Explain the bronchial asthma In Practice of medicine
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from Harrison's 22E and Goldman-Cecil. I have enough to write a thorough, well-structured explanation. Let me compose the full answer.
Bronchial Asthma - Practice of Medicine
Definition
Asthma is a disease characterized by episodic airway obstruction and airway hyperresponsiveness, usually accompanied by airway inflammation. In most cases the obstruction is reversible, but in a subset of patients a component may become fixed/irreversible. It is a clinical syndrome of largely unknown ultimate etiology, with multiple underlying pathobiologic mechanisms (endotypes) driving the classic signs and symptoms.
- Harrison's Principles of Internal Medicine, 22E, Ch. 298
- Goldman-Cecil Medicine, Ch. 75
Epidemiology
- Affects approximately 262 million people globally (Harrison's) / 340 million (Cecil)
- 7.9% of the US population is asthmatic; ~4.3% worldwide prevalence
- More prevalent in children (8.4%) than adults (7.7%); boys > girls in childhood, then women > men after puberty (female:male ratio ~1.8:1 in adults)
- Prevalence increased >50% in the latter half of the 20th century, linked to industrialization and reduced farming/animal contact (the "hygiene hypothesis")
- In the United States, asthma is more prevalent and causes greater morbidity in Black patients and the Puerto Rican population
- Global mortality declined from 0.44/100,000 in 1993 to 0.19/100,000 in 2006 - largely attributed to increased use of inhaled corticosteroids
- Annual economic cost in the US: estimated at $82 billion (2013 data)
Asthma Development Pathway
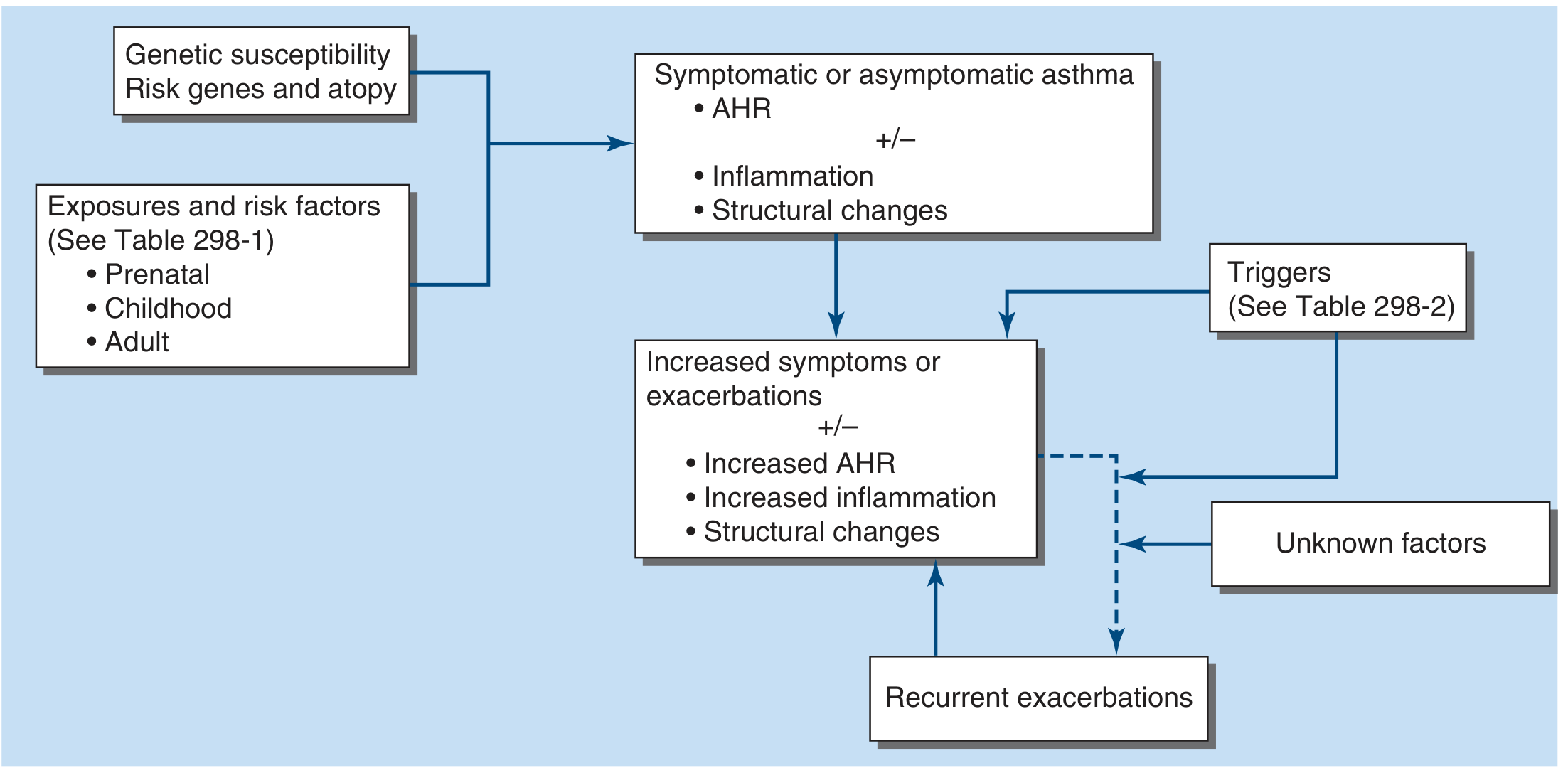
Genetic susceptibility, environmental exposures, and developmental factors interact to produce airway hyperresponsiveness (AHR), inflammation, and structural changes. Triggers then drive acute exacerbations - Harrison's 22E, Fig. 298-1.
Pathobiology
Genetics
Asthma has approximately 60% heritability (twin studies). Multiple genome-wide association studies have identified loci predominantly related to immune mechanisms - particularly genes controlling IgE production, cytokine signaling, and epithelial barrier function. (Goldman-Cecil, Ch. 75)
Endotypes / Pathologic Subtypes
The syndrome is characterized by marked heterogeneity. Multiple endotypes underlie the classic presentation:
| Subtype | Features |
|---|---|
| Atopic/allergic | Most common; IgE-mediated sensitization to environmental allergens; prevalent in school-age children and ~50% of adults |
| Non-atopic | No detectable IgE sensitization; more common in adult-onset asthma; often triggered by infections, exercise, irritants |
| Aspirin-exacerbated | Characterized by nasal polyposis, chronic rhinosinusitis, and severe bronchospasm triggered by NSAIDs; significant leukotriene overproduction |
| Eosinophilic | High blood/sputum eosinophils; type 2 inflammation (IL-4, IL-5, IL-13); responds well to anti-IL-5/IL-4R biologics |
| Non-eosinophilic / neutrophilic | Steroid-resistant; associated with smoking, obesity, occupational exposures |
| Occupational | Triggered by workplace sensitizers or irritants |
Cellular Mechanisms
In allergic asthma, allergen exposure leads to:
- IgE production by B cells, facilitated by Th2 cytokines (IL-4, IL-13)
- Mast cell sensitization - on re-exposure, cross-linking of IgE on mast cells triggers degranulation, releasing histamine, prostaglandins, leukotrienes, and tryptase
- Eosinophil recruitment driven by IL-5
- Airway remodeling - subepithelial fibrosis, smooth muscle hypertrophy, goblet cell hyperplasia, and vascular changes over time
Key inflammatory mediators include: histamine, cysteinyl leukotrienes (LTC4, LTD4), prostaglandins, tryptase, IL-4, IL-5, IL-13, TNF-alpha, and TSLP.
Structural Changes (Airway Remodeling)
Chronic asthma produces progressive structural changes:
- Subepithelial fibrosis (thickened reticular basement membrane)
- Smooth muscle hypertrophy and hyperplasia
- Goblet cell hyperplasia with mucus hypersecretion
- Vascular proliferation
- These changes contribute to the partially irreversible component of obstruction seen in long-standing disease
Triggers
Common triggers of asthma exacerbations include:
- Allergens: dust mites, cockroach, cat/dog dander, mold, seasonal pollens
- Respiratory infections: rhinovirus (most common), RSV, influenza, parainfluenza, Chlamydophila pneumoniae, Mycoplasma pneumoniae
- Exercise (especially in cold, dry air)
- NSAIDs/aspirin (in aspirin-exacerbated respiratory disease)
- Occupational exposures: isocyanates, flour, latex, animal dander
- Irritants: tobacco smoke, air pollutants, strong odors, fumes
- Hormonal changes: menses, pregnancy
- GERD and post-nasal drip
- Emotional stress and anxiety
- Beta-blockers (including ophthalmic drops)
Clinical Manifestations
Asthma most commonly presents as:
- Episodic wheezing (expiratory > inspiratory)
- Shortness of breath (dyspnea)
- Chest tightness
- Cough (may be the only symptom in "cough-variant asthma")
- Mucus production
Symptoms often:
- Occur at night or early morning (circadian variation in airway tone)
- Are triggered by the above stimuli
- Resolve spontaneously or with bronchodilator therapy
- Are worse in cold air or with exercise
In acute severe attacks: the patient is upright, using accessory muscles, unable to complete sentences, with audible wheeze, prolonged expiration, tachycardia, tachypnea, pulsus paradoxus, and falling O2 saturation. A "silent chest" in an acutely dyspneic patient is ominous - airflow so reduced that wheeze disappears.
Differential Diagnosis
| Condition | Distinguishing Feature |
|---|---|
| COPD | Usually older, smoker, less reversibility on spirometry |
| Cardiac asthma (heart failure) | Orthopnea, S3, elevated BNP, bilateral crackles |
| Vocal cord dysfunction | Inspiratory stridor, normal spirometry between episodes |
| Endobronchial obstruction | Localized wheeze, does not respond to bronchodilators |
| Pulmonary embolism | Acute, pleuritic chest pain, risk factors |
| Hyperventilation / anxiety | No wheeze, normal spirometry, Co2 dysregulation |
Diagnosis and Evaluation
Clinical Approach
- Compatible history of recurrent wheezing, breathlessness, chest tightness, or cough - especially when episodic and triggered
- Pulmonary function testing (spirometry) is the cornerstone of objective confirmation
Key Investigations
1. Spirometry
- Shows an obstructive pattern: reduced FEV1, reduced FEV1/FVC ratio (<0.70)
- Post-bronchodilator reversibility: ≥12% AND ≥200 mL increase in FEV1 confirms diagnosis
- Normal spirometry does not exclude asthma (can be normal between attacks)
2. Peak Expiratory Flow Rate (PEFR)
- Inexpensive, portable; serial measurements show diurnal variability >20% suggesting asthma
- Used for home monitoring
3. Bronchoprovocation Challenge
- Methacholine, histamine, or exercise challenge
- Used when spirometry is normal but clinical suspicion is high
- A PC20 methacholine <8 mg/mL is considered positive for airway hyperresponsiveness
4. Exhaled Nitric Oxide (FeNO)
- Elevated in eosinophilic airway inflammation (>25 ppb in adults)
- Guides choice of ICS dose and predicts steroid response
5. Allergy Testing
- Skin prick test or specific IgE (RAST/ImmunoCAP) to identify allergen triggers
- Essential if biologic therapy (omalizumab) is being considered
6. Additional in Severe/Poorly Responsive Asthma
- Complete blood count with differential (peripheral eosinophilia)
- Serum IgE
- Sputum induction (eosinophil count)
- HRCT chest (to exclude structural lung disease, bronchiectasis)
- Testing for aspirin sensitivity, ABPA (Aspergillus IgE, precipitins)
Classification of Severity (NAEPP/GINA)
| Category | Daytime Sx | Nighttime Sx | SABA use | FEV1 % predicted |
|---|---|---|---|---|
| Intermittent | ≤2 days/week | ≤2/month | ≤2 days/week | ≥80% |
| Mild Persistent | >2 days/week | 3-4/month | >2 days/week | ≥80% |
| Moderate Persistent | Daily | >1/week | Daily | 60-80% |
| Severe Persistent | Continuous | Frequent | Multiple/day | <60% |
Treatment
Treatment has two components: controller (preventive) therapy and rescue (reliever) therapy. The stepwise approach adjusts intensity to the level of asthma control.
Goals of Therapy (Goldman-Cecil, Ch. 75)
- Allow pursuit of normal daily activities without limitation from asthma
- Allow uninterrupted sleep
- Minimize need for rescue inhaler use
- Prevent unscheduled medical visits
- Maintain near-normal lung function
Stepwise Treatment (GINA/NAEPP Steps 1-5)
Step 1 - Mild Intermittent
- Rescue: Short-acting β₂-agonist (SABA) as needed - salbutamol (albuterol), terbutaline
- Preferred (GINA 2023): Low-dose ICS-formoterol as-needed (AIR therapy)
Step 2 - Mild Persistent
- Controller: Low-dose ICS (e.g., fluticasone 100 mcg/day, beclomethasone 200 mcg/day)
- Alternative: Leukotriene receptor antagonist (LTRA) - montelukast
- Rescue: SABA or low-dose ICS-formoterol
Step 3 - Moderate Persistent
- Controller: Low-to-medium dose ICS + LABA (e.g., fluticasone/salmeterol, budesonide/formoterol)
- Alternative: Medium-dose ICS alone, or low-dose ICS + LTRA
Step 4 - Severe Persistent
- Controller: Medium-to-high dose ICS/LABA
- Add-on: Tiotropium (LAMA), LTRA, zileuton
- Consider biologic therapy if poorly controlled
Step 5 - Very Severe / Refractory
- High-dose ICS/LABA
- Biologics:
- Omalizumab (anti-IgE) - for allergic asthma, IgE 30-700 IU/mL, positive allergen sensitivity
- Mepolizumab, Reslizumab, Benralizumab (anti-IL-5/IL-5R) - for severe eosinophilic asthma
- Dupilumab (anti-IL-4Rα) - for type 2 asthma (eosinophilic + atopic dermatitis)
- Tezepelumab (anti-TSLP) - for severe uncontrolled asthma regardless of phenotype
- Oral corticosteroids as last resort (minimum effective dose)
Key Medications in Detail
Inhaled Corticosteroids (ICS)
- Mainstay of persistent asthma control
- Reduce airway inflammation, improve lung function, decrease exacerbation frequency
- Reduction in asthma mortality attributed to widespread ICS use
- Side effects: thrush, dysphonia; at high doses - osteoporosis, cataract, growth suppression in children
- Do NOT alter the long-term natural history of asthma
Short-Acting β₂-Agonists (SABA)
- First-line rescue: salbutamol, terbutaline
- Onset within minutes; bronchodilation via smooth muscle relaxation (cAMP pathway)
- Overuse (>2 canister/month) is a risk factor for asthma death - mandates controller escalation
Long-Acting β₂-Agonists (LABA)
- Salmeterol, formoterol - never used as monotherapy in asthma; always combined with ICS
- Formoterol: fast onset, can also serve as reliever
Leukotriene Modifiers
- Montelukast (LTRA): oral, once daily; effective add-on or mild asthma alternative to ICS; preferred in exercise-induced asthma and aspirin-exacerbated disease
- Zileuton (5-lipoxygenase inhibitor): oral; increases liver transaminases in 3% of patients
Anti-IgE (Omalizumab)
- Targets Fc portion of IgE; prevents mast cell/basophil sensitization
- Reduces exacerbations by 25-50% in eligible allergic asthmatics
- Dosed subcutaneously every 2-4 weeks based on weight and IgE level
Cromolyn Sodium
- Stabilizes mast cells; mild efficacy; primarily used in pediatrics via nebulization
Methylxanthines (Theophylline)
- Narrow therapeutic window; now rarely used as add-on in step 3-4; requires serum level monitoring
Acute Asthma Attack - Management
Assessment of Severity
- Mild/Moderate: PEFR >50% predicted, O2 sat >92%, speaks in phrases
- Severe: PEFR 33-50%, O2 sat 90-92%, speaks in words, tachycardia >110, RR >25
- Life-threatening: PEFR <33%, silent chest, cyanosis, bradycardia, exhaustion, altered consciousness
Management Steps
- Oxygen: target SpO2 93-95% (94-98% in children)
- Inhaled SABA: repeated doses every 20 minutes for the first hour (salbutamol 2.5-5 mg via nebulizer or 4-8 puffs via MDI+spacer)
- Ipratropium bromide: add to SABA nebulization in moderate-severe attacks (0.5 mg q20 min x 3 doses)
- Systemic corticosteroids: oral prednisolone 40-60 mg or IV methylprednisolone; begin as early as possible; continue 5-7 days
- IV magnesium sulfate: 2g IV over 20 minutes - for severe/life-threatening attacks or those not responding to above
- Heliox (helium-oxygen mixture): can reduce work of breathing; adjunct use
- IV aminophylline/theophylline: rarely used now; high toxicity
- ICU / Intubation: for respiratory failure, fatigue, rising PaCO2
Patients at Risk of Death from Asthma
- Previous near-fatal attack (ICU/intubation)
- Two or more hospitalizations or >3 ED visits in past year
- Over-reliance on SABA (>1 canister/month)
- Lack of ICS use
- Psychosocial problems, poor adherence
- Comorbidities: cardiovascular disease, COPD, psychiatric illness
- Low FEV1, poor perception of symptoms
Special Considerations
Aspirin-Exacerbated Respiratory Disease (AERD)
- Samter's triad: asthma + nasal polyposis + aspirin/NSAID sensitivity
- Significant leukotriene overproduction - leukotriene modifiers are particularly effective
- Aspirin desensitization can be performed under supervision
Exercise-Induced Bronchoconstriction (EIB)
- Occurs 5-10 minutes after cessation of vigorous exercise
- Pre-treatment with SABA (10-15 minutes before) or montelukast is effective
- Warm-up and cool-down periods help blunt the response
Occupational Asthma
- Work-related sensitizer (isocyanates, flour, latex) or irritant (high-level exposure)
- Removal from exposure is the primary treatment; steroid therapy alone is insufficient
- Diagnosis: serial PEFR at/away from work, specific bronchoprovocation challenge
Asthma-COPD Overlap (ACO)
- Patients with features of both diseases: usually older smokers with partially reversible obstruction
- Require ICS-containing regimens; LABAs and LAMAs often needed
- High SABA-alone use increases risk
Asthma in Pregnancy
- Can worsen, improve, or remain unchanged during pregnancy
- Uncontrolled asthma carries greater risk to fetus than the risks of treatment
- ICS (budesonide preferred), SABAs, and montelukast are safe; systemic steroids when needed
- Close monitoring of PEFR and fetal wellbeing essential
Elderly Patients
- Diagnosis often delayed due to attribution of dyspnea to aging or cardiac disease
- Fixed airflow obstruction more common
- Inhaler technique issues more prevalent; risk of drug interactions (beta-blockers)
Severe / Refractory Asthma
- Defined as asthma requiring high-dose ICS/LABA to remain controlled, or uncontrolled despite Step 4-5 therapy
- Must first exclude poor adherence, inhaler technique errors, and comorbidities (GERD, rhinosinusitis, obesity, OSA, VCD)
- Phenotyping (FeNO, blood eosinophils, IgE, serology) guides biologic choice
- Bronchial thermoplasty: bronchoscopic procedure reducing airway smooth muscle mass; option for select refractory patients
Prognosis and Monitoring
- Many patients, especially children with mild-intermittent asthma, may enter remission in adulthood
- Patients with severe asthma, fixed obstruction, or smoking have worse long-term outcomes
- Regular monitoring tools: spirometry, FeNO, Asthma Control Test (ACT), Asthma Control Questionnaire (ACQ), symptom diary, PEFR charts
- A written Asthma Action Plan (green/yellow/red zones) given to every patient reduces exacerbations and emergency visits
Sources:
- Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapter 298 - Asthma (Elliot Israel)
- Goldman-Cecil Medicine, International Edition, Chapter 75 - Asthma (Jeffrey M. Drazen & Elisabeth H. Bel)
- Murray & Nadel's Textbook of Respiratory Medicine (supplementary)
This is a shared conversation. Sign in to Orris to start your own chat.