Malaria
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"malaria" AND "diagnosis"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have all the content needed for a thorough answer on clinical features and diagnosis of malaria. Let me compile it.
Malaria: Clinical Features & Diagnosis
Causative Species
Five Plasmodium species infect humans:
| Species | Fever Pattern | Notes |
|---|---|---|
| P. falciparum | Tertian (every 48 h), irregular early | Most dangerous; drug resistance common |
| P. vivax | Tertian (every 48 h) | Relapsing; dormant hypnozoites in liver |
| P. ovale | Tertian (every 48 h) | Relapsing; mild |
| P. malariae | Quartan (every 72 h) | Mild; can persist for years |
| P. knowlesi | Daily (every 24 h) | Zoonotic (SE Asia); more virulent than it appears - mimics P. malariae morphologically |
Vector: bite of the female Anopheles mosquito. Humans are the only natural reservoir.
Life Cycle (Pathogenic Basis of Symptoms)

Fig. 10.8 - Life cycle of P. falciparum, Robbins & Kumar Basic Pathology
- Hepatic (pre-erythrocytic) stage - clinically silent; sporozoites travel to the liver, differentiate into merozoites over 1-4 weeks; P. vivax and P. ovale can form dormant hypnozoites that cause relapse months to years later.
- Erythrocytic stage - merozoites invade RBCs via a lectin-like molecule binding sialidated glycophorin; trophozoites consume hemoglobin; schizonts multiply and lyse the RBC - this lysis cycle is what drives the periodic fever.
- P. falciparum trophozoites express PfEMP1 (knob-like extensions on infected RBCs) that bind ICAM-1, VCAM-1, and CD36 on vascular endothelium, causing sequestration in capillary beds - the mechanism of cerebral malaria and multi-organ failure.
Clinical Features
Typical (uncomplicated) presentation
- Paroxysms of fever - classically in three stages: cold/shivering stage → hot stage (high fever 39-41°C) → sweating stage; coincide with synchronized RBC lysis
- Fever periodicity: every 24 h (P. knowlesi), every 48 h (P. falciparum, P. vivax, P. ovale), every 72 h (P. malariae) - but this periodicity is unreliable, especially for P. falciparum which may produce continuous fever early in illness
- Headache, myalgia, arthralgia, fatigue - often the presenting complaints
- Nausea, vomiting, diarrhea - can mimic gastroenteritis and delay diagnosis
- Hemolytic anemia - pallor, jaundice; present to some degree in all species; severe in P. falciparum
- Splenomegaly - from marked hyperplasia of mononuclear phagocytes; hepatomegaly less common
- Thrombocytopenia - common finding on CBC
- Incubation period: typically 1-4 weeks after exposure
Key point: Fever is common but not universal at initial presentation. Studies in low-endemicity areas found fever or headache has sensitivity >95%. In travelers, diarrhea and headache may dominate before fever is prominent. - Rosen's Emergency Medicine
Severe / Complicated Malaria (P. falciparum)
Severe malaria is almost exclusively due to P. falciparum and can develop within days in non-immune patients:
| Complication | Features |
|---|---|
| Cerebral malaria | Convulsions, altered consciousness → coma; small vessels of the brain become engorged/occluded by PfEMP1-expressing RBCs |
| Severe anemia | Hemoglobin < 7 g/dL from hemolysis + inhibited erythropoietin + iron deficiency |
| Blackwater fever | Massive intravascular hemolysis → hemoglobinemia, hemoglobinuria ("black water"), jaundice, renal failure |
| Acute kidney injury | Often accompanies severe anemia and hemolysis |
| Pulmonary involvement | Ranges from cough to ARDS/ALI; bilateral opacities on CXR resembling pulmonary edema; alveolar macrophages may contain hemozoin (brown hemoglobin degradation product) |
| Hypoglycemia | High-grade parasitemia consumes glucose + quinine infusion stimulates insulin secretion |
| Multi-organ failure | End-stage severe disease |
High-risk groups for severe/pulmonary disease: children, pregnant women, and non-immune travelers.
Diagnosis
1. Peripheral Blood Smear (Gold Standard)
- Thick smear - used for detection (concentrated film; better sensitivity)
- Thin smear - used for species identification (morphology of intraerythrocytic forms)
- Stained with Giemsa or Wright stain
- Allows determination of parasitemia level (% infected RBCs) and species
- P. falciparum: "appliqué" or accolé forms (rings at periphery of RBC), multiply-infected RBCs, no enlarged RBCs
- Even if smear is negative, treatment should not be withheld if clinical suspicion is high - Rosen's Emergency Medicine
- Repeat smears every 12-24 h if initial smear is negative and clinical suspicion persists
2. Rapid Diagnostic Tests (RDTs)
- Antigen-based lateral flow assays (e.g., Alere BinaxNOW) - FDA approved; qualitative; ~$5/test
- Detect antigens: HRP-2 (P. falciparum specific), pLDH (all species), aldolase (pan-Plasmodium)
- Advantages: rapid (~15 min), no microscopy expertise needed
- Limitation: less sensitive than microscopy; cannot quantify parasitemia; microscopy must still be performed for all positive RDT results to confirm species and severity
3. PCR (Molecular Methods)
- Most sensitive and specific method
- Can detect low-level parasitemia and mixed infections
- Not routinely available in emergency settings; used for confirmation and epidemiological purposes
- Especially useful for differentiating P. knowlesi from P. malariae
4. Laboratory Findings (supportive)
| Finding | Significance |
|---|---|
| Hemolytic anemia (normocytic) | Near-universal; severity reflects parasitemia |
| Thrombocytopenia | Very common; useful screening clue |
| Elevated LDH, indirect bilirubin | Hemolysis |
| Elevated creatinine | Renal involvement |
| Hypoglycemia | Especially in P. falciparum or with quinine |
| Elevated liver enzymes | Common; jaundice from hemolysis |
| Leukopenia or leukocytosis | Variable |
5. Travel History (Critical)
A comprehensive travel history is mandatory:
- Exact countries and dates visited
- Time spent in cities vs. rural/forested areas
- Prophylaxis compliance
- Mosquito precautions taken
- Symptom onset relative to return
Most fatalities in the developed world result from delayed diagnosis because patients and clinicians underestimate the risk of severe malaria in returning travelers. - Murray & Nadel's Respiratory Medicine
Key Species-Specific Diagnostic Clues on Blood Smear
| Feature | P. falciparum | P. vivax | P. ovale | P. malariae |
|---|---|---|---|---|
| RBC enlargement | No | Yes | Yes (oval shape) | No |
| Multiple infections per RBC | Yes | Rare | Rare | No |
| Schüffner's dots | No | Yes | Yes | No |
| Ziemann's stippling | No | No | No | Yes |
| Classic form | Ring (accolé), banana-shaped gametocytes | Ameboid trophozoites | Oval RBCs, fimbriated | "Band form" trophozoite |
Sources:
- Robbins & Kumar Basic Pathology (10th ed.), Ch. 10 (Hematopathology / Infectious Disease)
- Rosen's Emergency Medicine, Ch. 122 (Parasitic Infections)
- Murray & Nadel's Textbook of Respiratory Medicine, Ch. 58
How are the different Plasmodium species treated?
Finding Sources
Searching PubMed
"malaria" AND "treatment" AND "artemisinin"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Excellent - I now have the full treatment algorithm image plus comprehensive drug-by-drug and species-by-species content. I have everything needed for a thorough answer.
Treatment of Malaria by Plasmodium Species
Treatment Decision Algorithm
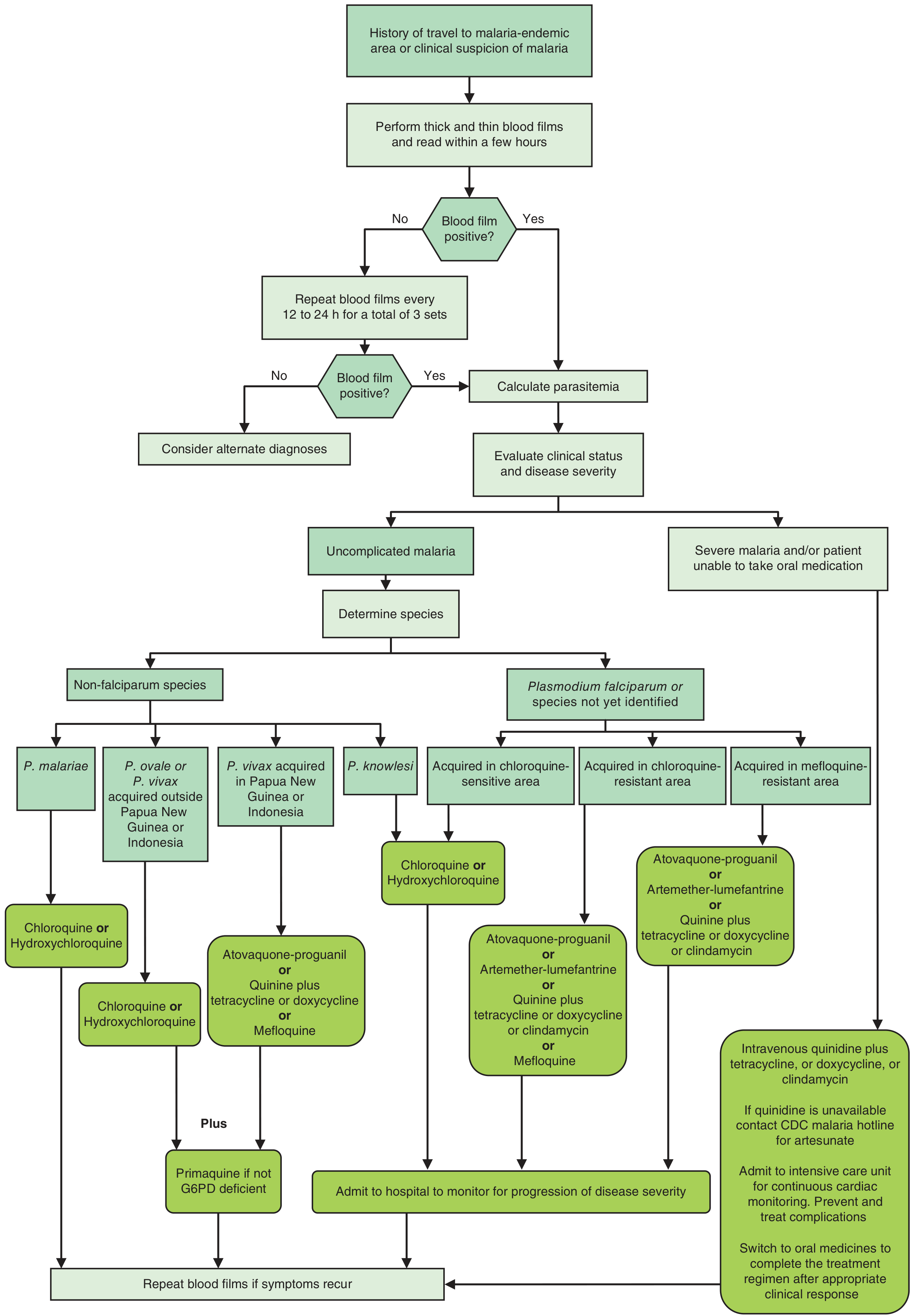
Fig. 66-3 - Decision algorithm for treatment of malaria, Goodman & Gilman's Pharmacological Basis of Therapeutics
Core Principle: Two Questions Drive Drug Choice
- Which species? (determines if you need radical cure for relapsing forms)
- Chloroquine-sensitive or resistant? (the single most important question for P. falciparum)
1. P. vivax and P. ovale (Relapsing Malaria)
These two species form dormant hypnozoites in the liver that cause relapses weeks to months after the initial infection. Treatment therefore has two components:
Blood-stage treatment (eliminates circulating merozoites)
| Acquisition region | Drug |
|---|---|
| Most areas | Chloroquine 25 mg/kg over 3 days (10 mg/kg day 1, 10 mg/kg day 2, 5 mg/kg day 3) |
| Papua New Guinea / Indonesia (P. vivax chloroquine-resistant) | Atovaquone-proguanil, or quinine + tetracycline/doxycycline, or mefloquine |
Radical cure (eliminates liver hypnozoites - prevents relapse)
| Drug | Dose | Notes |
|---|---|---|
| Primaquine | 0.25-0.5 mg/kg/day × 14 days | Supervised; most widely used |
| Tafenoquine | 300 mg single dose | Newer; more convenient |
Critical: Both primaquine and tafenoquine cause hemolysis in G6PD-deficient patients. Test for G6PD deficiency before prescribing. Both are contraindicated in pregnancy and in infants. - Goldman-Cecil Medicine
2. P. malariae
- No hypnozoites; no radical cure needed.
- Treated with chloroquine alone (same schedule as vivax).
- Generally mild and chloroquine-sensitive worldwide.
3. P. knowlesi (Zoonotic, SE Asia)
- More virulent course than P. malariae despite similar appearance.
- Treated with chloroquine or hydroxychloroquine (chloroquine-sensitive).
- If acquired in a chloroquine-resistant region, treat as chloroquine-resistant P. falciparum.
4. P. falciparum - Uncomplicated Disease
If acquired in chloroquine-SENSITIVE area
(Haiti, Dominican Republic, Central America north of Panama Canal, limited Middle East)
Chloroquine phosphate: 1 g → 500 mg at 6 h → 500 mg at 24 h → 500 mg at 48 h
If acquired in chloroquine-RESISTANT area (majority of the world)
Choose one of:
| Regimen | Adult Dose | Notes |
|---|---|---|
| Artemether-lumefantrine (Coartem) | 4 tabs twice daily × 3 days | First-line globally; FDA approved; no documented lumefantrine resistance |
| Atovaquone-proguanil (Malarone) | 4 tabs daily × 3 days | Excellent efficacy; well tolerated; expensive |
| Quinine + doxycycline | Quinine 650 mg TID × 3-7 days + doxycycline 100 mg BID × 7 days | Doxycycline not for children <8 years |
| Quinine + clindamycin | Quinine 650 mg TID × 7 days + clindamycin 600 mg BID × 7 days | For children and pregnant women |
| Mefloquine | 750 mg then 500 mg in 6-8 h | Single 1250 mg dose less tolerated; resistance in SE Asia |
If acquired in mefloquine-RESISTANT area (parts of SE Asia)
- Artesunate-mefloquine combination or dihydroartemisinin-piperaquine
- Artesunate-pyronaridine (newer; no documented resistance to either component)
ACT monotherapy is banned - artemisinin must always be used in combination to prevent resistance development. - Park's Preventive & Social Medicine
5. P. falciparum - Severe/Complicated Disease
Severe malaria is defined by: coma, convulsions, severe anemia (Hb <5 g/dL), renal failure (creatinine >3 mg/dL), jaundice (bilirubin >3 mg/dL), pulmonary edema/ARDS, hypoglycemia (glucose <40 mg/dL), hyperparasitemia (>5% RBCs infected), circulatory collapse, DIC, or hemoglobinuria.
Parenteral therapy is mandatory. This is a medical emergency.
| Drug | Dose | Notes |
|---|---|---|
| IV Artesunate (first-line) | 2.4 mg/kg at 0, 12, 24 h, then daily | Superior to quinine; fewer side effects; obtain via CDC Malaria Hotline (770-488-7788) in the US |
| IV Quinine dihydrochloride (alternative) | 20 mg/kg loading over 4 h, then 10 mg/kg every 8 h | Requires continuous cardiac monitoring (QT prolongation); not as efficacious as artesunate |
| IM Artemether (alternative) | 3.2 mg/kg IM, then 1.6 mg/kg/day | Not available in the US |
Switch to oral therapy once patient can tolerate it, and complete a full course (doxycycline, clindamycin, or full ACT).
Supportive care for severe malaria:
- Close nursing care and fluid/electrolyte maintenance
- Glucose monitoring and replacement (hypoglycemia is common, worsened by quinine)
- Respiratory support for ARDS
- Anticonvulsants for seizures
- Transfusion only if Hb <5 g/dL (avoid in pulmonary edema)
6. Malaria in Pregnancy
| Trimester | P. falciparum | P. vivax |
|---|---|---|
| 1st trimester | Quinine + clindamycin (ACTs avoided) | Chloroquine |
| 2nd & 3rd trimester | ACT (artemether-lumefantrine preferred) | Chloroquine |
- Primaquine and tafenoquine are contraindicated throughout pregnancy.
- Breastfeeding: chloroquine/hydroxychloroquine preferred; check infant G6PD before any primaquine.
7. Mixed Infections
Treat as the most severe species present - mixed infections with P. falciparum are treated with the P. falciparum regimen. Then add primaquine if P. vivax or P. ovale is confirmed, after G6PD testing.
ACT Regimens Used Globally (WHO-Recommended)
| ACT Combination | Where Used |
|---|---|
| Artemether-lumefantrine (Coartem) | First-line in most countries; FDA approved |
| Artesunate-amodiaquine (ASAQ) | First-line in parts of Africa |
| Artesunate-mefloquine | Standard in SE Asia (resistance emerging) |
| Dihydroartemisinin-piperaquine | Highly effective; resistance in SE Asia |
| Artesunate-pyronaridine | Newer; efficacious; no documented resistance |
A 2025 meta-analysis (Bohissou et al., BMC Infect Dis, PMID 41291512) confirmed ACT efficacy across sub-Saharan Africa 2010-2024, though with emerging resistance signals in some regions - reinforcing WHO recommendations to monitor treatment response and consider second-line agents where ACT failure is suspected.
Quick Reference by Species
| Species | Radical cure needed? | Blood-stage drug | Anti-relapse drug |
|---|---|---|---|
| P. falciparum | No | ACT or chloroquine (if sensitive) | Primaquine 0.75 mg/kg single dose (reduce transmission only) |
| P. vivax | Yes | Chloroquine (or ACT if resistant) | Primaquine × 14 days or tafenoquine single dose |
| P. ovale | Yes | Chloroquine | Primaquine × 14 days or tafenoquine single dose |
| P. malariae | No | Chloroquine | None needed |
| P. knowlesi | No | Chloroquine | None needed |
Sources:
- Goodman & Gilman's Pharmacological Basis of Therapeutics, Ch. 66
- Goldman-Cecil Medicine (International Ed.), Ch. 316
- Park's Textbook of Preventive & Social Medicine, Ch. on Malaria
- Katzung's Basic & Clinical Pharmacology, 16th Ed., Ch. 52
This is a shared conversation. Sign in to Orris to start your own chat.