Neonatal sepsis for paediatrics examination mbbs Final year
Reading File
Finding Sources
Searching PubMed
"neonatal sepsis" diagnosis management
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Searching the Web
neonatal sepsis MBBS final year paediatrics definition classification organisms diagnosis treatment 2024
Loading Image
I now have all the key content needed. Let me compile a comprehensive, exam-oriented answer on neonatal sepsis for MBBS Final Year Paediatrics.
Neonatal Sepsis - MBBS Final Year Paediatrics
Definition
Neonatal sepsis (neonatal septicemia) is defined as a generalized systemic infection with clinical features of sepsis occurring in the first 28 days of life, associated with pure growth of bacteria from blood or other sterile sites in a newborn.
- Incidence (India, NNPD data): ~30 per 1000 live births; mortality ~4.1%
- Neonates have approximately twice the risk of serious bacterial infection compared to infants aged 4-8 weeks
- It is the most common cause of neonatal cardiorespiratory distress
Classification
| Feature | Early-Onset Sepsis (EOS) | Late-Onset Sepsis (LOS) |
|---|---|---|
| Timing | First 72 hours (some define as <7 days) | After 72 hours (>7 days in some definitions) |
| Source | Maternal genital tract / perinatal acquisition | Environment, hospital, caregivers |
| Presentation | Fulminant, multisystem | More gradual onset |
| Predominant organisms | GBS, E. coli, Listeria monocytogenes, Klebsiella, Haemophilus influenzae | Staphylococcus aureus (MRSA), CoNS, Klebsiella, Pseudomonas, Candida |
| Association | Maternal risk factors | Nosocomial / community |
| Complications | Septic shock, neutropenia more common | Meningitis more common |
Very Late-Onset Sepsis - Some classify infections after 90 days separately, mainly in preterm NICU babies.
Causative Organisms
Early-Onset Sepsis (India - important for exam)
- Gram-negative organisms predominate in India (unlike the West where GBS predominates)
- Klebsiella pneumoniae, E. coli - most common in India
- Group B Streptococcus (GBS, Streptococcus agalactiae) - most common in the West
- Listeria monocytogenes
- Staphylococcus aureus
Late-Onset Sepsis
- Staphylococcus aureus (MRSA in NICU)
- Coagulase-negative Staphylococci (CoNS) - esp. in preterm/VLBW with lines
- Klebsiella, Pseudomonas, Acinetobacter
- Candida species - in immunocompromised/preterm
Memory Tip: GBS is most common globally; Klebsiella/E. coli dominate in India.
Risk Factors
Maternal / Perinatal Risk Factors (EOS)
- Prolonged rupture of membranes (PROM >18 hours)
- Maternal fever / chorioamnionitis
- GBS-positive vaginal swabs in mother
- Fetal distress / birth asphyxia
- Prematurity / low birth weight (LBW)
- Maternal urinary tract infection
- Traumatic delivery / multiple vaginal examinations
Neonatal Risk Factors (LOS)
- Prematurity / VLBW (<1500 g)
- Invasive procedures (central lines, intubation)
- Prolonged hospital stay / NICU admission
- Parenteral nutrition
- Immunodeficiency
Pathophysiology
Neonates are immunologically vulnerable due to:
- Immature cutaneous and mucosal barriers
- Low T-cell and B-cell concentrations with absent antigenic memory
- Maternal IgG (passive immunity) reaches nadir at 2-3 months of age
- Depressed cell-mediated immunity (susceptibility to viral/fungal infections)
- Neutrophil functional defects (chemotaxis, phagocytosis)
Clinical Features
General (The "sick-looking" neonate)
The classic presentation is a neonate who "looks unwell" without localizing signs.
| System | Features |
|---|---|
| Temperature | Fever (rectal ≥38°C/100.4°F) OR hypothermia (<36.5°C/97.7°F) - hypothermia more common in preterm |
| CNS | Lethargy, irritability, high-pitched cry, seizures, bulging fontanelle |
| Respiratory | Apnea, tachypnea, grunting, respiratory distress (may be the only sign) |
| GI | Poor feeding, vomiting, abdominal distension, diarrhea |
| Cardiovascular | Hypotension, poor perfusion, tachycardia/bradycardia |
| Skin | Jaundice (especially in first 24 hours), petechiae, rashes, mottling, sclerema |
| Metabolic | Hypoglycemia, metabolic acidosis |
Important exam point: Nuchal rigidity and Kernig/Brudzinski signs are present in only a small minority of neonates with meningitis - DO NOT rely on them to exclude meningitis in neonates!
Tachypnea and respiratory distress can be the only sign of meningitis or UTI in a neonate.
Investigations
Sepsis Screen (essential for exam)
The "Sepsis Screen" - a battery of tests where 2 or more positive tests = positive screen:
| Test | Positive Value |
|---|---|
| Total leukocyte count (TLC) | <5000/mm³ or >15,000/mm³ (leucopenia more significant) |
| Absolute neutrophil count (ANC) | <1800/mm³ |
| Immature to total neutrophil ratio (I:T ratio) | >0.2 |
| Micro-ESR | >15 mm at end of 1 hour (in first week) |
| C-Reactive Protein (CRP) | >1 mg/dL (>10 mg/L) |
Gold Standard Investigation
- Blood culture - gold standard for diagnosis; however only ~50% of clinically septic neonates have positive cultures
Other Investigations
- CBC with differential - neutropenia, thrombocytopenia, toxic granules, Döhle bodies
- Lumbar puncture + CSF analysis - mandatory in all suspected neonatal sepsis (threshold is lower than older infants); send for cell count, protein, glucose, culture
- Urine culture (catheter or suprapubic aspiration)
- Chest X-ray - pneumonia
- Blood glucose - hypoglycemia
- ABG - metabolic acidosis, hypoxia
- Coagulation profile - DIC (gram-negative sepsis more likely to cause thrombocytopenia)
- Procalcitonin - rising biomarker, but physiologically elevated in first 48 hours of life normally
- Serum bilirubin
Differential Diagnosis
- Congenital heart disease (ductal-dependent lesions - may mimic septic shock)
- TORCH infections (Toxoplasmosis, Rubella, CMV, Herpes, Others)
- Respiratory distress syndrome (RDS) / TTN
- Inborn errors of metabolism
- Congenital adrenal hyperplasia
- Intracranial hemorrhage
- Necrotizing enterocolitis (NEC)
Management
Supportive Care (ABCDE approach)
- Maintain thermoneutral environment
- IV access, fluid resuscitation (10 mL/kg normal saline boluses for shock)
- Oxygen supplementation / mechanical ventilation if required
- Treat hypoglycemia (IV dextrose)
- Correct metabolic acidosis
- Blood products for DIC / thrombocytopenia
Empirical Antibiotic Therapy (start BEFORE culture results)
First-line (Standard EOS/LOS):
| Drug | Dose | Coverage |
|---|---|---|
| Ampicillin | 50 mg/kg IV | GBS, Listeria, Enterococcus |
| + Gentamicin (aminoglycoside) | 2.5 mg/kg IV | E. coli, gram-negatives |
AVOID ceftriaxone in neonates - displaces bilirubin from albumin and can cause kernicterus!
When gram-negative meningitis suspected (better CNS penetration needed):
- Replace gentamicin with Cefotaxime or Ceftazidime (50 mg/kg) - better CSF penetration
When MRSA/CoNS (NICU/LOS) suspected:
- Add Vancomycin
When HSV encephalitis suspected (maternal herpes history, CSF with lymphocytes + RBCs, ill-appearing neonate):
- Add IV Acyclovir
When fungal sepsis suspected (preterm, VLBW, prior antibiotics):
- Amphotericin B or Fluconazole
Duration of Antibiotics
- Culture-positive sepsis without meningitis: 10-14 days
- Meningitis: 14-21 days
- Culture-negative but clinically improved: 7-10 days
Prevention
Intrapartum Antibiotic Prophylaxis (IAP) for GBS
- Penicillin G / Ampicillin / Cefazolin given ≥4 hours before delivery = adequate IAP
- Indications: GBS-positive vaginal swab, prior GBS-affected infant, GBS bacteriuria in current pregnancy, unknown status with risk factors
Other Prevention Strategies
- Handwashing (most important infection control measure in NICU)
- Minimize invasive procedures
- Encourage exclusive breastfeeding
- Kangaroo mother care for LBW/preterm
- Chlorhexidine cord care
- Antenatal corticosteroids reduce risk in preterm
Risk Assessment for GBS EOS (AAP Algorithm)
Three approaches are used (see figure below):
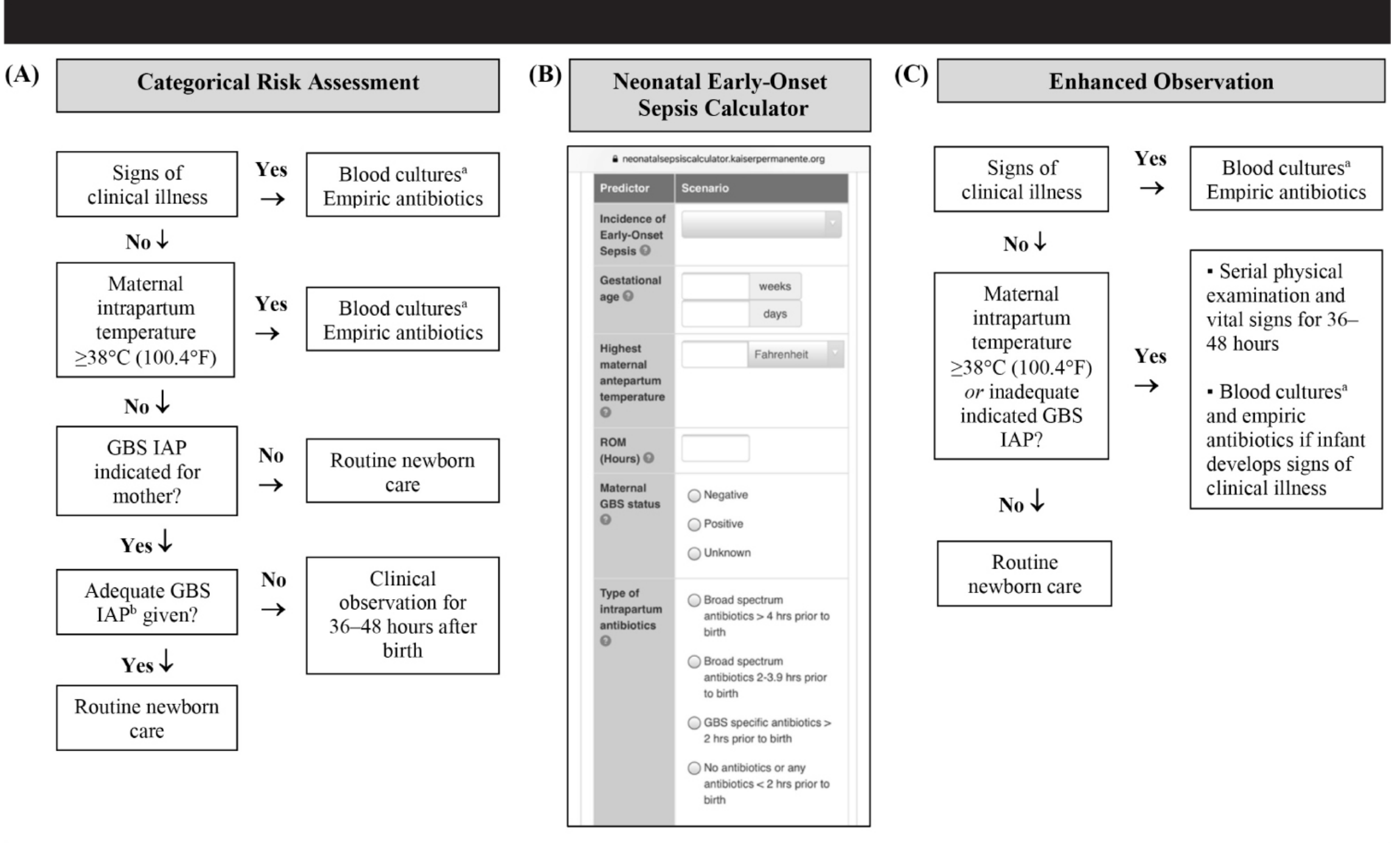
(A) Categorical: Uses threshold values - if signs of illness or maternal fever ≥38°C, give blood culture + empiric antibiotics. If GBS IAP was adequate - routine care.
(B) Neonatal EOS Calculator (Kaiser Permanente): Multivariate tool using gestational age, maternal temperature, ROM duration, GBS status, IAP type - estimates risk per 1000 births.
(C) Enhanced Observation: Based on clinical condition at birth - well-appearing term infants have 60-70% reduced risk.
Red Book (AAP) 2021, p. 1101-1102
Complications
- Meningitis - especially with late-onset sepsis; commoner with GBS and gram-negative organisms
- Disseminated Intravascular Coagulation (DIC)
- Septic shock - more common with early-onset sepsis
- Pneumonia / respiratory failure
- Pulmonary hypertension
- Renal failure
- Neurodevelopmental sequelae - cerebral palsy, hearing loss, developmental delay (especially post-meningitis)
- Death - still a major cause of neonatal mortality
High-Yield Exam Points
- Gold standard: Blood culture (positive in only ~50% of clinical sepsis)
- Avoid ceftriaxone in neonates - risk of kernicterus
- Empiric treatment: Ampicillin + Gentamicin (first line)
- Hypothermia (not just fever) is a danger sign in preterm neonates
- GBS = most common cause globally (West); Klebsiella/E. coli = most common in India
- Meningitis signs are unreliable in neonates - always do LP
- LOS is more associated with meningitis; EOS with septic shock
- Sepsis screen = 2 or more positive parameters
- Neonates with suspected sepsis should always be admitted and started on empiric IV antibiotics
- Add Acyclovir for HSV encephalitis risk; Add Vancomycin for MRSA risk in NICU
Sources: Tintinalli's Emergency Medicine, p. 774-775 | Miller's Anesthesia 10e, p. 11455-11456 | Red Book (AAP) 2021, p. 1100-1103 | Antibiotic strategies for neonatal sepsis 2025 meta-analysis (PMID: 40555905)
This is a shared conversation. Sign in to Orris to start your own chat.