Lsn score
Reading File
Finding Sources
Finding Sources
Searching the Web
LSN score lung sonography neonates scoring system
Asking for Preferences
Finding Sources
Finding Sources
Searching the Web
LSN score liver stiffness NAFLD steatosis scoring system
Finding Sources
Searching the Web
"LSN score" liver NAFLD OR fibrosis OR steatosis
Now I have a clear answer. The LSN score stands for Liver Surface Nodularity (LSN) score - a CT-based imaging biomarker for liver fibrosis staging.
LSN Score - Liver Surface Nodularity Score
The LSN (Liver Surface Nodularity) score is a quantitative, imaging-based biomarker derived from routine abdominal CT scans to non-invasively assess and stage hepatic fibrosis, including in NAFLD/NASH.
How It Works
Liver fibrosis causes formation of fibrotic bands and regenerative nodules, which progressively increase the irregular ("nodular") contour of the liver surface. Software quantifies this nodularity automatically from CT images.
Measurement method:
- Imaging software detects the liver surface contour on CT
- The LSN score = average distance between the detected liver surface and a smoothed polynomial "best-fit" line
- 10 contiguous CT slices are evaluated (total distance: 80-100 cm)
- Final score = average of all slice scores, expressed in tenths of a millimeter
- Average processing time: <2 minutes
Score Range & Interpretation
| LSN Score | Interpretation |
|---|---|
| ~1.5 | Normal liver (F0) |
| 1.45-1.48 | F1 fibrosis range |
| >1.48 | Suggests F2+ fibrosis (cut-off in NAFLD) |
| 1.67+ | F2/F3 (advanced fibrosis) range |
| 1.5-5.0 | Typical range |
| >5.0 | Severe cirrhosis with marked nodularity |
- In NAFLD studies: Mean LSN - Normal controls: 1.30 ± 0.09, Simple steatosis: 1.54 ± 0.21, NASH: 1.59 ± 0.23
- Mean LSN by fibrosis grade: F0 = 1.30, F1 = 1.45, F2&F3 = 1.67
Diagnostic Accuracy for Hepatic Fibrosis Staging
From studies in HCV and NAFLD (AUC values):
| Fibrosis Stage | AUC Range |
|---|---|
| Early fibrosis (>F2) | 0.88-0.90 |
| Advanced fibrosis (>F3) | 0.89-0.93 |
| Cirrhosis (F4) | 0.90-0.96 |
- In NAFLD specifically: Cut-off LSN >1.48 distinguishes F1 from F2/F3 with sensitivity 83.3%, specificity 72.7%, AUROC 0.788
- Accuracy further improves when combined with FIB-4 index (age + AST + ALT + platelet count)
Reliability
- Inter-observer agreement: ICC 0.94 (CV 9%) - very high
- Test-retest reliability: ICC 0.82 (CV 12%)
- Software-based LSN has higher inter-observer agreement than subjective visual scoring (ICC 0.84 vs 0.61)
- Technical failure rate: approximately 0-3.9%
Uses
- Non-invasive fibrosis staging in NAFLD, NASH, HCV, and other chronic liver diseases
- Cirrhosis sub-staging - predicts hepatic decompensation and death
- Monitoring disease progression over time
- Reduces need for liver biopsy in many patients
Context Among Other NAFLD Scoring Tools
The LSN score is an imaging biomarker, distinct from serum-based scores. It complements:
- NFS (NAFLD Fibrosis Score) - uses age, BMI, hyperglycemia, AST/ALT, platelets, albumin
- FIB-4 - age, AST, ALT, platelets
- BARD score - BMI, AST/ALT ratio, diabetes
- LSM (Liver Stiffness Measurement) via FibroScan/transient elastography (in kPa)
The Scientific Reports paper by Hanaoka et al. (2019) first validated LSN specifically in NAFLD, while SAR/abdominal radiology resources provide detailed technical guidance on its CT-based application.
Liver surface nodularity
Finding Sources
Searching the Web
liver surface nodularity CT scoring fibrosis staging radiology
Searching PubMed
"liver surface nodularity" fibrosis CT imaging
Reading Web Page
liver surface nodularity score CT fibrosis staging measurement interpretation
Finding Sources
Searching PubMed
"liver surface nodularity" cirrhosis fibrosis
Reading File
Reading File
Reading Article
Loading Image
Here is a comprehensive overview of Liver Surface Nodularity (LSN).
Liver Surface Nodularity (LSN)
Pathophysiology
Progressive hepatic fibrosis causes the formation of fibrotic bands and regenerative nodules throughout the liver parenchyma. As fibrosis worsens, these changes distort the normally smooth liver capsule into an irregular, bumpy ("nodular") contour. LSN is therefore a morphological marker that reflects the degree of underlying fibrosis - the more advanced the fibrosis, the greater the surface irregularity.
Detection Methods
1. Ultrasound (Qualitative)
The most accessible method. Using a high-frequency linear array transducer directly on the liver surface, an irregular/nodular contour can be identified visually. This is one of the classic sonographic signs of cirrhosis, alongside:
- Right lobe atrophy with compensatory left lobe/caudate hypertrophy
- Parenchymal inhomogeneity
- Signs of portal hypertension (splenomegaly, varices, ascites)
However, ultrasound detection of nodularity is subjective and operator-dependent, with moderate sensitivity and specificity for cirrhosis detection.
Here is the sonographic appearance of liver surface nodularity in a cirrhotic liver (arrows indicate the bumpy contour, asterisk = ascites):
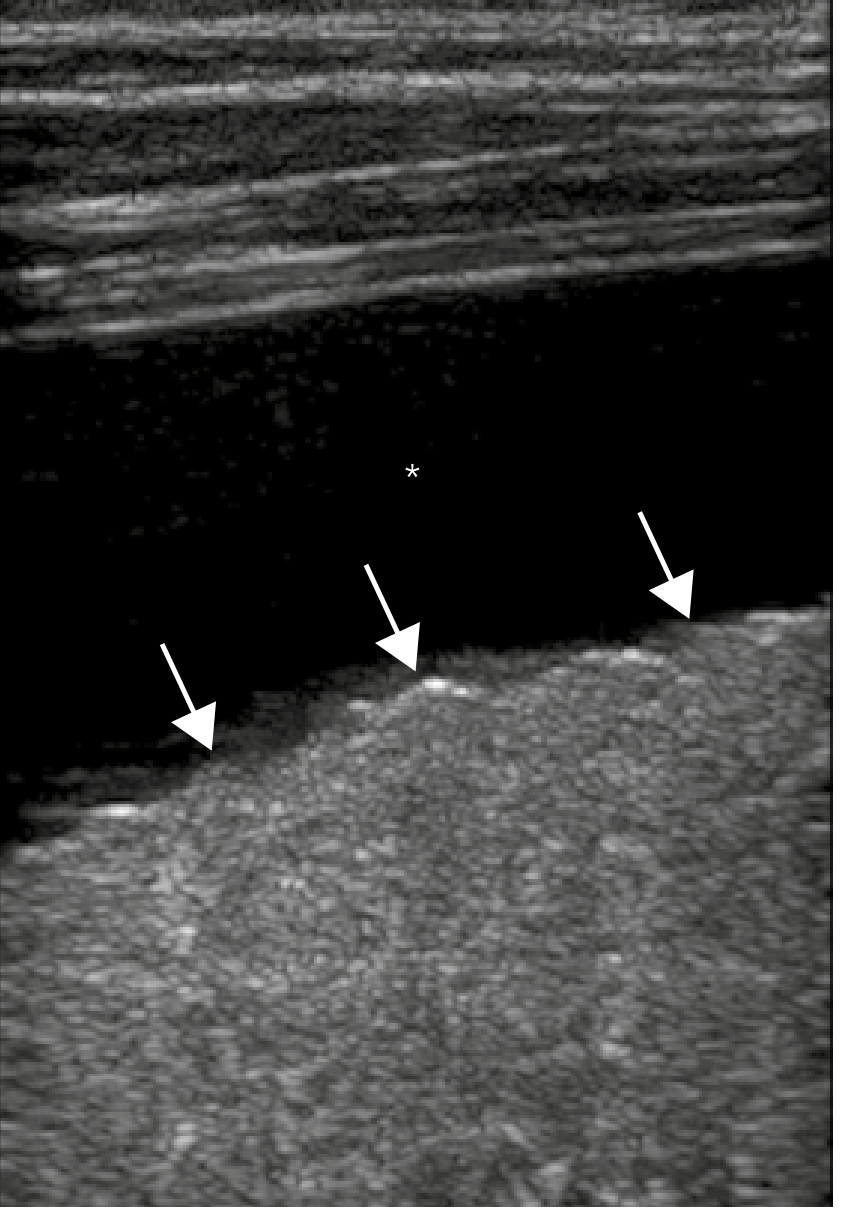
Yamada's Textbook of Gastroenterology, 7th ed. - Sonogram with high-frequency linear transducer showing nodular contour of cirrhotic liver (arrows) with moderate ascites (*).
2. CT - Quantitative LSN Score (Primary Method)
CT allows software-based quantification of liver surface nodularity, producing the LSN score (also called the "Liver Score"):
How it is measured:
- Imaging software automatically detects the liver surface outline on axial CT slices
- LSN score = average distance between the detected liver surface and a smoothed polynomial "best-fit" line
- 10 contiguous CT slices are evaluated (total coverage: 80-100 cm)
- Final score = average of all slice scores, expressed in tenths of a millimeter
- Processing time: <2 minutes
- Works on non-contrast and contrast-enhanced CT
Score ranges:
| LSN Score | Interpretation |
|---|---|
| ~1.30 | Normal liver (F0) |
| ~1.45 | Early fibrosis (F1) |
| >1.48 | Suggests F2+ (NAFLD cut-off) |
| ~1.67+ | Advanced fibrosis (F2-F3) |
| 1.5-5.0 | Typical clinical range |
| >5.0 | Severe/decompensated cirrhosis |
Diagnostic Accuracy for Fibrosis Staging (CT-based)
From HCV and NAFLD studies (AUC values):
| Target | AUC |
|---|---|
| Early fibrosis (>F2) | 0.88-0.90 |
| Advanced fibrosis (>F3) | 0.89-0.93 |
| Cirrhosis (F4) | 0.90-0.96 |
- In NAFLD specifically: cut-off LSN >1.48 differentiates F1 from F2/F3 with sensitivity 83%, specificity 73%, AUROC 0.788
- Accuracy further improves when combined with FIB-4 index (age + AST + ALT + platelet count)
Clinical Applications
- Non-invasive fibrosis staging in chronic liver disease (HCV, NAFLD/NASH, alcohol-related liver disease)
- Substaging of cirrhosis - the LSN score is a strong predictor of hepatic decompensation (variceal bleeding, encephalopathy, ascites) and death (Smith et al., Radiology 2017)
- Portal hypertension detection - LSN correlates with hepatic venous pressure gradient (Sartoris et al., Radiology 2018)
- Reducing liver biopsies - high negative predictive value for ruling out advanced fibrosis
- Retrospective staging from existing CT images (no additional scan needed)
Reliability
| Parameter | Value |
|---|---|
| Inter-observer reliability (ICC) | 0.94 (CV 9%) |
| Test-retest reliability (ICC) | 0.82 (CV 12%) |
| Software vs. visual scoring ICC | 0.84 vs. 0.61 |
| Technical failure rate | 0-3.9% |
Limitations and Contraindications
| Limitation | Detail |
|---|---|
| Ionizing radiation | Requires CT scan |
| Ascites | Fluid obscures liver surface detection |
| Very low BMI | No perihepatic fat = technical failure |
| Limited validation | Mainly HCV and NAFLD; less data for other CLD causes |
| Pregnancy | Relative contraindication (radiation) |
| Software requirement | Needs dedicated post-processing software |
MRI-Based LSN
Emerging MRI-compatible LSN software has been developed (Hanaoka et al., 2019) that applies the same measurement principle to MRI images, offering the advantage of no ionizing radiation. Validation is still ongoing before clinical implementation.
Context Among Non-Invasive Fibrosis Tools
| Tool | Type | Modality |
|---|---|---|
| LSN score | Quantitative morphology | CT/MRI |
| LSM (FibroScan) | Liver stiffness | Ultrasound elastography |
| MR Elastography | Liver stiffness | MRI |
| FIB-4 | Serum biomarker | Blood |
| NAFLD Fibrosis Score | Serum biomarker | Blood |
| BARD score | Serum biomarker | Blood |
A 2024 review (Zheng et al., Abdom Radiol 2024, PMID 38372765) places LSN among the most promising quantitative imaging biomarkers for cirrhosis, alongside elastography, extracellular volume fraction, and diffusion-weighted imaging parameters.
This is a shared conversation. Sign in to Orris to start your own chat.