Provide me appropriate images to fit in the empty space left for images
LVNC left ventricular non-compaction echocardiogram trabeculations pediatric
ARVC arrhythmogenic right ventricular cardiomyopathy cardiac MRI fatty replacement
restrictive cardiomyopathy CMR biatrial enlargement pediatric
pediatric echocardiogram cardiac ultrasound child heart
Atypical Cardiomyopathy Pediatrics WithImages
Presentation · PPTX
Hello
The second presentation is mine i want you to make my presentation to look similar to the first one. Without changing my original content
Metabolic Disorders Monitoring
Presentation · PPTX
| Design Element | Applied |
|---|---|
| A4 Portrait (8.27" × 11.69") | ✅ Same layout size |
| Dark navy blue (#0D2B55) header bar + slide background (title) | ✅ |
| Red accent line under header | ✅ |
| Dark navy footer bar with topic name + page number | ✅ |
| Blue section headers (#1A78C2) with white bold text | ✅ |
| Red section headers (#B51212) for alternate sections | ✅ |
| Light blue content panels (#E8F1FA) for bullet content | ✅ |
| Gold "⚡ Key Points" callout boxes (#FFF8E1 with gold left bar) | ✅ |
| Comparison table at bottom of last slide | ✅ |
| Two-column layout on content slides | ✅ |
- Title slide — your name, institution, topic
- Introduction to Metabolic Disorders
- Importance of Long-Term Monitoring
- Risk Factors
- Symptoms
- Treatment & Management (with comparison table)
I told you to create on the topic "Atypical forms of cardiomyopathy in children and adolescents." You have done the opposite. I want you to create a pdf similar to the metabolic disorder presentation i gave you
Atypical Cardiomyopathy Pediatrics PDF
PDF Document · PDF
| Feature | Your PDF | This PDF |
|---|---|---|
| Format | A4 portrait | A4 portrait ✅ |
| Page 1 | Cover: University name + topic | Jalalabad State University, Faculty of Medicine + topic ✅ |
| Page 2 | Formal title page (Ministry header) | Ministry of Education header, same details ✅ |
| Pages 3–8 | Heading + paragraph body text | Same structure ✅ |
| Last page | "THANK YOU" | "THANK YOU" ✅ |
| Author/year/group | Snigdha Mandaokar, 4th, 8th | Same ✅ |
- Introduction to atypical cardiomyopathies
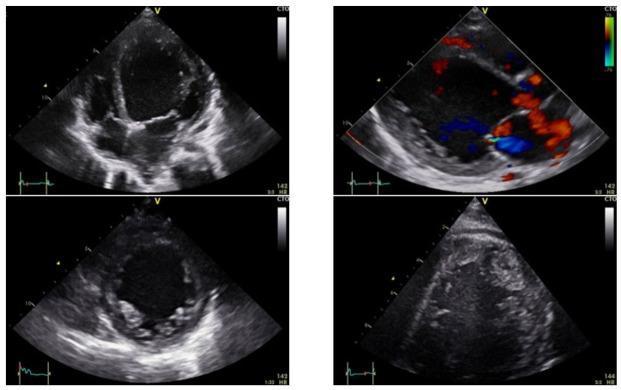
- Left Ventricular Non-Compaction (LVNC)
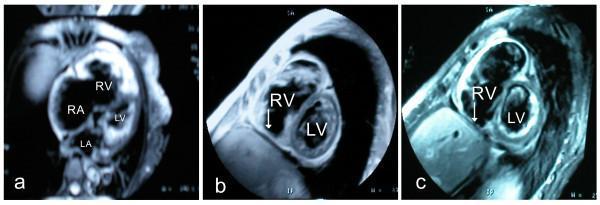
- Arrhythmogenic Cardiomyopathy (ACM/ARVC)
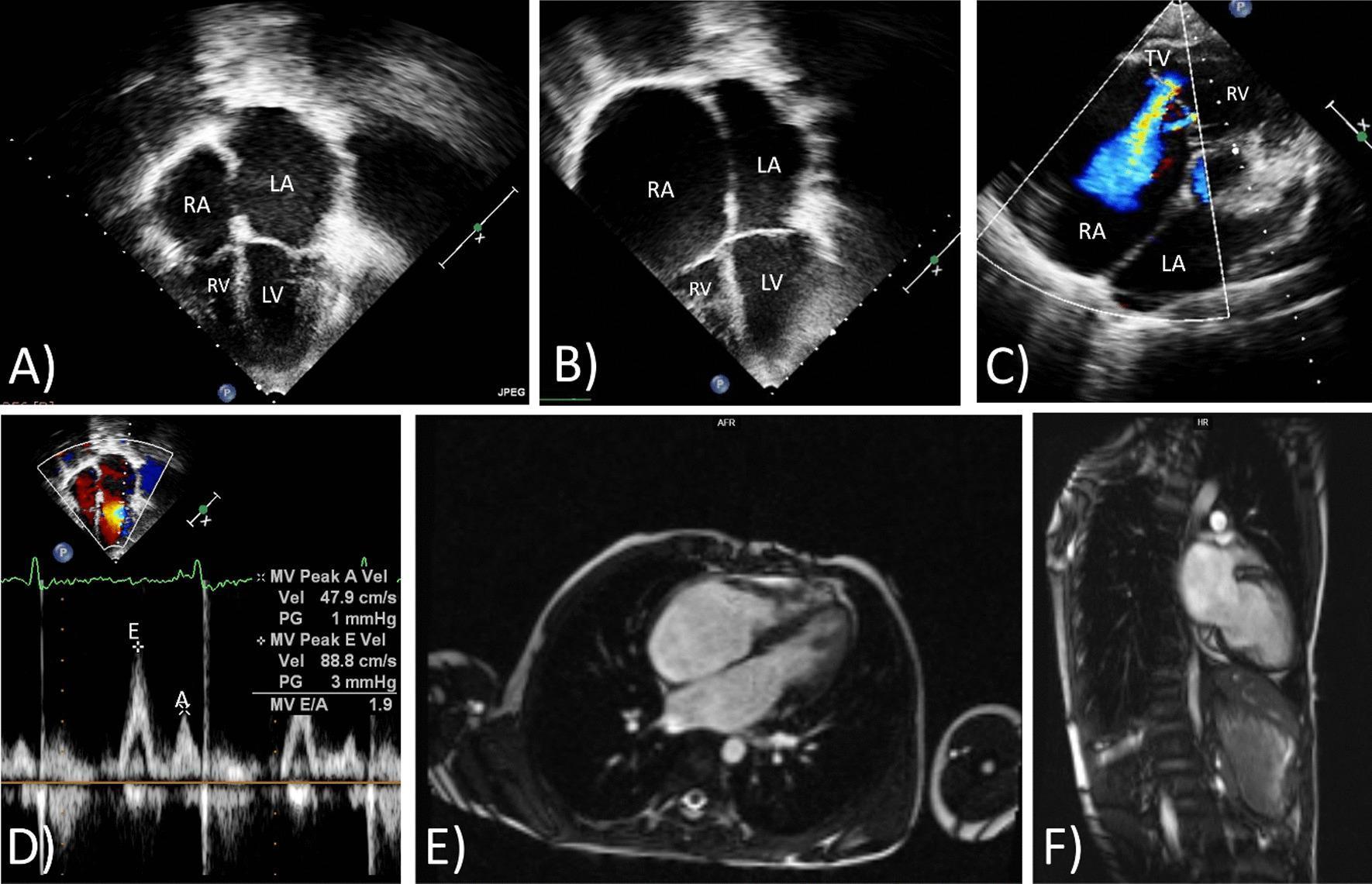
- Restrictive Cardiomyopathy (RCM)
- Other Atypical Forms (Takotsubo, Myocarditis, Metabolic, PPCM)
- Treatment and Management
- Thank You
Add some related images on each page and make the background layout colour full. This pdf looks boring make it more attractive
LVNC left ventricular non-compaction echocardiogram trabeculations pediatric
ARVC arrhythmogenic right ventricular cardiomyopathy cardiac MRI epsilon wave ECG
restrictive cardiomyopathy biatrial enlargement echocardiogram pediatric
Takotsubo cardiomyopathy apical ballooning echocardiogram stress cardiomyopathy
pediatric heart cardiomyopathy cardiac anatomy illustration children
Atypical Cardiomyopathy Colorful
PDF Document · PDF
| Page | Content | Color Theme | Image |
|---|---|---|---|
| 1 | Cover | Dark navy + gold + crimson | — |
| 2 | Formal title page | Navy + teal institutional | — |
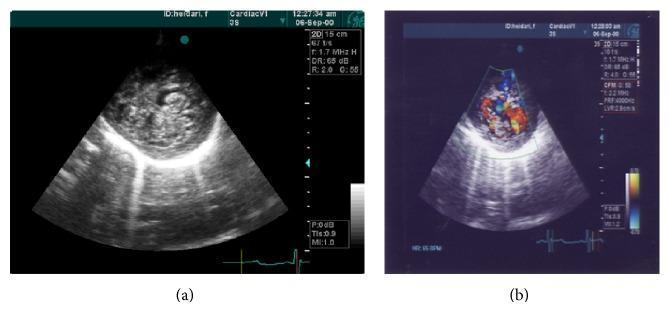
| 3 | Introduction | Navy blue | Pediatric echo (DCM) |
| 4 | LVNC | Teal | LVNC echo with trabeculations |
| 5 | ACM/ARVC | Purple | ECG epsilon wave + MRI fibrofatty RV |
| 6 | RCM | Crimson | CXR cardiomegaly + echo biatrial enlargement |
| 7 | Other Atypical Forms | Green | Takotsubo apical ballooning echo |
| 8 | Treatment & Management | Orange | Pediatric VAD + echo |
| 9 | Thank You | Navy | — |
- Colored header band (different color per page)
- Tinted background per page (no more plain white)
- Gold accent stripe under every header
- Left accent sidebar stripe
- Medical images framed with colored border + caption badge
- Rounded section pills and callout boxes
- Matching footer bar on every page
My name is Raghul Balaji.Make this pdf presentation into black and white and increase the size of the images . I don't want you to make change in any of the content. Don't spoil the originality
Okay I need this type of format by mentioning time Patient name,age,BP,diagnosis,patient Complaint,clinical Findings and treatment Plan.The name should be the names if kyrgyz people because I'm studying mbbs in Kyrgyzstan.Then my posting is under ENT department ,so give me situations according to that
══════════════════════════════════════════════════════════════════
ENT DEPARTMENT — PATIENT LOG
Jalalabad State University Hospital
Student: Raghul Balaji | 4th Year MBBS
══════════════════════════════════════════════════════════════════
─────────────────────────────────────────────────────────────────
CASE 01
─────────────────────────────────────────────────────────────────
Time : 09:10 AM
Patient Name : Айгүл Маматова (Aigul Mamatova)
Age : 28 years | Female
BP : 118/76 mmHg
Diagnosis : Acute Tonsillitis
─────────────────────────────────────────────────────────────────
Chief Complaint : Severe sore throat for 3 days, difficulty
swallowing, and fever.
─────────────────────────────────────────────────────────────────
Clinical Findings:
• Temperature: 38.6°C
• Oropharynx: Bilateral tonsillar enlargement (Grade II),
erythema, and exudative white patches on tonsils
• Tender bilateral anterior cervical lymphadenopathy
• Uvula midline, no peritonsillar bulge
─────────────────────────────────────────────────────────────────
Treatment Plan :
• Amoxicillin 500 mg TDS × 7 days
• Paracetamol 500 mg SOS for fever/pain
• Throat gargles with warm saline (4× daily)
• Adequate oral hydration; soft diet
• Review after 5 days; tonsillectomy counselling if recurrent
═════════════════════════════════════════════════════════════════
─────────────────────────────────────────────────────────────────
CASE 02
─────────────────────────────────────────────────────────────────
Time : 09:45 AM
Patient Name : Бакыт Дүйшөнов (Bakyt Duishonov)
Age : 42 years | Male
BP : 134/88 mmHg
Diagnosis : Chronic Suppurative Otitis Media (CSOM) —
Tubotympanic type
─────────────────────────────────────────────────────────────────
Chief Complaint : Recurrent ear discharge from the right ear
for 6 months, associated with decreased hearing.
─────────────────────────────────────────────────────────────────
Clinical Findings:
• Right ear: Mucopurulent discharge; central perforation of
tympanic membrane (anteroinferior quadrant)
• Left ear: Normal TM, no discharge
• Weber test: Lateralizes to right (affected) ear
• Rinne test: Negative on right (conductive hearing loss)
• No facial nerve palsy; no mastoid tenderness
─────────────────────────────────────────────────────────────────
Treatment Plan :
• Aural toilet (dry mopping) of right ear
• Ciprofloxacin ear drops 3 drops TDS × 2 weeks
• Oral Amoxicillin-Clavulanate 625 mg BD × 7 days
• Audiogram and high-resolution CT temporal bones
• Refer to senior ENT for tympanoplasty counselling
• Advise: keep ear dry, avoid swimming
═════════════════════════════════════════════════════════════════
─────────────────────────────────────────────────────────────────
CASE 03
─────────────────────────────────────────────────────────────────
Time : 10:15 AM
Patient Name : Нургүл Токтоматова (Nurgul Toktomatova)
Age : 7 years | Female
BP : 96/64 mmHg
Diagnosis : Adenoid Hypertrophy with Obstructive
Sleep-Disordered Breathing
─────────────────────────────────────────────────────────────────
Chief Complaint : Mouth breathing, snoring at night, and nasal
obstruction for 4 months (reported by mother).
─────────────────────────────────────────────────────────────────
Clinical Findings:
• Adenoid facies: open mouth posture, elongated face
• Nasal endoscopy: large adenoid pad obstructing >75%
of the nasopharyngeal airway
• Bilateral tympanic membranes dull/retracted (Eustachian
tube dysfunction)
• Tonsils: Grade I–II bilaterally
• No stridor at rest
─────────────────────────────────────────────────────────────────
Treatment Plan :
• Mometasone nasal spray 1 puff each nostril OD × 6 weeks
• Montelukast 4 mg OD (adjunct for allergic component)
• Lateral neck X-ray: confirm adenoid-nasopharyngeal ratio
• Polysomnography if apnea episodes confirmed by parents
• Surgical referral: adenoidectomy ± grommet insertion
═════════════════════════════════════════════════════════════════
─────────────────────────────────────────────────────────────────
CASE 04
─────────────────────────────────────────────────────────────────
Time : 10:50 AM
Patient Name : Эрлан Жакшылыков (Erlan Zhakshy lykov)
Age : 55 years | Male
BP : 148/92 mmHg
Diagnosis : Epistaxis (Anterior) — Hypertension-related
─────────────────────────────────────────────────────────────────
Chief Complaint : Sudden onset bleeding from the left nostril
for 20 minutes, not stopping with pinching.
─────────────────────────────────────────────────────────────────
Clinical Findings:
• Active bleeding from left nostril; Little's area erythematous
with visible vessel on anterior nasal septum
• BP at presentation: 164/98 mmHg (elevated)
• No posterior pharyngeal blood clots visible
• No nasal trauma history; no anticoagulant use
• SpO₂: 98% on room air
─────────────────────────────────────────────────────────────────
Treatment Plan :
• Immediate: Seat patient upright, lean forward; pinch
cartilaginous nose for 10–15 minutes
• Silver nitrate cauterisation of bleeding vessel (Little's area)
• Anterior nasal packing (BIPP/Vaseline gauze) if cautery fails
• Amlodipine 5 mg OD — initiate antihypertensive therapy
• BP monitoring every 30 min for 2 hours post-procedure
• Refer to medicine for hypertension management
• Avoid nose-blowing and strenuous activity for 5 days
═════════════════════════════════════════════════════════════════
─────────────────────────────────────────────────────────────────
CASE 05
─────────────────────────────────────────────────────────────────
Time : 11:30 AM
Patient Name : Зарина Асанова (Zarina Asanova)
Age : 34 years | Female
BP : 120/78 mmHg
Diagnosis : Allergic Rhinitis (Perennial)
─────────────────────────────────────────────────────────────────
Chief Complaint : Persistent nasal blockage, watery nasal
discharge, sneezing, and itchy eyes for 1 year,
worse in dusty environments.
─────────────────────────────────────────────────────────────────
Clinical Findings:
• Nasal mucosa pale and boggy; clear watery rhinorrhoea
• Inferior turbinates hypertrophied bilaterally
• Allergic salute sign present
• Eyes: mild bilateral conjunctival injection
• No nasal polyps visible on anterior rhinoscopy
• Skin prick test: positive for house dust mite, mold
─────────────────────────────────────────────────────────────────
Treatment Plan :
• Fluticasone nasal spray 2 puffs each nostril OD
• Cetirizine 10 mg OD (at bedtime)
• Saline nasal irrigation BD
• Allergen avoidance: dust-proof pillowcase, reduce carpets
• Consider allergen immunotherapy if poorly controlled
after 3 months
═════════════════════════════════════════════════════════════════
─────────────────────────────────────────────────────────────────
CASE 06
─────────────────────────────────────────────────────────────────
Time : 12:05 PM
Patient Name : Канат Осмонов (Kanat Osmonov)
Age : 19 years | Male
BP : 112/72 mmHg
Diagnosis : Acute Otitis Externa (Swimmer's Ear)
─────────────────────────────────────────────────────────────────
Chief Complaint : Right ear pain and itching for 4 days,
worsened after swimming; slight discharge.
─────────────────────────────────────────────────────────────────
Clinical Findings:
• Right ear: Tragal tenderness ++; pinna traction pain ++
• EAC: Oedematous, erythematous; scant serous discharge
• Tympanic membrane partially visible but intact
• Left ear: Normal
• No fever; no lymphadenopathy
─────────────────────────────────────────────────────────────────
Treatment Plan :
• Gentle aural toilet; suction clearance of debris
• Ciprofloxacin + Dexamethasone ear drops 4 drops QID × 7 days
• Wick insertion (Pope wick) if canal too swollen for drops
• Oral ibuprofen 400 mg TDS for pain relief
• Strict water precautions: ear plugs when bathing
• Review in 7 days
═════════════════════════════════════════════════════════════════
─────────────────────────────────────────────────────────────────
CASE 07
─────────────────────────────────────────────────────────────────
Time : 12:40 PM
Patient Name : Гүлбарчын Исакова (Gulbarchyn Isakova)
Age : 62 years | Female
BP : 142/86 mmHg
Diagnosis : Benign Paroxysmal Positional Vertigo (BPPV)
— Posterior semicircular canal (right)
─────────────────────────────────────────────────────────────────
Chief Complaint : Brief episodes of spinning dizziness triggered
by rolling over in bed and looking up, for 2 weeks.
─────────────────────────────────────────────────────────────────
Clinical Findings:
• Dix-Hallpike test (right): Positive — upbeat-torsional
nystagmus with 5-second latency, fatigable
• Dix-Hallpike (left): Negative
• Neurological exam: No focal deficits, gait normal
• Otoscopy: Bilateral normal TMs
• No hearing loss; no tinnitus
─────────────────────────────────────────────────────────────────
Treatment Plan :
• Epley canalith repositioning manoeuvre (right side) —
performed in clinic; vertigo resolved post-procedure
• Betahistine 16 mg TDS × 2 weeks (symptomatic relief)
• Home Brandt-Daroff exercises (BD × 2 weeks)
• Advise: avoid sudden head movements; fall precautions
• BP follow-up with physician
• Review in 2 weeks; repeat Dix-Hallpike to confirm resolution
═════════════════════════════════════════════════════════════════
─────────────────────────────────────────────────────────────────
CASE 08
─────────────────────────────────────────────────────────────────
Time : 02:00 PM
Patient Name : Мирлан Кадыров (Mirlan Kadyrov)
Age : 38 years | Male
BP : 126/80 mmHg
Diagnosis : Deviated Nasal Septum (DNS) with
Secondary Sinusitis
─────────────────────────────────────────────────────────────────
Chief Complaint : Left-sided nasal obstruction since childhood,
now with recurrent headaches and facial pain
for 3 months.
─────────────────────────────────────────────────────────────────
Clinical Findings:
• Anterior rhinoscopy: C-shaped DNS to the left; nasal spur
at osteocartilaginous junction
• Left turbinate: Compensatory hypertrophy
• Facial tenderness over left maxillary sinus region
• Nasal endoscopy: mucopus in left middle meatus
• X-ray PNS (Waters view): Haziness of left maxillary sinus
─────────────────────────────────────────────────────────────────
Treatment Plan :
• Amoxicillin-Clavulanate 625 mg BD × 10 days
• Mometasone nasal spray OD × 4 weeks
• Saline nasal irrigation TDS
• CT PNS (coronal cuts) to assess sinus disease extent
• Surgical referral: Septoplasty ± FESS (Functional
Endoscopic Sinus Surgery)
═════════════════════════════════════════════════════════════════
─────────────────────────────────────────────────────────────────
CASE 09
─────────────────────────────────────────────────────────────────
Time : 02:35 PM
Patient Name : Адалат Эгембердиева (Adalat Egemberdieva)
Age : 15 years | Female
BP : 108/68 mmHg
Diagnosis : Peritonsillar Abscess (Quinsy) — Left side
─────────────────────────────────────────────────────────────────
Chief Complaint : Progressive severe sore throat for 5 days,
now with inability to open mouth fully and
muffled voice.
─────────────────────────────────────────────────────────────────
Clinical Findings:
• Temperature: 39.1°C
• Trismus present (mouth opening ~2 cm)
• Left peritonsillar bulge with uvular deviation to the right
• Left tonsil pushed inferomedially; fluctuance on palpation
• Hot potato (muffled) voice
• Tender left jugulodigastric lymph node
─────────────────────────────────────────────────────────────────
Treatment Plan :
• IV Benzylpenicillin 1.2 g QID + Metronidazole 500 mg TDS
• IV Dexamethasone 8 mg stat (reduces oedema, trismus)
• Needle aspiration of abscess under LA — 4 mL pus drained
• IV fluids (maintenance); soft diet when tolerated
• Upgrade to incision & drainage if aspiration insufficient
• Tonsillectomy (interval) recommended after 6 weeks
(quinsy tonsillectomy counselled)
═════════════════════════════════════════════════════════════════
─────────────────────────────────────────────────────────────────
CASE 10
─────────────────────────────────────────────────────────────────
Time : 03:10 PM
Patient Name : Темирбек Султанов (Temirbek Sultanov)
Age : 47 years | Male
BP : 138/84 mmHg
Diagnosis : Sudden Sensorineural Hearing Loss (SSNHL)
— Left ear
─────────────────────────────────────────────────────────────────
Chief Complaint : Sudden complete hearing loss in the left ear
on waking this morning, associated with
tinnitus and mild vertigo.
─────────────────────────────────────────────────────────────────
Clinical Findings:
• Otoscopy: Bilateral normal TMs; no discharge
• Tuning fork:
– Weber: Lateralizes to right (normal) ear
– Rinne: AC > BC bilaterally (sensorineural pattern left)
• Audiogram: Left ear — profound SNHL across all frequencies
• MRI IAC: Ordered to exclude acoustic neuroma / MS
• No facial palsy; no preceding URTI
─────────────────────────────────────────────────────────────────
Treatment Plan :
• Prednisolone 1 mg/kg/day (max 60 mg) OD × 7 days,
then taper over 5 days — URGENT (within 24–48 hrs)
• Intratympanic dexamethasone injection if systemic steroids
contraindicated or fail
• Carbogen (95% O₂ + 5% CO₂) inhalation therapy
• Urgent audiogram and BERA (Brainstem Evoked Response)
• Strict bed rest; avoid noise exposure
• Prognosis counselling: 30–65% recovery with early treatment
═════════════════════════════════════════════════════════════════
─────────────────────────────────────────────────────────────────
CASE 11
─────────────────────────────────────────────────────────────────
Time : 03:45 PM
Patient Name : Жылдыз Бекова (Zhyldyz Bekova)
Age : 31 years | Female
BP : 116/74 mmHg
Diagnosis : Vocal Cord Nodules (Singer's Nodules)
─────────────────────────────────────────────────────────────────
Chief Complaint : Progressive hoarseness of voice for 4 months,
worse with prolonged speaking; works as a
school teacher.
─────────────────────────────────────────────────────────────────
Clinical Findings:
• Voice: Rough, breathy dysphonia; reduced volume
• Indirect laryngoscopy / Flexible nasolaryngoscopy:
Bilateral whitish nodules at the anterior 1/3–2/3
junction of vocal cords ("kissing nodules")
• Vocal cords mobile; no mucosal irregularity
• No neck lymphadenopathy
• GERD symptoms present (throat clearing, post-nasal drip)
─────────────────────────────────────────────────────────────────
Treatment Plan :
• Voice rest: reduce speaking to minimum for 2 weeks
• Speech therapy (voice hygiene training) × 6–8 sessions
• Pantoprazole 40 mg BD × 4 weeks (treat GERD component)
• Adequate hydration; avoid caffeine and smoking
• Microlaryngoscopy + excision if no improvement after
6–8 weeks of conservative therapy
• Occupational advice: voice amplifier at work
═════════════════════════════════════════════════════════════════
─────────────────────────────────────────────────────────────────
CASE 12
─────────────────────────────────────────────────────────────────
Time : 04:20 PM
Patient Name : Болот Чоротегин (Bolot Chorotegin)
Age : 9 years | Male
BP : 98/62 mmHg
Diagnosis : Foreign Body Nose — Left nostril (bead)
─────────────────────────────────────────────────────────────────
Chief Complaint : Foul-smelling unilateral nasal discharge from
left nostril for 10 days (reported by mother;
child denies inserting anything).
─────────────────────────────────────────────────────────────────
Clinical Findings:
• Left nostril: Purulent malodorous discharge; mucosa
erythematous and swollen
• Anterior rhinoscopy: Small round blue bead visible in
left nasal cavity, anterior floor
• Right nostril: Normal
• No signs of respiratory distress
─────────────────────────────────────────────────────────────────
Treatment Plan :
• Mother's kiss technique attempted — unsuccessful
• Removal under direct visualisation using Jobson-Horne
probe and Tilley's forceps; bead extracted successfully
• Nasal mucosa inspected post-removal: intact, no ulceration
• Saline nasal drops BD × 3 days
• Parent counselling: keep small objects away from child
• No antibiotics needed (discharge resolved on removal)
═════════════════════════════════════════════════════════════════
─────────────────────────────────────────────────────────────────
CASE 13
─────────────────────────────────────────────────────────────────
Time : 04:55 PM
Patient Name : Салтанат Токтогулова (Saltanat Toktogulova)
Age : 53 years | Female
BP : 150/94 mmHg
Diagnosis : Chronic Rhinosinusitis with Nasal Polyposis
─────────────────────────────────────────────────────────────────
Chief Complaint : Complete nasal blockage, loss of smell, and
chronic headache for over 1 year; not
responding to prior nasal sprays.
─────────────────────────────────────────────────────────────────
Clinical Findings:
• Anterior rhinoscopy: Bilateral pale grey semi-translucent
polyps prolapsing from middle meatus; Grade III polyposis
• Anosmia confirmed (smell identification test)
• CT PNS: Bilateral opacification of ethmoid and maxillary
sinuses; osteomeatal complex blocked bilaterally
• No features of malignancy (irregular margins, bony erosion)
─────────────────────────────────────────────────────────────────
Treatment Plan :
• Prednisolone 30 mg OD × 14 days (oral steroid reduction)
• Mometasone nasal spray 2 puffs BD (maintenance long-term)
• Saline nasal irrigation TDS
• Allergy evaluation; Aspirin sensitivity testing
• Surgical referral: FESS (bilateral) — polypectomy +
ethmoidectomy + middle meatal antrostomy
• Post-FESS steroid nasal spray indefinitely to prevent
recurrence
• BP follow-up with physician
═════════════════════════════════════════════════════════════════
─────────────────────────────────────────────────────────────────
CASE 14
─────────────────────────────────────────────────────────────────
Time : 05:30 PM
Patient Name : Улукбек Мамытбеков (Ulukbek Mamytbekov)
Age : 24 years | Male
BP : 122/78 mmHg
Diagnosis : Acute Laryngitis with Dysphonia
─────────────────────────────────────────────────────────────────
Chief Complaint : Complete loss of voice (aphonia) for 2 days
following a cold; mild throat pain and dry
cough.
─────────────────────────────────────────────────────────────────
Clinical Findings:
• Temperature: 37.8°C (low-grade fever)
• Voice: Aphonic; forced whisper only
• Flexible laryngoscopy: Bilateral vocal cords erythematous
and oedematous; no ulcers, no mass, no stridor
• Anterior cervical mild lymphadenopathy
• No respiratory distress; SpO₂ 99%
─────────────────────────────────────────────────────────────────
Treatment Plan :
• Complete voice rest × 5–7 days (absolute silence)
• Steam inhalation TDS × 5 days
• Benzydamine hydrochloride throat spray (anti-inflammatory)
• Paracetamol 500 mg TDS for discomfort
• Avoid whispering (as harmful as speaking)
• Adequate hydration; humidifier advised
• Reassess in 10 days; laryngoscopy if dysphonia persists
> 3 weeks (exclude malignancy)
═════════════════════════════════════════════════════════════════
─────────────────────────────────────────────────────────────────
CASE 15
─────────────────────────────────────────────────────────────────
Time : 06:00 PM
Patient Name : Нурбек Эсенгулов (Nurbek Esengulov)
Age : 16 years | Male
BP : 110/70 mmHg
Diagnosis : Otitis Media with Effusion (Glue Ear) —
Bilateral
─────────────────────────────────────────────────────────────────
Chief Complaint : Bilateral hearing difficulty and a sensation
of fullness in both ears for 2 months;
teacher reports inattentiveness in class.
─────────────────────────────────────────────────────────────────
Clinical Findings:
• Otoscopy: Bilateral amber/yellow TMs, retracted; loss of
light reflex; fluid level visible behind left TM
• Rinne: AC < BC bilaterally (conductive hearing loss)
• Weber: Midline (bilateral equal loss)
• Pure Tone Audiogram: Bilateral 30–35 dB conductive HL
• Tympanogram: Bilateral type B (flat curves)
• Nasopharyngoscopy: Mild adenoid hypertrophy
─────────────────────────────────────────────────────────────────
Treatment Plan :
• Watchful waiting for 6–8 weeks (first-line if < 3 months)
• Autoinflation (Valsalva / Otovent balloon) TDS
• Intranasal steroid spray (Mometasone) OD × 6 weeks
• Adenoidectomy + bilateral grommet (ventilation tube)
insertion if no resolution at 8-week review
• Hearing therapy and classroom seating advice
(front row, face teacher)
• Audiological re-evaluation at 8-week follow-up
══════════════════════════════════════════════════════════════════
END OF DAILY LOG
ENT Department | Jalalabad State University
══════════════════════════════════════════════════════════════════
| # | Diagnosis | Key Teaching Point |
|---|---|---|
| 1 | Acute Tonsillitis | Exudative, Group A Strep |
| 2 | CSOM Tubotympanic | Central perforation, safe type |
| 3 | Adenoid Hypertrophy | Adenoid facies, pediatric |
| 4 | Anterior Epistaxis | Little's area, hypertensive |
| 5 | Allergic Rhinitis | Perennial, dust mite |
| 6 | Otitis Externa | Swimmer's ear, tragal tenderness |
| 7 | BPPV | Epley manoeuvre, Dix-Hallpike |
| 8 | DNS + Sinusitis | Septoplasty + FESS |
| 9 | Peritonsillar Abscess | Quinsy, trismus, hot potato voice |
| 10 | SSNHL | Steroid emergency within 48 hrs |
| 11 | Vocal Cord Nodules | Teacher, voice therapy |
| 12 | Foreign Body Nose | Child, bead, mother's kiss |
| 13 | Nasal Polyposis | Grade III, FESS indication |
| 14 | Acute Laryngitis | Aphonia, voice rest |
| 15 | Glue Ear (OME) | Grommets, tympanogram type B |
Export these 15 cases as a printable PDF document
Purchase a top-up for immediate access to convert the 15 ENT cases to PDF

Don't change the originality just make sure every text and number looks same and font and font side similar if not correct only those and give me a flawless image