Seroma of leg
Reading File
Finding Sources
Finding Sources
Searching PubMed
seroma lower extremity management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Finding Sources
I now have comprehensive information to deliver a thorough answer. Let me compile it.
Seroma of the Leg
Definition
A seroma is a sterile collection of serous (inflammatory/lymphatic) fluid that accumulates in a potential tissue space created by surgical dissection, trauma, or injury. In the leg, it most commonly arises as a complication of:
- Inguinal lymph node dissection (e.g., for melanoma) - one of the most common causes
- Lower extremity vascular/bypass surgery
- Flap creation or large subcutaneous dissections over the thigh or leg
- Trauma with shearing of soft tissues (degloving-type injuries)
Pathophysiology
Release of fascial planes or creation of large tissue flaps creates a potential dead space that fills with exudate - a combination of lymph, plasma ultrafiltrate, and inflammatory mediators - that exceeds the capacity for local reabsorption. Wide subcutaneous dissection and premature drain dislodgement/clogging are key contributors. - Sabiston Textbook of Surgery
Presentation
- Soft, fluctuant, non-tender swelling beneath the skin
- May develop slowly over days to weeks post-operatively or post-trauma
- Skin overlying the swelling is typically normal (no erythema or warmth unless infected)
- Can cause discomfort, wound tension, or drainage through the incision
Diagnosis
- Clinical in most cases (fluctuant, non-tender swelling at or near a surgical site)
- Bedside ultrasound - first-line imaging; confirms anechoic fluid collection, distinguishes seroma from hematoma, abscess, or recurrent hernia
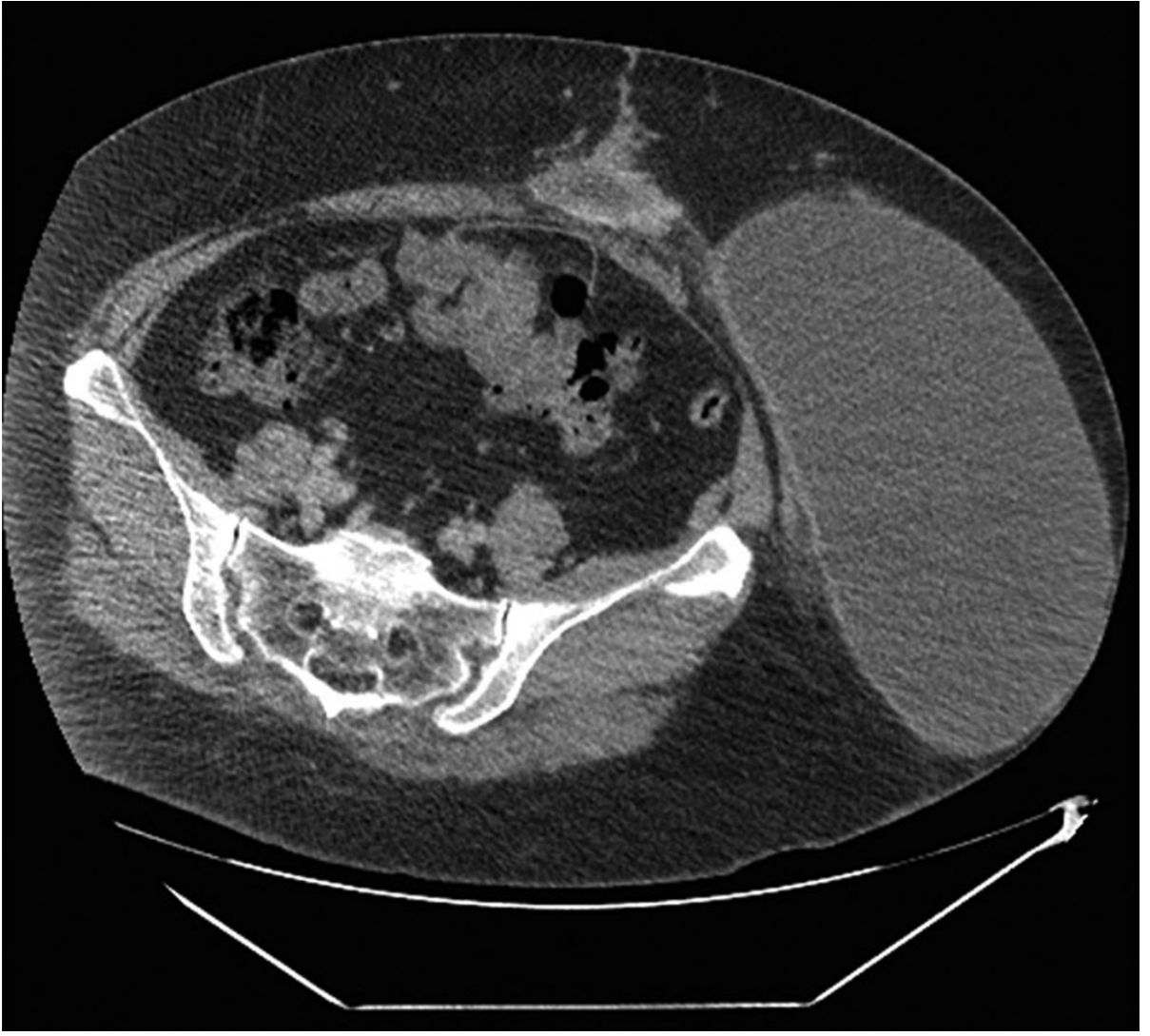
- CT scan - used when there is ambiguity (e.g., differentiating seroma from early hernia recurrence, or when deep location makes US difficult)
Specific Context: Inguinal Lymph Node Dissection for Leg Melanoma
This is a very common scenario. Inguinal dissection carries substantial morbidity including:
- Seroma
- Infection
- Lymphedema
- Flap necrosis
- Deep venous thromboembolism
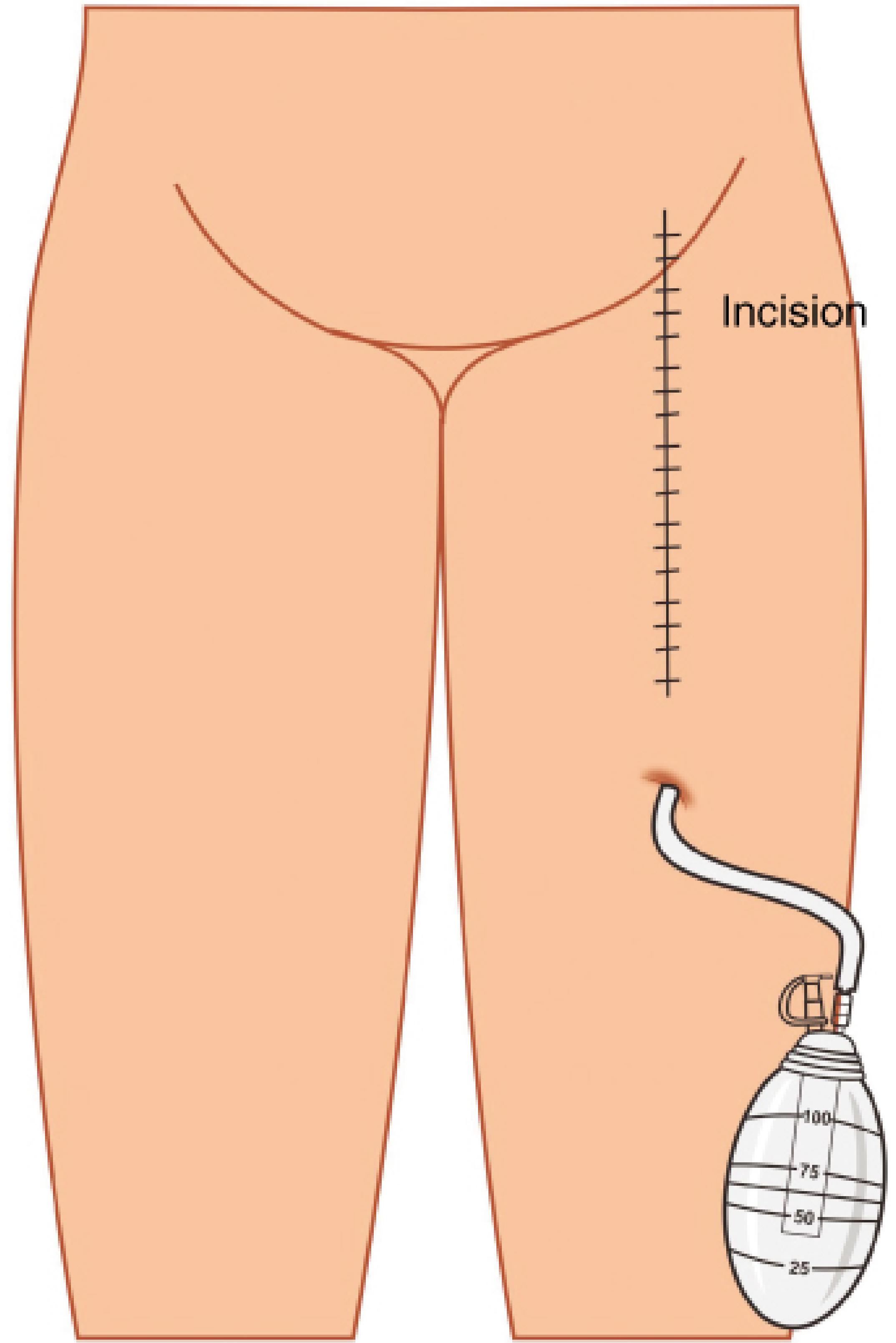
Prevention: A closed suction drain is placed just distal to the distal end of the incision (see illustration below). The drain is left in place until output is <75 mL/day.
Additional preventive techniques include:
- Limiting incision length
- Tension-free skin closure
- Creating a thick (1 cm) skin flap
- Sartorius muscle transposition to cover femoral vessels
Risk Factors for Seroma Formation
| Factor | Notes |
|---|---|
| Wide subcutaneous dissection | Creates large dead space |
| Large skin flaps | Elevated lymph/plasma exudate |
| High BMI | Greater subcutaneous tissue bulk |
| Premature drain removal | Dead space not yet obliterated |
| Emergency surgery | Less meticulous hemostasis |
| Biologic or onlay mesh | When applicable |
| Component separation | Extensive fascial release |
Management
Management depends on size, symptoms, and chronicity:
1. Observation
- Small, asymptomatic seromas will typically resolve spontaneously
- No prophylactic antibiotics are indicated for uncomplicated seromas
- Tintinalli's Emergency Medicine: "Small seromas can be managed by observation and will usually resolve spontaneously."
2. Needle Aspiration
- Indicated when the seroma is large, prolonged, or causing significant symptoms (pain, pressure, drainage from wound)
- Can be performed as an outpatient procedure (bedside or ultrasound-guided)
- May require multiple aspirations for complete resolution
- After inguinal dissection: observe if small; aspirate if large or symptomatic - Fischer's Mastery of Surgery
3. Drain Placement
- May be required for seromas that persist after repeated aspirations
- Drains removed when output <25-30 mL over 24 hours
4. Sclerotherapy (refractory cases)
Chemical sclerotherapy agents used when aspiration/catheter drainage fails:
- Talc
- Tetracycline / Doxycycline
- Ethanol
- Erythromycin
- Fibrin glue
Mechanical sclerotherapy via endoscopic argon beam ablation has also been described. - Sabiston Textbook of Surgery
5. Surgical Excision
- Reserved for seromas that are refractory to all percutaneous interventions
CT Image: Seroma After Skin Flap Creation
Complications of Untreated / Infected Seroma
- Secondary infection - may progress to abscess (typically presents 10-14 days post-op)
- Compromise of mesh integration (in hernia repair contexts)
- Wound dehiscence
- If infection is suspected: open, drain, and pack with wet-to-dry dressings
Prevention Summary
| Technique | Evidence |
|---|---|
| Closed suction drains | Reduces seroma rate (OR 0.34; 95% CI 0.12-0.96) with no increase in infection - meta-analysis |
| External compression (binders) | Aids skin flap adherence, hinders fluid collection |
| Quilting sutures | Obliterate dead space under flaps |
| Surgical tissue adhesive | Applied under skin flaps; limited large study evidence |
| Tension-free closure, thick flaps | Reduces ischemia and necrosis |
Sources: Fischer's Mastery of Surgery (8th ed.), Sabiston Textbook of Surgery, Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.