Best medicines to prevent the attach of acute urticaria in previously chronic urticaria patient
Reading File
Finding Sources
Searching PubMed
"chronic urticaria" AND "prevention" AND antihistamine
Searching the Web
prevention acute urticaria attacks chronic urticaria guidelines 2024 2025 medications
Reading File
Reading File
Searching PubMed
"chronic urticaria" AND "omalizumab" AND treatment
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the information needed to provide a comprehensive, well-structured answer. Here's the full synthesis:
Preventing Acute Urticaria Attacks in a Patient with Chronic Urticaria
The goal in a patient with known chronic urticaria (CU) is suppressing ongoing mast cell activation to prevent episodic acute flares. Management follows a stepwise approach based on international guidelines (EAACI/GA²LEN/EDF/WAO):
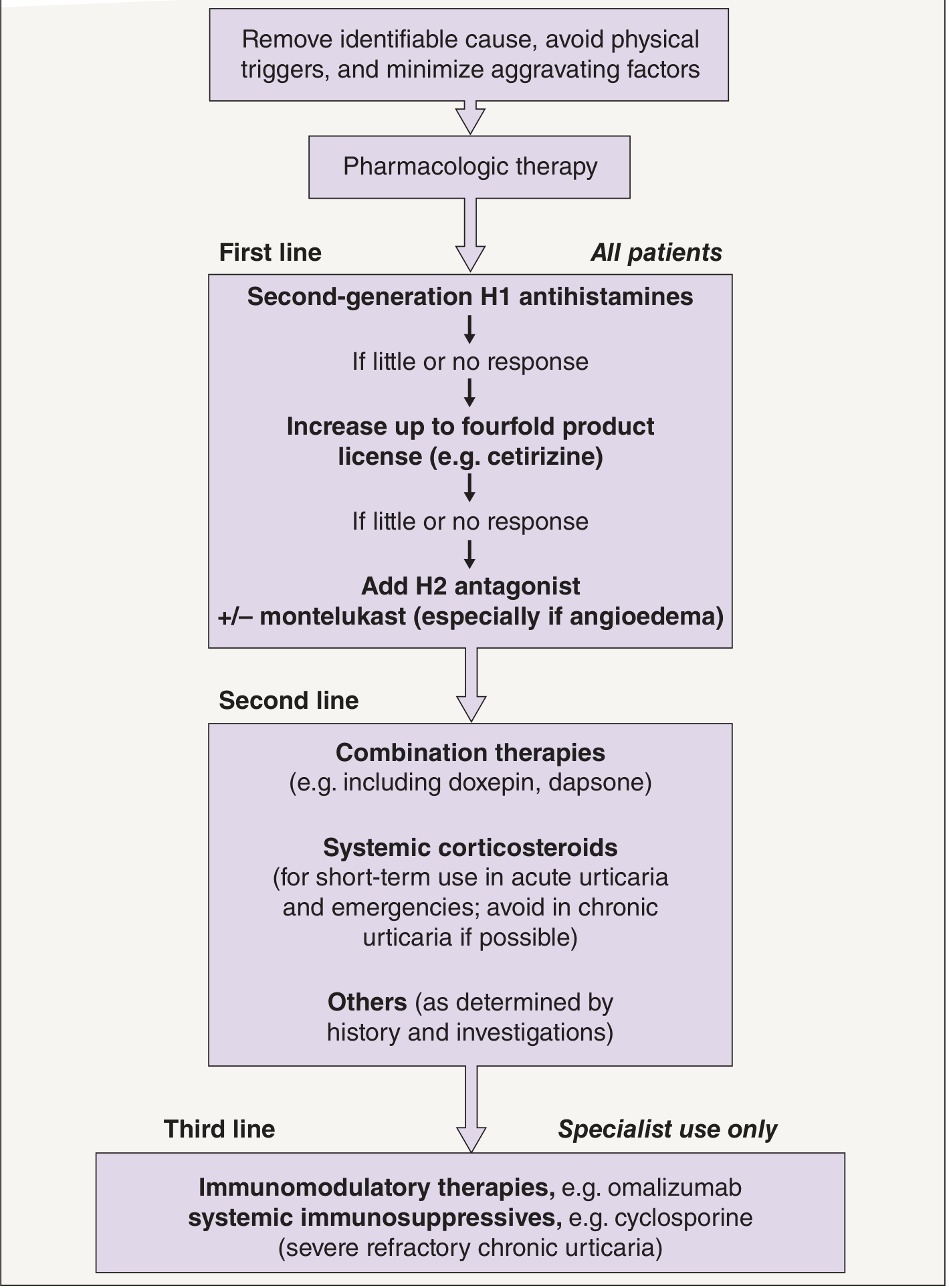
Step 0 — Non-pharmacologic Foundation
Before any drug, address modifiable triggers:
- Remove identifiable causes (foods, drugs, infections, NSAIDs, ACE inhibitors)
- Avoid physical triggers (cold, pressure, exercise, sunlight depending on subtype)
- Minimize aggravating factors (aspirin/NSAIDs worsen ~30% of CU patients)
🥇 First Line — Second-Generation H1 Antihistamines (All Patients)
These are the backbone of prevention. They are safe, non-sedating, and taken daily (not just on-demand) to prevent attacks.
| Drug | Standard Dose | Notes |
|---|---|---|
| Cetirizine | 10 mg once daily | Can up-dose to 40 mg/day |
| Levocetirizine | 5 mg once daily | Active enantiomer of cetirizine |
| Loratadine | 10 mg once daily | Preferred in pregnancy |
| Desloratadine | 5 mg once daily | Long half-life (27 h) |
| Fexofenadine | 180 mg once daily | Licensed specifically for urticaria |
| Bilastine | 20 mg once daily | Half-life 14.5 h, no food interactions |
| Rupatadine | 10 mg once daily | Also PAF antagonist activity |
Key principle: If the standard dose provides inadequate control, increase up to fourfold (e.g., cetirizine 40 mg/day). Guidelines strongly recommend against sedating first-generation antihistamines as monotherapy. — Dermatology 5e
If still insufficient → add H2 antagonist (famotidine 20 mg twice daily) ± montelukast (leukotriene receptor antagonist, especially useful if angioedema is present or aspirin sensitivity).
🥈 Second Line — Combination & Short-Term Bridge Therapies
When first-line antihistamines (even at high doses) fail to prevent attacks:
Doxepin
- Tricyclic antidepressant with potent H1 + H2 blocking activity
- Dose: 10–50 mg at night
- Useful when sleep is disturbed by urticaria
Systemic Corticosteroids (Short-term only)
- Prednisolone used as a rescue/bridge for acute flare management
- Not recommended for chronic daily use due to predictable long-term side effects (hypertension, weight gain, glucose intolerance, osteoporosis) and rebound on cessation
- Suitable for brief courses (5–7 days) during breakthrough flares
Dapsone
- Evidence is limited but used as adjunct in refractory cases, particularly neutrophilic urticaria or urticarial vasculitis
🥉 Third Line — Specialist Immunomodulatory Therapies (Refractory CU)
Omalizumab (Anti-IgE monoclonal antibody) ✅ Most Important
- 300 mg subcutaneously every 4 weeks is the approved dose for chronic spontaneous urticaria (CSU)
- Rapidly reduces urticaria activity scores; onset within 1–4 weeks in responders
- Approved for adults and children ≥12 years (and off-label in younger children)
- Mechanism: neutralizes free IgE → downregulates FcεRI on mast cells/basophils
- Recent 2024 network meta-analysis (PMID 39673624) confirms omalizumab 300 mg q4w as the most cost-effective dose
- 2025 WAO position paper (PMID 39732405) provides consensus on remission criteria and stepping down therapy
- A 2025 network meta-analysis (PMID 41186128) comparing omalizumab, dupilumab, and remibrutinib showed omalizumab remains first among biologics
Cyclosporine (Ciclosporin)
- 2–5 mg/kg/day for severe refractory autoimmune CU (positive autologous serum skin test)
- Suppresses mast cell and T-cell activation
- Monitor renal function and blood pressure; limited to short courses (3–6 months)
- Goldman-Cecil: "For recurrent chronic spontaneous urticaria, cyclosporine or omalizumab therapy can be very effective"
Emerging Agents (Post-2024)
- Remibrutinib (BTK inhibitor) — showing promising results in phase III trials for CSU
- Dupilumab — IL-4/IL-13 blockade; emerging evidence in antihistamine-refractory CSU
Acute Attack ("Rescue") Management
When a breakthrough attack occurs despite prophylaxis:
| Severity | Drug |
|---|---|
| Mild–moderate | Extra-dose antihistamine + short course oral prednisolone |
| Severe/angioedema | IM epinephrine (adrenaline) — treatment of choice for anaphylactic/severe angioedema presentations |
| Oropharyngeal angioedema | IM/SC epinephrine; keep auto-injector (EpiPen) prescribed |
Summary Table — Prevention Ladder
| Line | Drug Class | Example | Role |
|---|---|---|---|
| 1st | 2nd-gen H1 antihistamine | Cetirizine 10–40 mg/day | Daily prophylaxis |
| 1st (adjunct) | H2 antagonist | Famotidine 20 mg BD | Add-on to H1 |
| 1st (adjunct) | Leukotriene antagonist | Montelukast 10 mg/day | Add-on, esp. angioedema |
| 2nd | Tricyclic antihistamine | Doxepin 10–50 mg nocte | Refractory/sleep disruption |
| 2nd | Corticosteroid | Prednisolone (short-term) | Acute flares only |
| 3rd | Anti-IgE biologic | Omalizumab 300 mg SC q4w | Refractory CSU |
| 3rd | Calcineurin inhibitor | Cyclosporine 2–5 mg/kg/day | Autoimmune CU |
Sources:
- Dermatology 2-Volume Set, 5e (Bolton/Burns, Figs. 18.20, Table 18.5)
- Fitzpatrick's Dermatology, Fig. 41-7 (EAACI/WAO treatment algorithm)
- Goldman-Cecil Medicine, International Edition (Ch. 407)
- Recent evidence: WAO position paper 2025 | Omalizumab network meta-analysis 2024 | Biologics comparative NMA 2025
This is a shared conversation. Sign in to Orris to start your own chat.