Digestive system
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
I now have rich material from multiple authoritative textbooks. Here is a comprehensive overview of the digestive system.
The Digestive System
1. Overview and Components
The digestive system consists of the alimentary canal (a continuous tube from mouth to anus) plus associated organs: tongue, teeth, salivary glands, pancreas, liver, and gallbladder. Its four major functions are:
- Transport - moving ingested water and food along the canal
- Secretion - releasing fluids, electrolytes, and digestive enzymes
- Digestion and absorption - chemical breakdown and uptake of nutrients
- Excretion - eliminating indigestible remains as feces
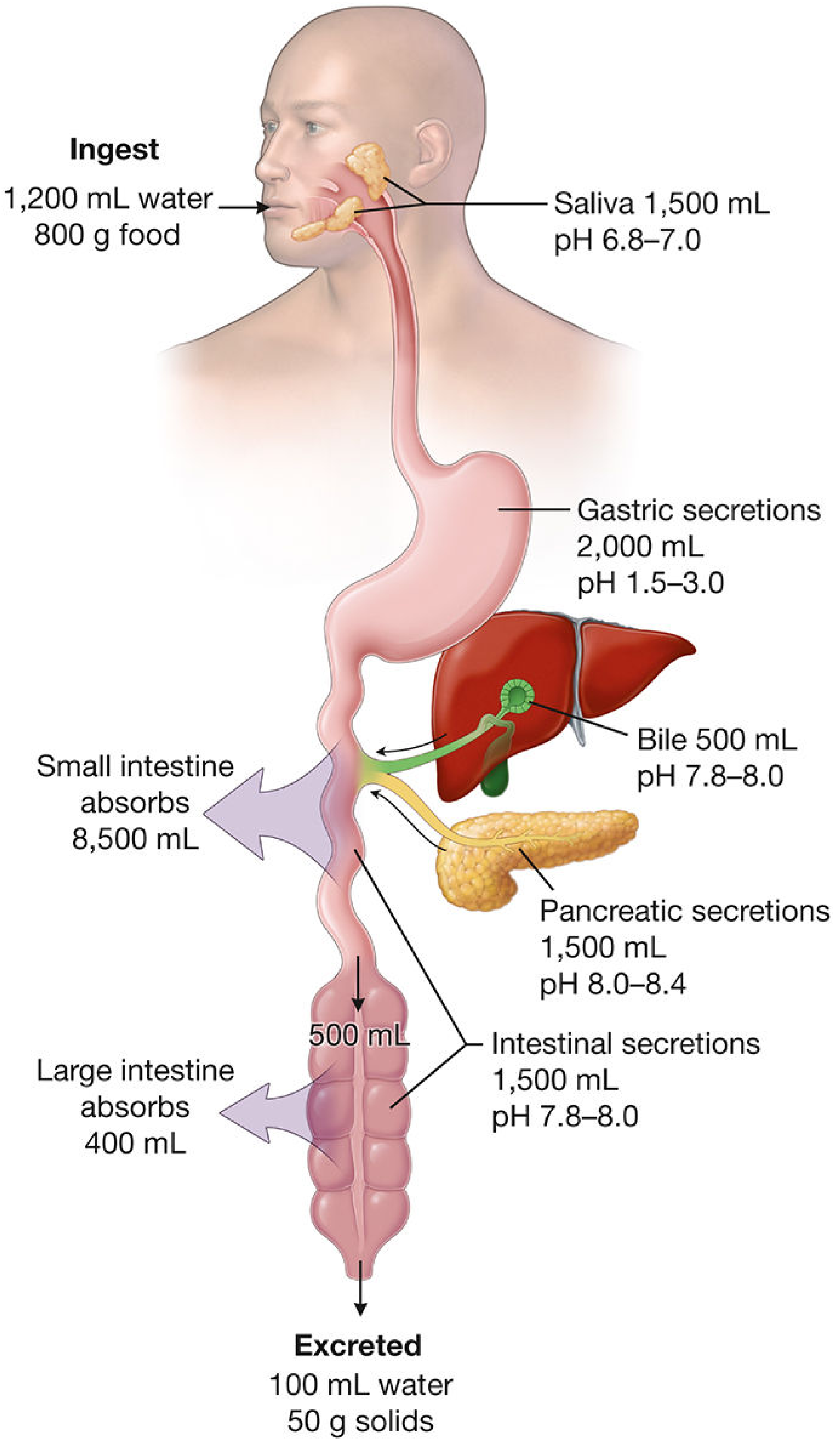
Approximately 2 L of water and food are ingested per day, while the total secretions from salivary glands, stomach, pancreas, intestines, and bile can amount to ~7 L/day. Almost all of this fluid is reclaimed - mainly in the small intestine - and only ~100 mL water and ~50 g solids are excreted as feces. - Histology: A Text and Atlas, p. 1409
2. Anatomy - Segment by Segment
Oral Cavity
- Bounded by the lips/cheeks, hard/soft palates, tongue, and entrance to the oropharynx
- Contains the teeth (incisors for cutting, molars for grinding - max force ~200 lb on molars), tongue, and three paired major salivary glands:
- Parotid (largest) - opens at parotid papilla opposite the 2nd upper molar via Stensen's duct
- Submandibular - opens at the sublingual caruncle via Wharton's duct
- Sublingual - opens via multiple short ducts
- Salivary secretion = ~1,500 mL/day at pH 6.8-7.0; contains salivary amylase (begins starch digestion) and mucin (lubricates the bolus)
- Waldeyer's tonsillar ring (palatine, tubal, pharyngeal tonsils, lingual tonsil) provides immunologic protection at the entrance to both the digestive and respiratory tracts
Esophagus
- A muscular conduit that propels the bolus by peristalsis
- Upper third = skeletal muscle; lower third = smooth muscle; middle = mixed
- Lower esophageal sphincter (LES) prevents gastroesophageal reflux
Stomach
- Secretes ~2,000 mL gastric juice/day at pH 1.5-3.0
- Key secretions: HCl (from parietal cells), pepsinogen (from chief cells), intrinsic factor (parietal cells, essential for B12 absorption), and mucus
- Mechanically churns food into chyme; empties into the duodenum at a controlled rate via the pyloric sphincter
- The enteroendocrine cells release gastrin (stimulates acid), which is in turn inhibited by somatostatin
Small Intestine (~6-7 m)
Divided into: duodenum (receives bile + pancreatic juice), jejunum (primary absorption site), and ileum (B12 and bile salt reabsorption)
- Structural adaptations massively increase absorptive surface area: plicae circulares (circular folds), villi (finger-like projections), and microvilli (brush border on enterocytes) - together expanding surface area ~600-fold
- Receives bile (500 mL/day, pH 7.8-8.0), pancreatic secretions (1,500 mL/day, pH 8.0-8.4), and intestinal secretions (1,500 mL/day)
- Absorbs ~8,500 mL fluid per day
Large Intestine (~1.5 m)
- Divided into: cecum, ascending, transverse, descending, sigmoid colon, rectum, and anal canal
- Primary function: water and electrolyte absorption (~400 mL/day), and compaction of feces
- Houses the gut microbiome (trillions of bacteria); ferments undigested carbohydrates
- No villi; contains goblet cells secreting mucus for lubrication
Accessory Organs
| Organ | Key Function |
|---|---|
| Liver | Bile production, detoxification, metabolism of absorbed nutrients (first-pass effect via portal circulation) |
| Gallbladder | Stores and concentrates bile; releases it in response to CCK |
| Pancreas | Exocrine: secretes amylase, lipase, proteases (trypsin, chymotrypsin); Endocrine: insulin, glucagon |
3. Physiology - Digestion and Absorption
Digestion is the chemical breakdown of food; absorption is the movement of nutrients from the lumen into blood. Two routes exist:
- Cellular (transcellular) - substances cross the apical membrane, pass through the enterocyte, and exit via the basolateral membrane
- Paracellular - substances pass through tight junctions between epithelial cells
Summary of Nutrient Digestion and Absorption
| Nutrient | Products | Site | Mechanism |
|---|---|---|---|
| Carbohydrates | Glucose, galactose, fructose | Small intestine | Na⁺-glucose/galactose cotransport (SGLT1); fructose via facilitated diffusion (GLUT5) |
| Proteins | Amino acids, di/tripeptides | Small intestine | Na⁺-amino acid cotransport; H⁺-peptide cotransport |
| Lipids | Fatty acids, monoglycerides, cholesterol | Small intestine | Bile salt micelles aid solubilization; diffusion into enterocytes; repackaged as chylomicrons → lymphatics |
| Fat-soluble vitamins (A, D, E, K) | - | Small intestine | Absorbed with lipid micelles |
| Vitamin B12 | - | Ileum | Requires intrinsic factor (from gastric parietal cells) |
| Calcium | Ca²⁺ | Small intestine | Vitamin D-dependent Ca²⁺-binding protein |
| Iron | Fe²⁺ (reduced from Fe³⁺) | Small intestine | Binds apoferritin in enterocyte → transferrin in blood |
| Bile salts | - | Ileum | Na⁺-bile salt cotransport (enterohepatic circulation) |
- Costanzo Physiology, 7th Ed., Table 8.6
4. Motility
- Mastication (chewing) - breaks food physically; exposes it to digestive enzymes; jaw muscles innervated by CN V
- Swallowing (deglutition) - involuntary pharyngeal phase; rapid passage protects the airway
- Peristalsis - rhythmic, coordinated smooth muscle contractions propelling contents forward
- Segmentation - localized contractions mixing contents without net forward movement (predominant in the small intestine)
- Mass movements - powerful colonic contractions occurring 1-3 times/day, triggered by the gastrocolic reflex after eating
- Defecation reflex - controlled by internal (involuntary) and external (voluntary) anal sphincters
The enteric nervous system (ENS) - often called the "second brain" - contains ~500 million neurons in the myenteric (Auerbach) and submucosal (Meissner) plexuses. It can regulate gut function largely independently of the CNS, though it is modulated by the sympathetic and parasympathetic systems.
5. GI Hormones (Key Four)
| Hormone | Secreted By | Stimulated By | Actions |
|---|---|---|---|
| Gastrin | G cells (stomach) | Peptides, distension, vagus | ↑ HCl, ↑ pepsin, ↑ motility |
| Secretin | S cells (duodenum) | Acid in duodenum | ↑ Pancreatic HCO₃⁻, ↓ gastric acid |
| CCK (cholecystokinin) | I cells (duodenum) | Fats, proteins | ↑ Pancreatic enzymes, gallbladder contraction |
| GIP | K cells (duodenum) | Glucose, fat | ↑ Insulin release, ↓ gastric motility |
6. The Mucosa as a Barrier
The alimentary mucosa is the interface between the body and the external environment. Beyond absorption and secretion, it performs:
- Barrier function - prevents entry of toxins, antigens, and pathogens
- Immunologic protection - gut-associated lymphoid tissue (GALT), including Peyer's patches in the ileum, forms the largest immune organ in the body
- Endocrine function - over 20 types of enteroendocrine cells produce hormones regulating digestion and satiety
7. Common Digestive Disorders (Summary)
| Disorder | Key Mechanism |
|---|---|
| GERD | LES incompetence → acid reflux → esophagitis |
| Peptic ulcer disease | H. pylori infection or NSAIDs disrupt mucosal barrier; acid erosion |
| Celiac disease | Immune reaction to gluten → villous atrophy → malabsorption |
| IBD (Crohn's / UC) | Dysregulated immune response to gut microbiota |
| Irritable bowel syndrome | Disordered gut motility and visceral hypersensitivity; no structural lesion |
| Colorectal cancer | Adenoma-carcinoma sequence; driven by APC, KRAS, TP53 mutations |
| Pancreatitis | Premature activation of pancreatic enzymes (often gallstones or alcohol) |
| Cirrhosis | Progressive hepatic fibrosis from chronic injury (alcohol, hepatitis, NASH) |
Sources: Histology: A Text and Atlas with Correlated Cell and Molecular Biology (Eroschenko) | Costanzo Physiology, 7th Ed. | Ganong's Review of Medical Physiology, 26th Ed. | Guyton and Hall Textbook of Medical Physiology
Blood
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Finding Sources
Finding Sources
I now have excellent material from multiple authoritative textbooks. Here is the comprehensive overview.
Blood
Blood is a specialized connective tissue - fluid in character - consisting of plasma (the liquid extracellular component) and formed elements (cells and cell fragments suspended within it). Total blood volume is approximately 70 mL/kg in adult women and 80 mL/kg in adult men. - Medical Physiology (Boron & Boulpaep)
1. Composition - The Big Picture
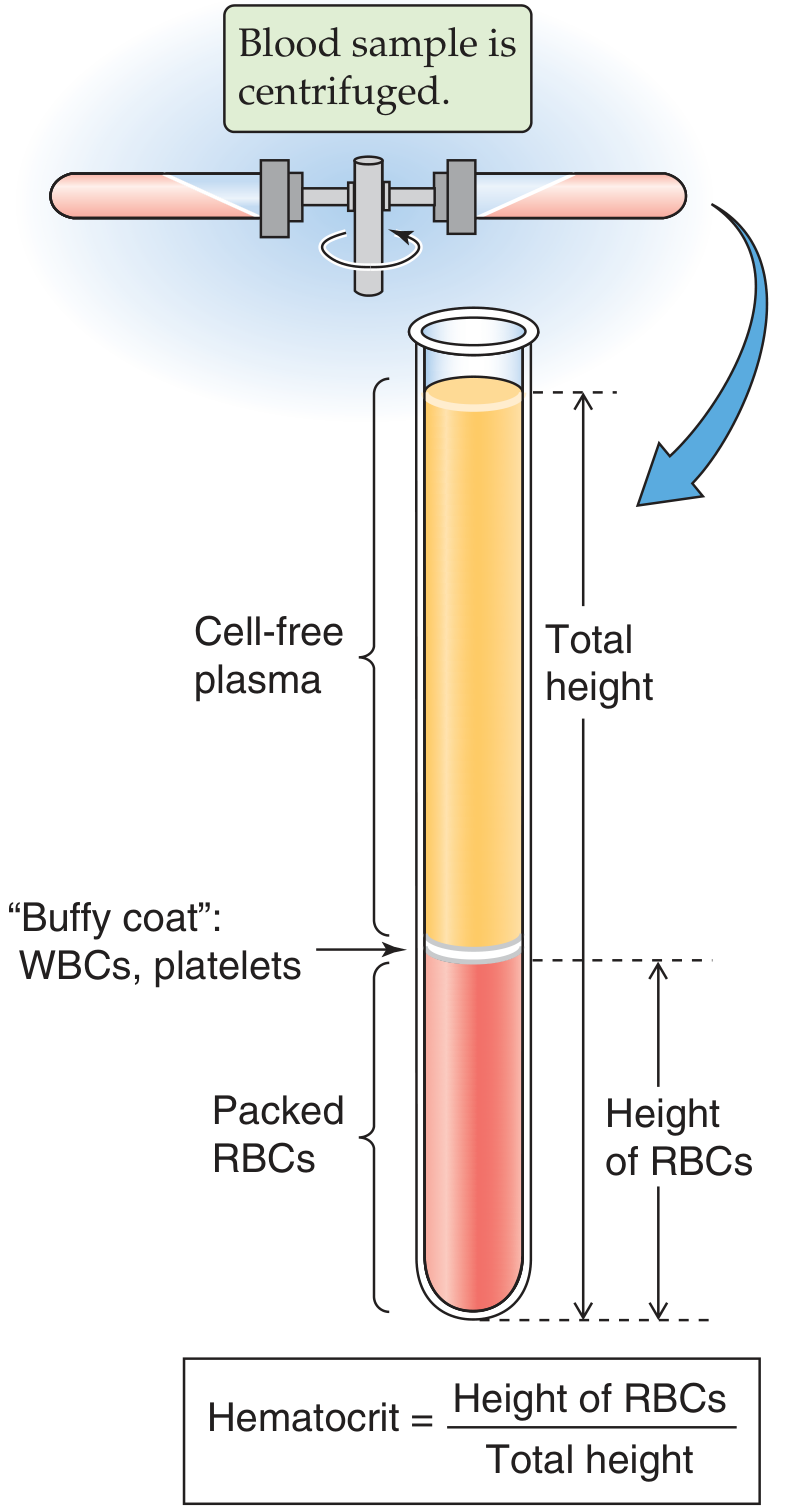
When a blood sample is centrifuged, it separates into three visible layers:
| Layer | Contents | % of Blood Volume |
|---|---|---|
| Plasma (top) | Water, proteins, electrolytes, hormones | ~55% |
| Buffy coat (middle) | WBCs (leukocytes) + platelets | <1% |
| Packed RBCs (bottom) | Erythrocytes | ~45% (= hematocrit) |
Normal hematocrit: ~45% in men, ~40% in women. At birth it is ~55%, drops to ~35% at 2 months, then rises to adult values at puberty.
2. Plasma
Plasma is a pale-yellow solution of:
- Water (~92%)
- Electrolytes - Na⁺, K⁺, Ca²⁺, Cl⁻, HCO₃⁻ (similar in composition to interstitial fluid)
- Plasma proteins (~7 g/dL total), generating an oncotic (colloid osmotic) pressure of ~25 mmHg
Key Plasma Proteins
| Protein | Molecular Weight | Major Functions |
|---|---|---|
| Albumin (3.5-5.5 g/dL) | 69 kDa | Oncotic pressure; binds steroids, T3, bilirubin, bile salts, fatty acids |
| Fibrinogen | 340 kDa | Clotting; contributes to ESR in inflammation |
| α1-antitrypsin | 54 kDa | Protease inhibitor; deficiency causes emphysema |
| Haptoglobin | 100 kDa | Binds free hemoglobin |
| Transferrin | 80 kDa | Transports iron |
| α2-macroglobulin | 725 kDa | Broad-spectrum protease inhibitor |
| LDL (β-lipoprotein) | 380 kDa | Lipid transport |
| IgG | 150 kDa | Antibody (humoral immunity) |
Albumin is synthesized by the liver at ~120 mg/kg/day with a plasma half-life of ~20 days. It is decreased in hepatic cirrhosis, nephrotic syndrome, and malnutrition.
Clinical note: Pink plasma = hemolysis (free hemoglobin). Brown-green plasma = elevated bilirubin. Cloudy plasma = cryoglobulinemia or hyperlipidemia.
ESR: Fibrinogen released during the acute-phase response causes RBCs to cluster, increasing their sedimentation rate. Normal ESR ≤15 mm/hr; markedly elevated in inflammatory disorders (e.g., temporal arteritis, multiple myeloma, lupus).
3. Red Blood Cells (Erythrocytes)
- Shape: Biconcave disc, 7.8 µm diameter, 2.5 µm thick at rim, ~1 µm at center. Volume 90-95 µm³
- Count: 5.2 million/µL (men), 4.7 million/µL (women)
- Life span: ~120 days; destroyed in the spleen and liver
- Structure: Anucleate; packed with hemoglobin (~34 g/100 mL of cells)
- Flexibility: The biconcave shape gives excess membrane relative to cell volume - this lets RBCs deform to squeeze through capillaries as narrow as 3 µm
Hemoglobin
Hemoglobin is a tetramer of 4 globin chains, each bound to an iron-containing heme group. One gram of Hgb carries 1.34 mL O₂ when fully saturated.
| Type | Adult % | Notes |
|---|---|---|
| HbA (α2β2) | ~96% | Predominant adult form |
| HbA2 (α2δ2) | ~3% | Elevated in β-thalassemia trait |
| HbF (α2γ2) | <1% (>1% fetal) | High O₂ affinity; predominant in fetus |
Normal Hgb: 15 g/dL (men), 14 g/dL (women)
O₂ carrying capacity: ~20 mL O₂/100 mL blood (men)
Other RBC Functions
- Carry carbonic anhydrase - converts CO₂ + H₂O ⇌ H₂CO₃ (→ HCO₃⁻) at 1000× normal rate, enabling massive CO₂ transport as bicarbonate
- Act as acid-base buffers - hemoglobin protein is the dominant blood buffer
4. White Blood Cells (Leukocytes)
Normal WBC count: ~7,000/µL (vs. 5 million RBCs/µL). WBCs are the mobile units of the immune system, transported rapidly to sites of infection and inflammation.
Classification
Granulocytes (have cytoplasmic granules; polymorphonuclear)
| Cell | % of WBCs | Key Features & Functions |
|---|---|---|
| Neutrophils | 47-67% | Multi-lobed nucleus; granules contain lysozymes, lactoferrin, antimicrobial peptides; primary phagocytes against bacteria; recruited via selectins + integrins (diapedesis) |
| Eosinophils | 1-4% | Bilobed nucleus; cytotoxic to parasites (helminths, protozoa); involved in allergic reactions |
| Basophils | <0.5% | Granules contain heparin, histamine, leukotrienes; role in allergic and inflammatory responses |
Agranulocytes (no specific granules)
| Cell | % of WBCs | Key Features & Functions |
|---|---|---|
| Lymphocytes | 26-30% | Dense spherical nucleus; T cells (cell-mediated immunity), B cells (antibody production), NK cells (kill virus-infected and cancer cells) |
| Monocytes | 3-9% | Kidney-shaped nucleus; migrate out of blood and differentiate into macrophages; antigen-presenting cells |
5. Platelets (Thrombocytes)
- Count: 150,000-450,000/µL (average ~300,000)
- Small, anucleate cytoplasmic fragments derived from megakaryocytes in bone marrow
- Organized into 4 zones: peripheral, structural, organelle, and membrane
- Function: Activation of hemostasis - adhere to damaged vessel walls, aggregate to form a primary platelet plug, and release granules that amplify clotting
Hemostasis - Overview
| Phase | What Happens |
|---|---|
| 1. Vascular spasm | Damaged vessel contracts immediately to reduce blood flow |
| 2. Primary hemostasis | Platelet adhesion (via vWF + GpIb), activation, and aggregation (via GpIIb/IIIa + fibrinogen) form a soft platelet plug |
| 3. Secondary hemostasis | Coagulation cascade activates - intrinsic pathway (contact with subendothelial collagen) and extrinsic pathway (tissue factor + Factor VIIa) converge at Factor X → thrombin → fibrin mesh stabilizes the clot |
| 4. Fibrinolysis | Plasmin dissolves the clot after healing; regulated by tPA and PAI-1 |
6. Hematopoiesis - How Blood Cells Are Made
All blood cells arise from hematopoietic stem cells (HSCs) residing in the red bone marrow in adults (previously in liver/spleen during fetal life). HSCs are pluripotent and self-renewing.
HSC
├─ Common Myeloid Progenitor (CMP)
│ ├─ Megakaryocyte → Platelets (thrombopoiesis)
│ ├─ Proerythroblast → RBCs (erythropoiesis)
│ └─ Granulocyte/Monocyte Progenitor (GMP)
│ ├─ Myeloblast → Neutrophils, Eosinophils, Basophils
│ └─ Monoblast → Monocytes → Macrophages
└─ Common Lymphoid Progenitor (CLP)
├─ T lymphocytes (mature in thymus)
├─ B lymphocytes (mature in bone marrow)
└─ NK cells
Neutrophil development stages: myeloblast → promyelocyte → myelocyte (first to show specific granules) → metamyelocyte → band cell → mature neutrophil. A "left shift" (increased band cells in blood) indicates acute bacterial infection.
Key regulators:
- Erythropoietin (EPO) - secreted by kidneys in response to hypoxia → drives erythropoiesis
- Thrombopoietin (TPO) - drives megakaryocyte/platelet production
- G-CSF, M-CSF, GM-CSF - colony-stimulating factors driving granulocyte/monocyte production
- IL-2, IL-7 - lymphocyte growth factors
Bone marrow: Red marrow (active hematopoiesis) is found in flat bones (sternum, ribs, pelvis, vertebrae) in adults. Yellow marrow (inactive, adipose-filled) replaces red marrow in long bone shafts. Under severe demand (e.g., hemolytic anemia), yellow marrow can be reactivated.
7. Key Blood Functions - Summary
| Function | Mediator |
|---|---|
| O₂ transport | Hemoglobin (RBCs) |
| CO₂ transport | Bicarbonate (from carbonic anhydrase in RBCs) |
| Immune defense | WBCs (neutrophils phagocytose; lymphocytes mount adaptive responses) |
| Hemostasis | Platelets + coagulation factors |
| Oncotic pressure | Albumin |
| pH buffering | Hemoglobin, bicarbonate, plasma proteins |
| Hormone/nutrient transport | Albumin, transferrin, lipoproteins, plasma |
| Temperature regulation | Heat transport from deep tissues to skin |
8. Common Blood Disorders - Quick Reference
| Disorder | Core Defect |
|---|---|
| Anemia | Reduced RBC count or Hgb (iron deficiency, B12/folate deficiency, hemolysis, bone marrow failure) |
| Polycythemia | Excess RBCs (primary: PV mutation in JAK2; secondary: chronic hypoxia, EPO-secreting tumor) |
| Leukemia | Malignant clonal proliferation of WBC precursors (AML, ALL, CML, CLL) |
| Thrombocytopenia | Low platelets → bleeding risk (ITP, TTP, heparin-induced HIT, bone marrow suppression) |
| Hemophilia A/B | Factor VIII/IX deficiency → impaired coagulation cascade |
| DIC | Uncontrolled activation of both clotting and fibrinolysis; consumption of factors and platelets |
| Sickle cell disease | HbS (β-globin Glu→Val mutation) → RBC sickling under low O₂ → vascular occlusion, hemolysis |
| Thalassemia | Reduced globin chain synthesis → hypochromic microcytic anemia |
Sources: Medical Physiology (Boron & Boulpaep) | Guyton and Hall Textbook of Medical Physiology | Histology: A Text and Atlas with Correlated Cell and Molecular Biology (Eroschenko)
This is a shared conversation. Sign in to Orris to start your own chat.