| Lesion level | LMN - brainstem nuclei / nerves | UMN - bilateral corticobulbar tracts |
| Lesion required | Unilateral or bilateral medulla | Must be bilateral |
| Tongue | Wasted, fasciculating, flaccid | Small, spastic, no wasting |
| Fasciculations | Present | Absent |
| Tone (tongue/palate) | Flaccid (hypotonic) | Spastic (hypertonic) |
| Jaw jerk | Absent / reduced | Brisk / exaggerated |
| Gag reflex | Absent / reduced | Hyperactive |
| Snout/suck reflex | Absent | Present (primitive reflexes released) |
| Dysarthria type | Nasal, flaccid | Spastic, strained, "hot potato" |
| Emotional lability | Absent | Present (pathognomonic) |
| Dysphagia | Severe, early | Present but milder |
| Nasal regurgitation | Common | Less common |
| Limb signs | Absent (unless mixed) | Bilateral UMN signs often present |
| Common causes | MND, GBS, polio | Bilateral strokes, MND, MS, PSP |
4. Mixed Bulbar + Pseudobulbar Palsy
Amyotrophic lateral sclerosis (ALS/MND) is the classic condition where both LMN and UMN signs coexist simultaneously in the bulbar region - the only common clinical situation where both spastic (pseudobulbar) and atrophic (bulbar) features coexist. The jaw jerk may be brisk even when jaw muscles are wasted, and pathological laughing/crying may reach extreme degrees alongside fasciculations. - Adams and Victor's Principles of Neurology
5. Key Points for Clinical Distinction
- Fasciculations + wasting = bulbar palsy (LMN) until proven otherwise
- Emotional lability (crying/laughing) = pseudobulbar palsy (UMN) - this does not occur in pure LMN lesions
- Brisk jaw jerk = UMN (pseudobulbar); absent jaw jerk = LMN (bulbar)
- A single hemisphere stroke rarely causes persistent bulbar palsy - bilateral lesions required for pseudobulbar
- Myasthenia gravis is the most important differential for bulbar palsy (especially in the elderly) - the fatigability and variability should help distinguish, but atypical cases can be confusing
Why exacerbated jaw reflex in umn lesion
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Excellent - all the key anatomy and mechanism is clear. Here is the full explanation:
Why the Jaw Jerk Is Exaggerated in UMN Lesions
The Jaw Jerk Reflex Arc
The jaw jerk (masseter reflex) is a monosynaptic stretch reflex - the cranial nerve equivalent of the knee jerk.
Stimulus: Tapping the chin (or a spatula on the lower teeth) with the mouth slightly open stretches the masseter and temporalis muscles.
Afferent limb:
- Stretch is detected by muscle spindle Ia proprioceptive fibers in the masseter
- These Ia fibers travel in the mandibular division (V3) of the trigeminal nerve
- Uniquely, their cell bodies lie inside the CNS in the mesencephalic nucleus of the trigeminal nerve in the midbrain - the only case where primary sensory neurons reside within the CNS rather than in a peripheral ganglion
- Their central processes descend a short distance within the brainstem to synapse directly in the motor nucleus of CN V in the mid-pons
Efferent limb:
- Motor neurons of the trigeminal motor nucleus (mid-pons)
- Axons exit via the mandibular nerve (V3)
- Innervate the masseter and temporalis → jaw closes
This is a monosynaptic arc entirely within the pons/midbrain, analogous to the knee jerk arc in the spinal cord.
- Neuroanatomy Through Clinical Cases; Adams and Victor's Principles of Neurology
Why It Is Normally Minimal or Absent
In healthy individuals, the jaw jerk is minimal or absent - this distinguishes it from limb stretch reflexes which are normally brisk.
The reason: the trigeminal motor nucleus sits in the pons and receives continuous tonic descending inhibition via the corticobulbar (corticonuclear) tracts from both motor cortices. These descending UMN fibers exert a suppressive, modulating influence on the reflex arc - dampening the excitability of the trigeminal motor nucleus and its response to incoming Ia signals.
Think of it as the corticobulbar system holding the reflex under a restraining "lid."
Why It Becomes Exaggerated with a UMN Lesion
When bilateral corticobulbar tracts are damaged (unilateral lesions are insufficient because the trigeminal motor nucleus has bilateral supranuclear innervation):
- The descending inhibitory control is removed - the trigeminal motor nucleus is released from supraspinal suppression
- The motor neurons of CN V become hyperexcitable (disinhibited)
- Even a small jaw stretch now triggers a brisk, exaggerated contraction of the masseters - jaw snaps shut
This is the exact same mechanism that produces hyperreflexia at the knee (exaggerated patellar reflex) in spinal cord UMN lesions - removal of descending inhibitory modulation from the corticospinal tract makes spinal motor neurons hyperexcitable.
"Lesions anywhere along this reflex arc result in depression of the ipsilateral jaw reflex, whereas bilateral supranuclear lesions result in an accentuated response."
- Localization in Clinical Neurology, 8e
Why Bilateral Lesions Are Required
The trigeminal motor nucleus (unlike the lower facial nucleus) receives predominantly bilateral corticobulbar innervation. A unilateral UMN lesion (e.g., a single stroke) still leaves the motor nucleus with ~50% of its supranuclear input from the intact hemisphere - enough to maintain near-normal inhibitory tone.
Only when both corticobulbar tracts are damaged (bilateral strokes, ALS, diffuse white matter disease, MS) does the nucleus lose enough inhibitory drive to show clear hyperreflexia - hence the brisk jaw jerk is a sign of bilateral UMN/corticobulbar pathology, and its presence clinches pseudobulbar palsy.
Summary Diagram
Normal:
Motor cortex (bilateral)
|
Corticobulbar tracts ──► Trigeminal motor nucleus (INHIBITED)
↑
Mesencephalic nucleus ──► (weak reflex response)
UMN Lesion (bilateral corticobulbar damage):
Motor cortex ✗
|
Corticobulbar tracts ──✗──► Trigeminal motor nucleus (DISINHIBITED / hyperexcitable)
↑
Mesencephalic nucleus ──► BRISK jaw jerk (masseter snaps shut)
In short: The jaw jerk is exaggerated in bilateral UMN lesions because loss of bilateral corticobulbar inhibition disinhibits the trigeminal motor nucleus, making the monosynaptic masseter stretch reflex arc hyperreactive - the same mechanism as limb hyperreflexia in spinal cord UMN disease.
Difference between umn lesion and lmn lesion
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
All the key content is assembled. Here is the comprehensive comparison:
UMN vs. LMN Lesion: Complete Comparison
Anatomy First
Upper Motor Neuron (UMN): The first neuron in the motor pathway - from the motor cortex (precentral gyrus) down through the internal capsule, brainstem, and corticospinal/corticobulbar tracts to synapse on the anterior horn cell (or brainstem motor nucleus). Any lesion from the cortex to (but not including) the anterior horn cell is a UMN lesion.
Lower Motor Neuron (LMN): The final common pathway - from the anterior horn cell (or brainstem motor nucleus) through the nerve root, peripheral nerve, neuromuscular junction, to the muscle. Any lesion at or distal to the anterior horn cell is a LMN lesion.
Core Comparison Table
| Feature | UMN Lesion | LMN Lesion |
|---|---|---|
| Weakness | Yes | Yes |
| Muscle tone | Increased (spasticity) | Decreased (flaccidity) |
| Reflexes (DTRs) | Increased (hyperreflexia) | Decreased / absent (hyporeflexia) |
| Clonus | Present | Absent |
| Babinski sign | Positive (extensor plantar) | Absent (or flexor) |
| Hoffmann sign | May be present | Absent |
| Muscle atrophy | Absent (mild disuse atrophy late) | Prominent, early |
| Fasciculations | Absent | Present |
| Muscle bulk | Preserved | Wasted |
| Distribution of weakness | Distal > proximal; pyramidal pattern | Variable; often focal to nerve/root |
| Pattern (limbs) | Flexors weak in arm; extensors weak in leg | Depends on which nerve/root/segment |
| Abdominal reflexes | Absent (lost) | Preserved |
| Cremasteric reflex | Absent | Preserved |
| Jaw jerk | Brisk (if bilateral corticobulbar) | Absent/reduced |
| Plantar response | Extensor (upgoing toe - Babinski) | Flexor (normal) or absent |
| EMG | Normal (or reduced recruitment) | Fibrillations, fasciculations, denervation |
| Nerve conduction | Normal | Reduced/absent |
- Harrison's Principles of Internal Medicine 22e; Neuroanatomy Through Clinical Cases
1. Tone
UMN - Spasticity:
- Velocity-dependent increase in tone (resistance increases with faster passive stretch)
- "Clasp-knife" phenomenon - initial resistance suddenly gives way
- Affects antigravity muscles predominantly: flexors in the arm, extensors in the leg
- Due to loss of descending inhibitory control on the stretch reflex arc
LMN - Flaccidity:
- Muscle tone is reduced or absent
- Limb is floppy, soft
- Due to loss of gamma motor neuron input that maintains spindle tension
2. Reflexes
UMN:
- Deep tendon reflexes (DTRs) are exaggerated - disinhibited stretch reflex arcs
- Clonus - rhythmic oscillations on sustained stretch (e.g., ankle clonus)
- Pathological reflexes present:
- Babinski sign (extensor plantar - great toe dorsiflexes, toes fan out)
- Hoffmann sign (finger flexion on flicking middle fingernail)
- Snout, suck, grasp reflexes (frontal release signs)
- Superficial reflexes lost: abdominal reflexes, cremasteric reflex
LMN:
- DTRs are reduced or absent - the reflex arc itself is broken
- No pathological reflexes
- Plantar response may be absent or flexor (normal direction)
Important exception: Immediately after an acute UMN lesion (e.g., cord transection, acute stroke), there is a period of spinal shock - flaccidity, hyporeflexia, and absent Babinski. Spasticity and hyperreflexia develop gradually over hours to weeks as the spinal cord adapts.
3. Wasting and Fasciculations
UMN: Muscle bulk is preserved because the LMN - the neuron that directly trophically supports the muscle - is intact. Only mild disuse atrophy develops over time.
LMN: Prominent atrophy develops rapidly because:
- The trophic influence of the motor neuron on the muscle fiber is lost
- Denervated muscle fibers atrophy
Fasciculations (visible twitches from spontaneous motor unit discharge) are a hallmark of LMN/anterior horn cell disease - particularly motor neuron disease. They do not occur in pure UMN lesions. Fibrillation potentials (single-fiber discharges visible only on EMG) also occur with LMN lesions.
4. Distribution of Weakness
UMN pattern:
- Distal muscles affected more than proximal
- Upper limb: extensors weaker than flexors (extensors are "anti-gravity" in the arm - so they bear the pyramidal tract distribution)
- Lower limb: flexors weaker than extensors (e.g., foot drop)
- This is the pyramidal distribution of weakness
- Axial (trunk) movements are relatively spared unless bilateral or severe
- Corticobulbar lesions preferentially affect: lower face, tongue; spares upper face, extraocular muscles, jaw
LMN pattern:
- Distribution matches the anatomical territory of the affected nerve, root, or anterior horn segment
- Nerve lesion: follows peripheral nerve territory
- Root lesion: dermatomal/myotomal distribution
- Anterior horn: segmental pattern
5. UMN Syndrome: Positive vs. Negative Features
The UMN syndrome has two components - Bradley and Daroff's Neurology:
| Positive Features (gain of function) | Negative Features (loss of function) |
|---|---|
| Increased tendon reflexes with radiation | Muscle weakness |
| Clonus | Loss of dexterity |
| Babinski sign | Fatigability |
| Involuntary activation of remote muscles | Loss of selective muscle control |
| Spasticity | Nonmotor changes (cognition, behavior) |
| Flexor/extensor spasms |
Positive features are more amenable to treatment (e.g., baclofen for spasticity). Negative features (weakness, loss of dexterity) are more responsible for disability but harder to treat.
6. Common Causes
| UMN Lesions | LMN Lesions | |
|---|---|---|
| Brain | Stroke, tumor, MS, TBI, ALS | - |
| Brainstem | Stroke, MS, tumor | Motor neuron disease, syringobulbia |
| Spinal cord | Trauma, MS, cord compression, ALS | Anterior horn: polio, SMA, ALS |
| Nerve root | - | Disc prolapse, radiculopathy |
| Peripheral nerve | - | GBS, neuropathies, mononeuritis |
| NMJ / Muscle | - | Myasthenia gravis, myopathies (functionally similar) |
Quick Memory Aid
| UMN | LMN | |
|---|---|---|
| Tone | Up (spastic) | Down (flaccid) |
| Reflexes | Up (brisk) | Down (absent) |
| Wasting | No | Yes |
| Fasciculations | No | Yes |
| Babinski | Yes (extensor) | No |
A simple rule: UMN = everything up (tone, reflexes, pathological signs), LMN = everything down (tone, reflexes, muscle bulk gone).
This is a shared conversation. Sign in to Orris to start your own chat.