How to differentiate normal vs infective etiology cxr
Normal vs. Infective Etiology on CXR
The Normal CXR - What You Should See
| Feature | Normal Appearance |
|---|---|
| Lung fields | Clear, black (air-filled), no opacities |
| Costophrenic angles | Sharp and acute bilaterally |
| Cardiothoracic ratio | < 0.5 on PA view |
| Hila | Bilateral, left slightly higher than right; no enlargement |
| Trachea | Midline |
| Hemidiaphragms | Right slightly higher than left; right at ~5th-6th rib anteriorly |
| Vascular markings | Present but traceable to hilum, not crowded |
| Pleural space | No effusion, no thickening |
Key Principle
Differentiation of aetiologies based solely on the radiograph is not reliable, yet the pattern of abnormalities is very useful for formulating a differential diagnosis. CXR is best used to determine the extent of pneumonia and detect complications (cavitation, abscess, pneumothorax, pleural effusion).
- Grainger & Allison's Diagnostic Radiology
Infective CXR - Three Main Patterns
1. Lobar (Airspace) Pneumonia
- Mechanism: Exudate starts in distal air spaces and spreads via pores of Kohn
- Appearance: Homogeneous opacification of a segment or entire lobe; air bronchogram present (air-filled bronchi visible within consolidated lung)
- Sharp margins at the interlobar fissure
- Common organisms: S. pneumoniae (most common), K. pneumoniae, Legionella, H. influenzae
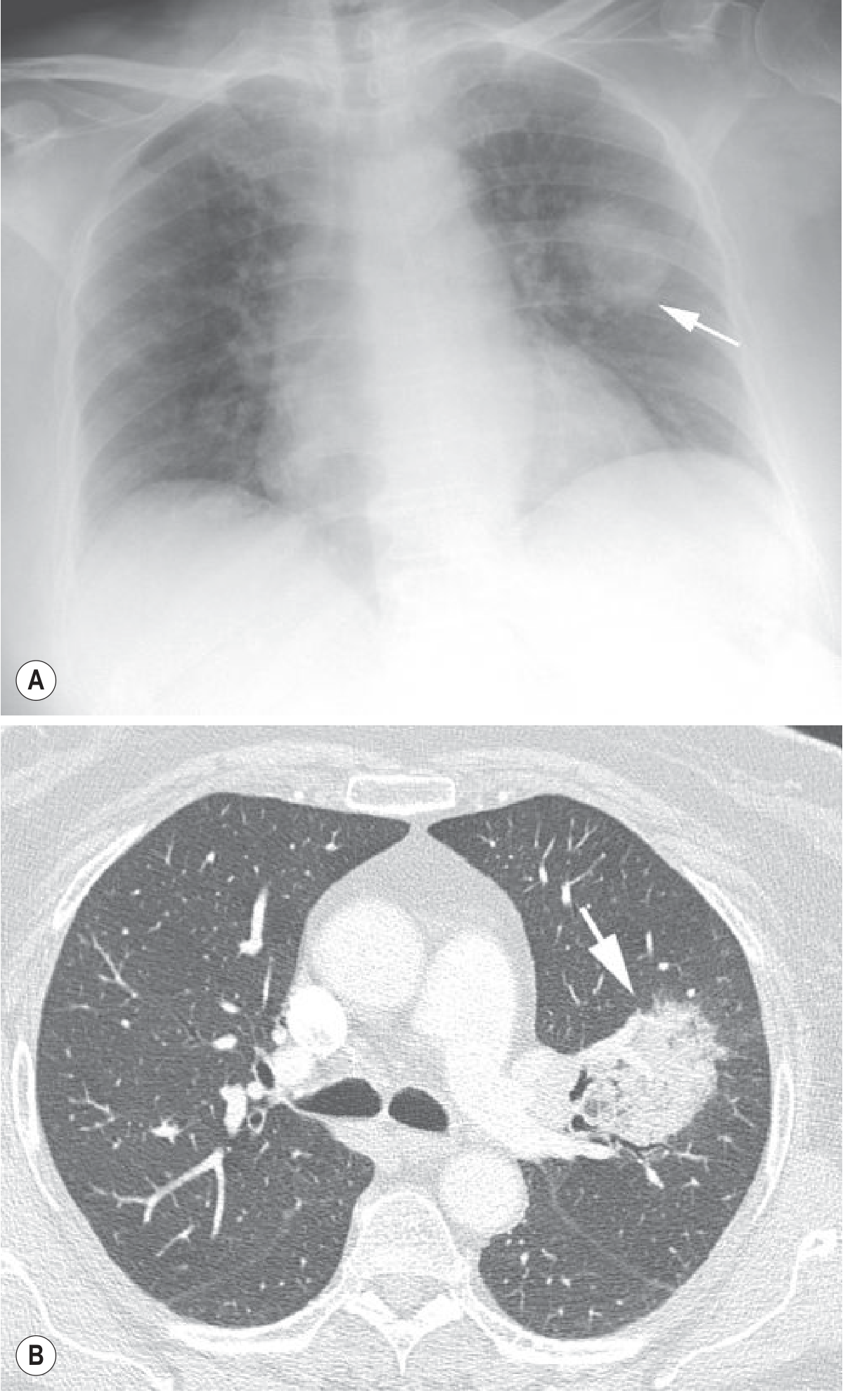
2. Bronchopneumonia (Lobular Pneumonia)
- Mechanism: Peribronchiolar inflammation spreading to surrounding lobules
- Appearance: Patchy, multifocal consolidation with poorly defined margins; air bronchogram usually absent
- On HRCT: centrilobular ill-defined nodules, branching linear opacities ("tree-in-bud"), multifocal lobular consolidation
- Common organisms: S. aureus, H. influenzae, P. aeruginosa, anaerobes
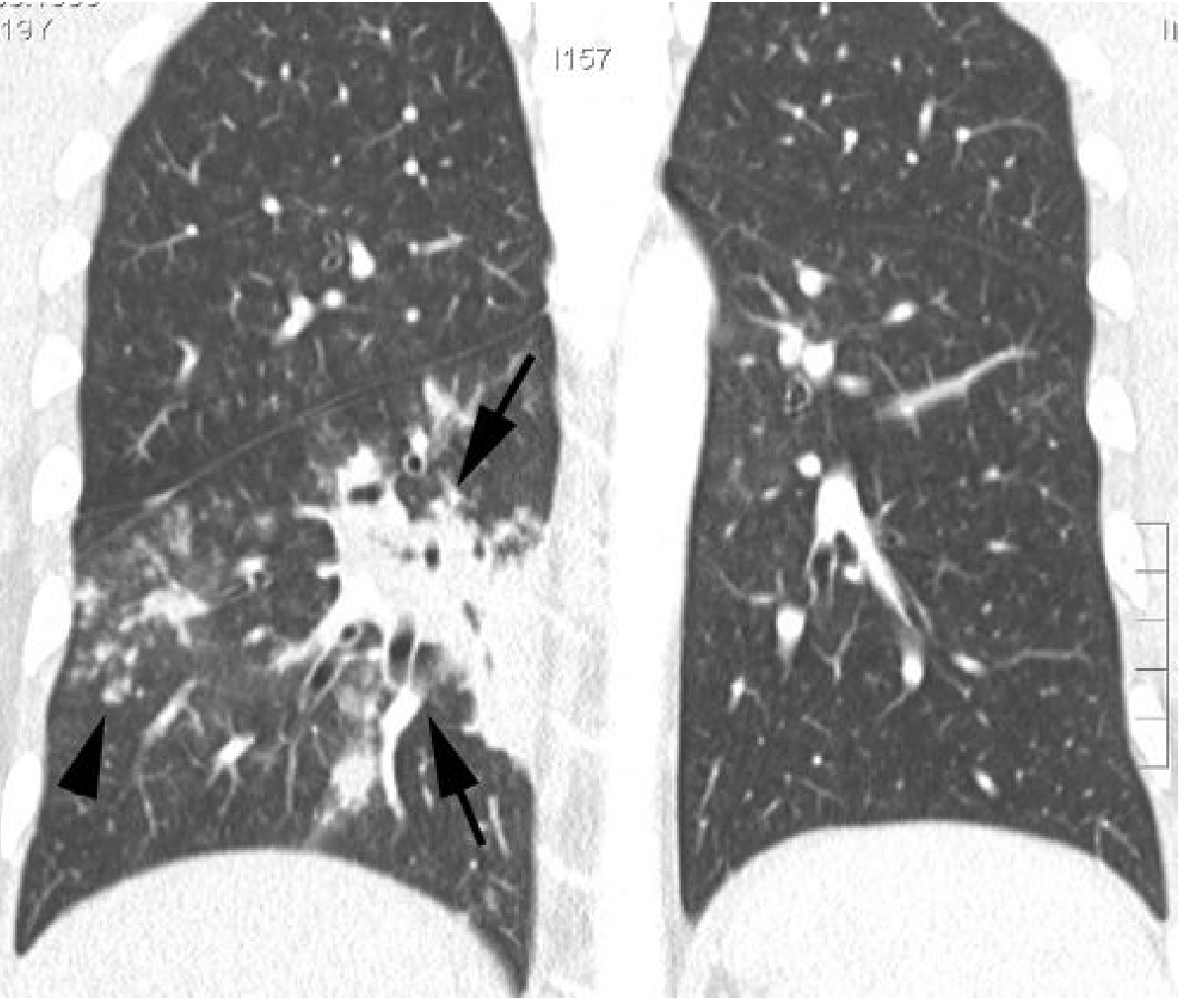
3. Interstitial (Atypical) Pneumonia
- Mechanism: Infection predominantly involving the interstitium rather than airspaces
- Appearance: Focal or diffuse small heterogeneous opacities, increased bronchovascular markings, bilateral perihilar haziness
- CXR can appear deceptively normal despite significant disease (notably in Pneumocystis jiroveci pneumonia - normal CXR in up to 10% of proven PCP)
- HRCT may show ground-glass opacity, smooth interlobular septal thickening - showing findings up to 5 days earlier than CXR
- Common organisms: Mycoplasma pneumoniae, viral (influenza, RSV, SARS-CoV-2), Chlamydia pneumoniae
Quick Differentiation Summary Table
| Feature | Normal CXR | Lobar Pneumonia | Bronchopneumonia | Interstitial Pneumonia |
|---|---|---|---|---|
| Lung fields | Clear | Lobar/segmental opacity | Patchy bilateral opacities | Diffuse fine haziness / normal |
| Air bronchogram | Absent | Present | Usually absent | Absent |
| Margins | N/A | Sharp (fissure-bound) | Ill-defined | Ill-defined/diffuse |
| Distribution | N/A | Lobar/segmental | Multifocal, bilateral | Bilateral perihilar |
| Hilar enlargement | Normal | May occur | May occur | Common (viral/Mycoplasma) |
| Pleural effusion | None | Can occur | Can occur | Less common |
| Cavitation | None | Rare (Klebsiella, Staph) | Can occur (Staph, anaerobes) | Rare |
| Classic organisms | - | Strep pneumo, Klebsiella | Staph, H. flu, Pseudomonas | Mycoplasma, viruses |
Complications That Indicate Infection (Not Normal)
- Lung abscess - cavity with air-fluid level; posterior upper lobe or superior lower lobe (aspiration-related); caused by anaerobes, S. aureus, P. aeruginosa, K. pneumoniae
- Pneumatoceles - thin-walled gas-filled cysts; typical of S. aureus pneumonia in children
- Empyema - loculated pleural effusion with pleural thickening
- Bulging fissure sign - lobar expansion suggests K. pneumoniae
- Hilar/mediastinal lymphadenopathy - suggests TB, fungal, viral
Important Caveats
- A normal CXR does not exclude pneumonia. Early pneumonia (first few hours), neutropenic patients, and PCP can all have a normal CXR despite clinical infection.
- HRCT is more sensitive - can detect pneumonia up to 5 days before it appears on CXR; recommended when clinical suspicion is high but CXR is normal.
- No pattern is pathogen-specific - radiological overlap is significant. CXR guides the differential, not a definitive microbiological diagnosis.
- Temporal resolution - CXR changes lag behind clinical improvement. Complete resolution can take 1-2 weeks (young, simple bacterial) up to 2 months (elderly, complex/atypical).
- Grainger & Allison's Diagnostic Radiology, Chapter 5
What is the shadow around hilar region
The Hilar Shadow on CXR
What Is the Normal Hilar Shadow?
| Structure | Contribution |
|---|---|
| Pulmonary arteries | ~90% of the hilar shadow - the dominant component |
| Pulmonary veins | Minor contribution, course inferiorly |
| Bronchial walls | Very minor - not visible on their own |
| Lymph nodes | Not visible on normal CXR; only seen when enlarged |
Normal characteristics:
- Left hilum is normally 0.5-1.5 cm higher than the right
- Concave outer border (convex = abnormal)
- Density = similar to overlying vascular structures
- Normal nodes are NOT visible on plain film - only CT/MRI can show normal-sized nodes
What Causes the "Shadow" Around the Hilum?
Causes of Abnormal Hilar Shadow
1. Lymph Node Enlargement (Lymphadenopathy)
| Cause | Laterality | Character |
|---|---|---|
| Sarcoidosis | Bilateral symmetrical (most common) | Dense, lobulated, well-demarcated; "potato nodes"; may calcify in "eggshell" or "icing sugar" pattern |
| Primary TB | Unilateral (right-sided more common) | Unilateral hilar + paratracheal = "1-2-3 sign" or Pawnbroker sign; seen in children especially |
| Lymphoma | Bilateral (± mediastinal widening) | Large, lobulated; progresses with parenchymal lesions unlike sarcoid |
| Malignancy (bronchogenic carcinoma) | Unilateral, ipsilateral to tumour | May reflect tumour itself, lymphadenopathy, or consolidated lung |
| Viral/Mycoplasma infection | Unilateral hilar | Mild; may be indistinguishable from primary TB in children |
Sarcoidosis is characterised by bilateral, symmetrical hilar and paratracheal lymphadenopathy. Hilar lymph node enlargement ranges from barely detectable to massive and gives the hila a dense lobulated and usually well-demarcated outline.
- Grainger & Allison's Diagnostic Radiology
In primary TB, consolidation of the lobe is associated with hilar lymphadenopathy - resembles acute bacterial pneumonia.
- Robbins & Cotran Pathologic Basis of Disease
2. Vascular Enlargement
| Cause | Pattern |
|---|---|
| Pulmonary arterial hypertension | Bilateral enlarged hilar arteries, "pruned tree" periphery |
| Left heart failure / mitral stenosis | Upper lobe blood diversion; enlarged veins; hazy hilar outlines |
| Large pulmonary embolism | Unilateral hilar enlargement (Palla's sign) |
| ASD/VSD (left-to-right shunt) | Bilateral hilar enlargement with plethoric lung fields |
3. Hilar Mass / Tumour
- Bronchogenic carcinoma (especially small cell, which is centrally located)
- Metastatic disease
- Carcinoid tumour
Summary: Normal vs. Abnormal Hilar Shadow
| Feature | Normal | Lymphadenopathy | Vascular Enlargement |
|---|---|---|---|
| Outline | Concave/flat lateral margin | Convex, lobulated | Convex, smooth |
| Laterality | Bilateral equal | Often bilateral | Bilateral |
| Density | Moderate | Increased | Increased |
| Calcification | None | In sarcoid/TB | None |
| Associated findings | None | Parenchymal nodules, consolidation | Pulmonary oedema, peripheral pruning |
Sarcoidosis - The Classic Bilateral Hilar Shadow
- Stage I: Lymphadenopathy only (bilateral symmetric hilar + paratracheal = "1-2-3 sign")
- Stage II: Lymphadenopathy + parenchymal opacity
- Stage III: Parenchymal opacity alone
- Stage IV: Pulmonary fibrosis
In 90% of patients with sarcoid lymphadenopathy, nodal enlargement is maximal on the first radiograph and disappears within 6-12 months. Recurrence is exceedingly rare.
- Grainger & Allison's Diagnostic Radiology
Can you show me the normal and abnormal xray
Normal vs. Abnormal Hilar Shadow - CXR Gallery
1. Normal CXR - PA View

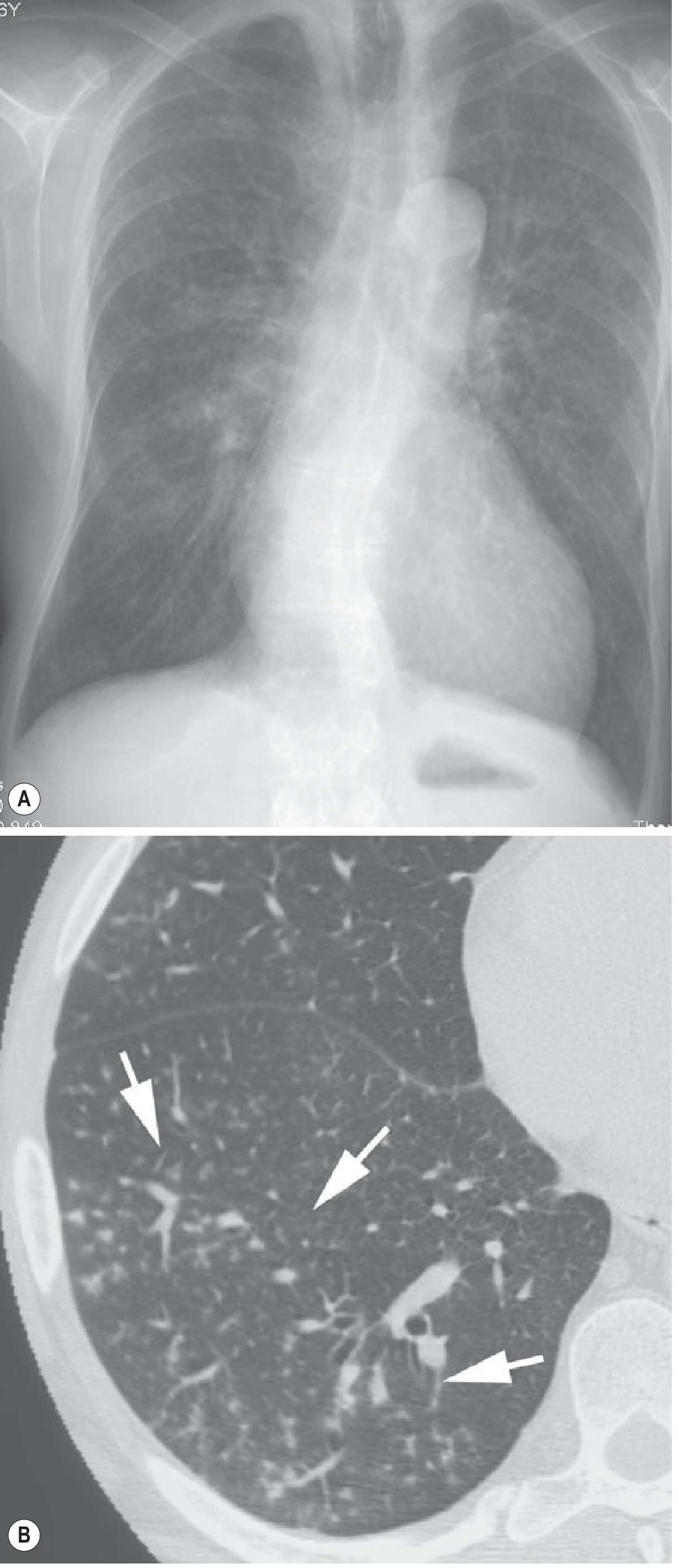
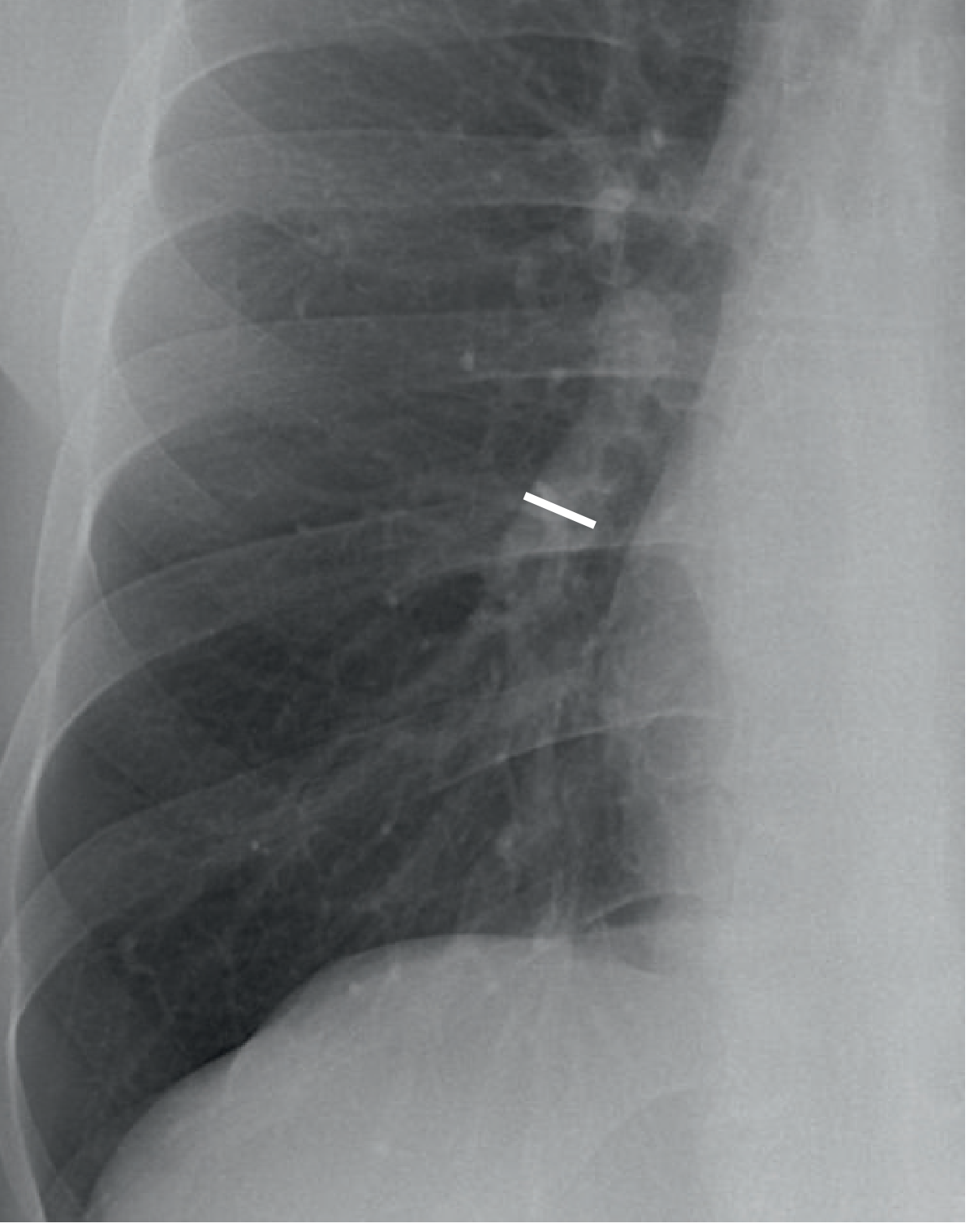
2. Normal CXR - Lateral View

3. Normal Hilar Anatomy - Labelled Diagram on Lateral CXR
4. Normal Frontal Hila - Lower Lobe Artery Measurement
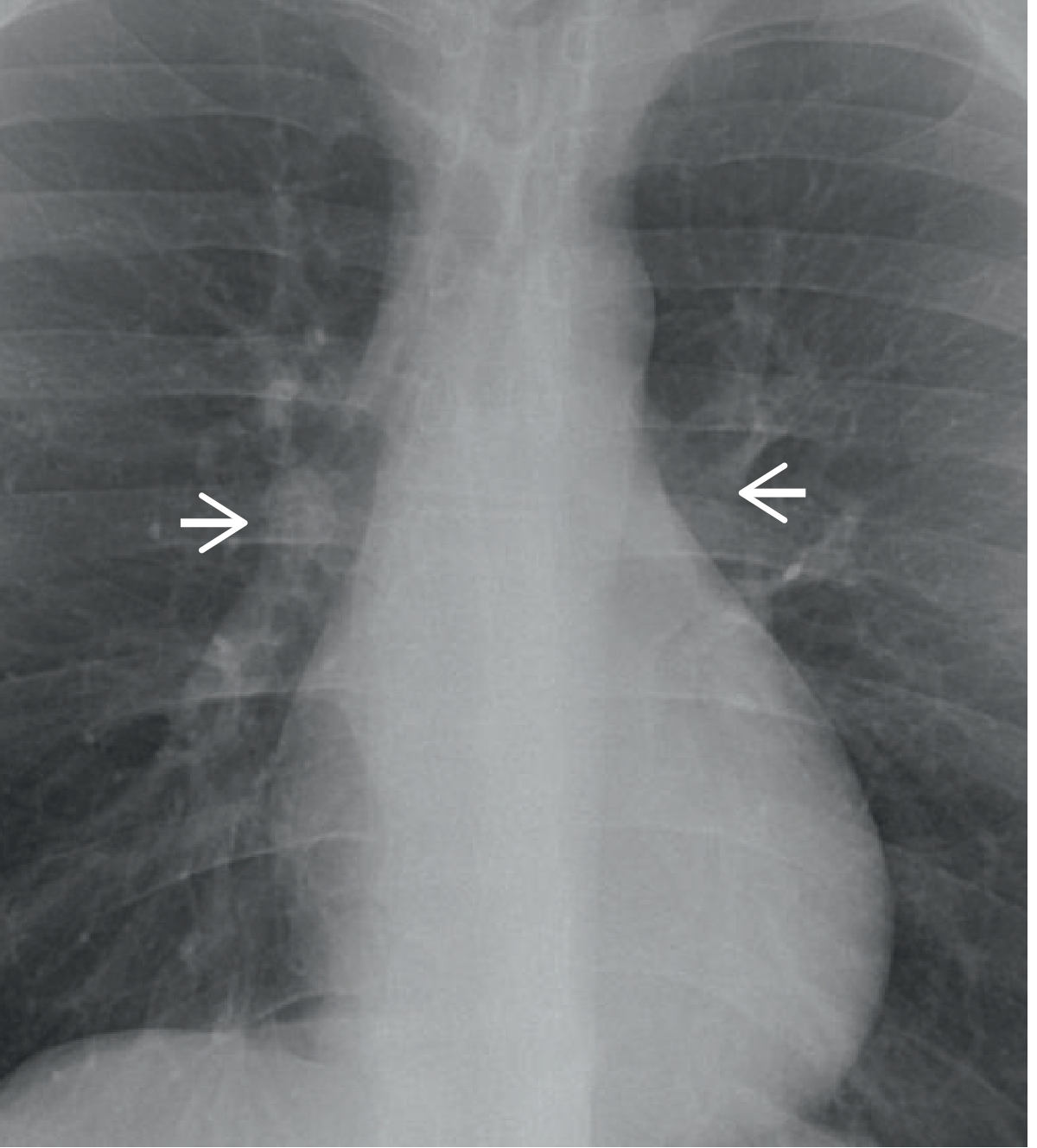
5. Abnormal - Bilateral Hilar Lymphadenopathy (Sarcoidosis) - CXR with Arrows
Sarcoidosis is characterised by bilateral, symmetrical hilar and paratracheal lymphadenopathy. Hilar lymph node enlargement gives the hila a dense lobulated and usually well-demarcated outline.
- Grainger & Allison's Diagnostic Radiology
6. Abnormal - Vascular Hilar Enlargement (Pulmonary Hypertension)
Quick Visual Comparison
| Normal | Lymphadenopathy (Sarcoid/TB) | Vascular (PAH) | |
|---|---|---|---|
| Hilar outline | Concave/subtle | Convex, lobulated | Convex, smooth |
| Size | Normal | Enlarged | Enlarged |
| Density | Moderate | Dense | Moderate-increased |
| Bilateral? | Yes (symmetrical) | Usually bilateral | Bilateral |
| Other clues | Clear lungs | ± parenchymal nodules | Pruned peripheral vessels |
Find current guidelines on sarcoidosis staging
"sarcoidosis"[MeSH Terms] AND "staging" AND "guidelines"
PMID: 41232941
PMID: 41224200
"sarcoidosis"[MeSH Terms] AND "diagnosis" AND "management"
ERS ATS sarcoidosis guidelines 2022 2023 2024 staging treatment
"sarcoidosis"[MeSH Terms] AND "treatment"
PMID: 34140301
ATS sarcoidosis clinical practice guideline 2020 Crouser staging Scadding limitations CT
https://www.aafp.org/afp/2024/0100/sarcoidosis
Current Guidelines on Sarcoidosis Staging
The Key Guidelines (Current as of 2026)
| Guideline | Year | Body | Scope |
|---|---|---|---|
| ATS Clinical Practice Guideline (Crouser et al.) | 2020 | American Thoracic Society | Diagnosis and detection |
| ERS Clinical Practice Guidelines (Baughman et al.) | 2021 | European Respiratory Society | Treatment (GRADE-based) |
| BTS Clinical Statement (Thillai et al.) | 2021 | British Thoracic Society | Pulmonary sarcoidosis |
| AAFP/AFP Review | 2024 | American Academy of Family Physicians | Evaluation and treatment |
| AHA Scientific Statement | 2024 | American Heart Association | Cardiac sarcoidosis |
The Scadding Staging System - Still the Standard for CXR
| Stage | CXR Findings | Frequency at Presentation | Spontaneous Resolution (untreated) |
|---|---|---|---|
| 0 | Normal CXR | 5-15% | N/A |
| I | Bilateral hilar/mediastinal lymphadenopathy only | 45-65% | 50-90% |
| II | Lymphadenopathy + parenchymal infiltrates | 30-40% | 30-70% |
| III | Parenchymal infiltrates only (no lymphadenopathy, no fibrosis) | 10-15% | 10-20% |
| IV | End-stage fibrosis (hilar distortion, upper lobe predominant) | 5% | 0% |
- Washington Manual of Medical Therapeutics; BTS Clinical Statement (Thillai et al., Thorax 2021)
Key prognostic rule: Acute onset disease (Löfgren's syndrome - fever, erythema nodosum, bilateral hilar lymphadenopathy, arthritis) carries an excellent prognosis with spontaneous resolution in >80%. Insidious onset carries a worse prognosis with risk of progressive fibrosis.
What the 2020 ATS Guideline Added Beyond Scadding
- Compatible clinical and radiographic presentation
- Non-necrotizing granulomas on tissue biopsy (at least one organ)
- Exclusion of alternative causes of granulomatous disease (especially TB, fungi)
- Baseline serum calcium in all patients (screens for hypercalcemia)
- Baseline eye examination for all patients (ocular sarcoidosis can be silent)
- HRCT over plain CXR when parenchymal infiltrates are present
The CT-Based Evolution: Beyond Scadding
| Modality | Role |
|---|---|
| CXR (Scadding) | Simple, cost-effective staging; does NOT correlate well with lung function |
| HRCT | Most precise - shows perilymphatic nodules, upper lobe predominance, fibrosis, traction bronchiectasis; best for quantifying fibrosis; guides biopsy site selection |
| PET scan | Assesses inflammatory activity and monitors therapy response; not for routine staging |
| Cardiac MRI | Standard for cardiac sarcoidosis detection (late gadolinium enhancement) |
CT is the most precise modality for stage classification and prognosis. Differentiating reversible inflammatory lesions from irreversible fibrotic lesions is critical for therapeutic decisions.
- Kostova et al., Rofo 2026 [PMID: 41224200]
Current Treatment Guidelines (ERS 2021 GRADE-Based)
| Scenario | Recommendation | Evidence |
|---|---|---|
| Mild/asymptomatic disease | No treatment - spontaneous resolution common | Grade C |
| Active pulmonary disease | Corticosteroids first-line (prednisone ~20-40 mg/day, taper over 6-12 months) | Grade B |
| Refractory or steroid-dependent | Methotrexate (second-line, steroid-sparing) | Grade C |
| Refractory to methotrexate | Azathioprine, leflunomide as alternatives | Grade C |
| Severe refractory | Anti-TNF agents (infliximab, adalimumab) - third-line, expert centres only | Grade C |
| End-stage fibrosis (Stage IV) | Lung transplantation consideration | Expert opinion |
| Fatigue | Neurostimulants (methylphenidate, armodafinil) may help | Insufficient evidence for formal recommendation |
Recent data (2026 state-of-the-art): Methotrexate and prednisone have comparable effects on pulmonary function but differ in side-effect profiles and time to efficacy. There is growing consensus to minimise corticosteroid use and adopt more evidence-based approaches.
- Miedema et al., Eur Respir J 2026 [PMID: 41232941]
Important Limitations of CXR Staging (All Current Guidelines Acknowledge This)
- Scadding stages do not predict disease activity - a patient can have active inflammation at any stage
- Stage does NOT equal treatment indication - treatment decisions are based on symptom burden, organ function, and risk of damage, not stage alone
- Up to 10-20% of Stage III patients can still resolve spontaneously
- Stage IV patients with fibrosis will NOT resolve but may stabilise
- Pulmonary function tests (FVC, DLCO) are more clinically meaningful than CXR stage alone
Summary: 2026 Clinical Approach Per Current Guidelines
Suspected Sarcoidosis
↓
CXR (Scadding stage) + HRCT if parenchymal disease
↓
Biopsy (non-necrotizing granulomas) - at least one organ
↓
Exclude TB/fungi/other granulomatous disease
↓
Baseline: serum Ca²⁺, eye exam, ECG, spirometry, DLCO
↓
Assess organ involvement + symptom burden
↓
Stage 0-I asymptomatic → Observe + monitor
Stage II-III symptomatic → Corticosteroids first-line
Refractory → Methotrexate / Azathioprine
Severe → Anti-TNF (infliximab)
Stage IV fibrosis → Supportive ± transplant referral
Treatment protocol for liver cirrhosis
"liver cirrhosis"[MeSH Terms] AND "management"
"cirrhosis"[MeSH Terms] AND "ascites" AND "portal hypertension"
Treatment Protocol for Liver Cirrhosis
STEP 1 - Treat the Underlying Cause
| Etiology | Treatment |
|---|---|
| Alcoholic liver disease | Complete alcohol cessation; consider steroids (prednisolone 40 mg/d) for alcoholic hepatitis; treat withdrawal |
| HBV cirrhosis | Entecavir or tenofovir (TDF/TAF) lifelong |
| HCV cirrhosis | Direct-acting antivirals (DAAs) - cure rates >95%; regression of fibrosis possible |
| MASLD/NASH cirrhosis | Weight loss, treat metabolic syndrome; resmetirom (FXR agonist) approved 2024 for earlier NASH |
| Autoimmune hepatitis | Prednisolone ± azathioprine (EASL 2025 guideline) |
| Haemochromatosis | Phlebotomy; deferasirox if phlebotomy not tolerated (EASL 2022) |
| PBC/PSC | Ursodeoxycholic acid (UDCA) for PBC; no proven disease-modifying therapy for PSC |
| Wilson's disease | D-penicillamine or trientine; zinc maintenance |
STEP 2 - General Measures for All Patients
- Alcohol abstinence (all patients, regardless of aetiology)
- Vaccinations: HAV, HBV, pneumococcal, influenza, COVID-19
- Nutrition: High-protein diet (1.2-1.5 g/kg/day); late evening snack to prevent overnight catabolism; avoid prolonged fasting
- Avoid NSAIDs - can precipitate renal failure and GI bleeding
- Avoid aminoglycosides - nephrotoxic
- Avoid sedatives/benzodiazepines - can precipitate hepatic encephalopathy
- Bone protection: Screen for and treat osteoporosis (common in cirrhosis)
- Monitor: 6-monthly ultrasound + AFP for HCC surveillance
STEP 3 - Managing Complications
A. Ascites
- Sodium restriction: 2 g/day (88 mmol/day)
- Diuretics - spironolactone + furosemide in ratio 100:40 mg/day
- Spironolactone max: 400 mg/day; Furosemide max: 160 mg/day
- Monitor: weight loss 0.5 kg/day (no peripheral oedema) or 1 kg/day (with oedema)
- If gynecomastia: substitute spironolactone with amiloride 5-40 mg/day
- Avoid: NSAIDs, ACE inhibitors, ARBs (worsen renal function)
-
Add midodrine (α1-agonist) ± clonidine - counteracts splanchnic vasodilation
-
Large-volume paracentesis (LVP): Remove >5 L; always give IV albumin 6-8 g per litre removed to prevent post-paracentesis circulatory dysfunction and death
-
TIPS (transjugular intrahepatic portosystemic shunt): Superior to LVP for reducing ascites reaccumulation; increases hepatic encephalopathy risk; no mortality difference
-
Caution: Beta-blockers in refractory ascites may be associated with decreased survival - reassess necessity
-
Harrison's Principles of Internal Medicine 22E (2025), p. 372
B. Spontaneous Bacterial Peritonitis (SBP)
- IV cefotaxime 2 g every 12 hours × 5 days (third-generation cephalosporin, covers gram-negative rods + streptococci)
- IV albumin 1.5 g/kg on day 1, then 1.0 g/kg on day 3 - reduces HRS risk and mortality
- Repeat paracentesis at 48 hours to confirm ≥25% reduction in PMN
- If nosocomial/healthcare-acquired SBP or critically ill: consider carbapenem (multidrug-resistant organisms)
-
Oral norfloxacin 400 mg/day (or ciprofloxacin 500 mg/day where norfloxacin unavailable) - indefinitely after first SBP
-
Also indicated: Ascitic protein <1 g/dL (high-risk), or active GI bleeding (use IV ceftriaxone in hospitalised patients)
-
Harrison's 22E; Rosen's Emergency Medicine
C. Variceal Haemorrhage
- Screen with upper endoscopy at diagnosis
- Small varices: non-selective beta-blocker (propranolol or carvedilol) if high-risk features (red wale marks, Child-Pugh B/C)
- Large varices: NSBBs OR endoscopic band ligation (EBL) - both equally effective
- Resuscitate - IV access, blood transfusion target Hb 7-8 g/dL (restrictive strategy)
- Vasoactive drugs: Terlipressin (first-line, 2 mg IV q4-6h), OR somatostatin/octreotide - start before endoscopy
- IV antibiotics: Ceftriaxone 1 g/day × 7 days (reduces SBP, rebleeding, mortality)
- Urgent endoscopy within 12 hours: Band ligation (EBL) ± sclerotherapy
- Balloon tamponade (Sengstaken-Blakemore tube) or SEMS (self-expanding metal stent) if endoscopy fails - bridge to TIPS
- TIPS: For refractory bleeding or Child-Pugh B/C with active bleeding at endoscopy (early TIPS improves survival)
- Combination of NSBB + EBL (superior to either alone)
- TIPS for those who fail pharmacological + endoscopic treatment
D. Hepatic Encephalopathy (HE)
- GI bleeding, infection (SBP, UTI), constipation, dehydration, hypokalemia, sedatives, renal failure, excessive protein intake
- Lactulose 15-45 mL PO 2-4×/day (or via NG tube if unable to swallow) - titrate to 2-3 soft stools/day; first-line
- Rifaximin 550 mg BD - add for episodes despite lactulose, or for prevention of recurrence (significantly reduces recurrence - NNT ~4)
- Zinc supplementation - if deficient (common in cirrhosis)
- Low-grade HE: Dietary protein restriction is NOT recommended - protein restriction worsens sarcopenia; maintain adequate protein intake
-
Rifaximin + lactulose combination reduces recurrence by ~49% vs lactulose alone
-
Mulholland & Greenfield's Surgery 7e; Washington Manual of Medical Therapeutics
E. Hepatorenal Syndrome (HRS)
-
First-line: IV terlipressin (0.5-2 mg q4-6h) + IV albumin 20-40 g/day - most established therapy; reversal rate ~40-50%
-
If terlipressin unavailable (e.g., USA): IV norepinephrine + albumin (ICU setting)
-
Alternative: Midodrine + octreotide + albumin (less effective)
-
TIPS can be considered in patients with HRS-CKD (previously Type 2)
-
Definitive treatment: Liver transplantation - only cure; bridge therapies aim to stabilise until transplant
-
Harrison's 22E (2025); Comprehensive Clinical Nephrology 7e; Miller's Anesthesia 10e
F. Hepatic Hydrothorax
- Same principles as ascites: sodium restriction + diuretics
- Thoracentesis if symptomatic (dyspnoea/hypoxia)
- TIPS for refractory cases
- Avoid chest tube (high morbidity/mortality in cirrhosis)
STEP 4 - Child-Pugh and MELD Scoring (Guide Treatment Intensity)
| Score | Variable |
|---|---|
| Child-Pugh | Bilirubin, albumin, PT/INR, ascites severity, encephalopathy grade - classifies A (5-6), B (7-9), C (10-15) |
| MELD-Na | Creatinine, bilirubin, INR, sodium - predicts 3-month mortality; used for transplant prioritisation |
- Child-Pugh C or MELD-Na ≥15 → urgent transplant evaluation
STEP 5 - Liver Transplantation
- MELD-Na ≥15 (mortality from liver disease exceeds transplant risk)
- Refractory ascites
- Recurrent SBP
- Recurrent variceal haemorrhage uncontrolled by medical/endoscopic therapy
- HRS unresponsive to vasoconstrictors
- Stage IV encephalopathy
- HCC within Milan criteria (single ≤5 cm or up to 3 nodules ≤3 cm each)
Summary Algorithm
Cirrhosis diagnosed
↓
Treat underlying cause + general measures
↓
Compensated (no complications) → Surveillance + prophylaxis + lifestyle
↓
Decompensated
├── Ascites → Na restrict + spironolactone/furosemide → LVP + albumin → TIPS
├── SBP → Cefotaxime + albumin → secondary norfloxacin prophylaxis
├── Varices → NSBB ± EBL prophylaxis → acute: terlipressin + EBL + antibiotics
├── HE → treat precipitant + lactulose + rifaximin
└── HRS → terlipressin + albumin → transplant
↓
MELD-Na ≥15 or refractory complications → Liver Transplant Evaluation
There are many treatments available to treat cirrhosis complications. Given the diverse nature, treatment decisions require an assessment of organ involvement, risk for significant morbidity, and impact on quality of life.
- ERS/EASL Guideline framework; EASL ACLF CPG 2023 [PMID: 37364789]
Treatment protocol for alcohol withdrawal
"alcohol withdrawal"[MeSH Terms] AND "treatment" AND "benzodiazepines"
"alcohol withdrawal syndrome"[MeSH Terms] AND "management"
"alcohol withdrawal" AND "delirium tremens" AND "treatment"
PMID: 34288186
alcohol withdrawal treatment protocol CIWA-Ar benzodiazepine regimen 2023 2024 guideline
PMID: 34523874
Treatment Protocol for Alcohol Withdrawal Syndrome (AWS)
Pathophysiology (Why It Happens)
Timeline of Symptoms
| Time after Last Drink | Symptoms |
|---|---|
| 4-12 hours | Tremor, anxiety, nausea, diaphoresis, tachycardia, hypertension - onset of uncomplicated withdrawal |
| 12-24 hours | Alcoholic hallucinosis (auditory/visual/tactile), autonomic instability |
| 24-48 hours | Peak seizure risk (generalised tonic-clonic) |
| 48-72 hours | Peak of uncomplicated withdrawal |
| 3-5 days | Delirium tremens (DTs) onset - if going to occur |
| ~7 days | DTs resolve if survived |
Uncomplicated withdrawal symptoms peak on day 2 and improve by day 4-5. DTs onset is 3-5 days after cessation with ~8% mortality if untreated.
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry
STEP 1 - Risk Stratification Using CIWA-Ar
| CIWA-Ar Score | Severity | Management |
|---|---|---|
| < 8 | Mild | Supportive care; pharmacotherapy may not be needed |
| 8-15 | Moderate | Pharmacotherapy indicated (benzodiazepines or alternatives) |
| > 15 | Severe | Intensive inpatient management; high risk for DTs/seizures |
A CIWA-Ar score >8-12 generally calls for active pharmacologic management, whether fixed-dose or symptom-triggered.
- Symptom to Diagnosis: An Evidence-Based Guide, 4e
STEP 2 - Determine Setting
- Mild withdrawal (CIWA-Ar < 10)
- No prior seizures or DTs
- No significant comorbidities
- Reliable social support, able to comply
- Daily review for up to 5 days after last drink
-
Moderate-severe withdrawal (CIWA-Ar ≥ 10-15)
-
Prior history of seizures or DTs
-
Unable to cooperate with outpatient therapy
-
Comorbid psychiatric or medical conditions (including liver disease)
-
Failed outpatient detoxification
-
Concurrent benzodiazepine dependence
-
Symptom to Diagnosis 4e; AFP 2021 [PMID: 34523874]
STEP 3 - Immediate Measures on Presentation (All Patients)
A. Thiamine FIRST - Before Any Glucose
- IV thiamine 100 mg before giving any glucose-containing fluids (prevents precipitating or worsening Wernicke encephalopathy)
- In suspected Wernicke encephalopathy (confusion, ataxia, ophthalmoplegia): IV thiamine 200-500 mg TDS until symptoms resolve
- Also give: folate, pyridoxine (B6), multivitamin
B. Electrolyte Correction
- Check and replace: potassium, magnesium, phosphate (all commonly depleted in alcoholism)
- Magnesium depletion lowers seizure threshold - replace IV/PO as needed
- IV fluids if dehydrated (use normal saline, not 5% dextrose until after thiamine)
C. Monitoring
- Vital signs and CIWA-Ar every 1-4 hours depending on severity
- Blood glucose, LFTs, FBC, coagulation, electrolytes, creatinine
- Quiet, low-stimulus environment; fall precautions
STEP 4 - Pharmacological Treatment
First-Line: Benzodiazepines
| Drug | Route | Half-life | Notes |
|---|---|---|---|
| Diazepam | PO/IV | Long (20-100h) | Preferred for severe withdrawal; smooth taper due to active metabolites; avoid in severe liver disease |
| Chlordiazepoxide | PO | Long (5-30h) | Standard for planned detox; less IV abuse potential |
| Lorazepam | PO/IV/IM | Intermediate (10-20h) | Preferred in liver failure (no active metabolites), elderly, respiratory compromise |
| Oxazepam | PO | Short (5-15h) | Safe in liver disease; no active metabolites |
UK guidelines: Use one benzodiazepine only (chlordiazepoxide or diazepam). Avoid multiple benzodiazepines. - UK Draft Clinical Guidelines for Alcohol Treatment
Strategy 1 - Symptom-Triggered (Preferred where monitoring is adequate)
- Dose given only when CIWA-Ar ≥ 8-10
- Example: Lorazepam 1-2 mg PO/IV or Diazepam 5-10 mg PO when CIWA-Ar ≥ 8-10, repeat hourly as needed
- Advantage: avoids over-sedation, uses less total benzodiazepine, shorter treatment duration
- Requires frequent skilled nursing assessments (every 1-2h)
Strategy 2 - Fixed-Schedule (Use if adequate monitoring not available)
- Delivers regular doses regardless of symptoms
- Example Chlordiazepoxide fixed taper (typical inpatient schedule):
| Day | Chlordiazepoxide dose |
|---|---|
| Day 1 | 30 mg QID (120 mg/day) |
| Day 2 | 20 mg QID (80 mg/day) |
| Day 3 | 10 mg QID (40 mg/day) |
| Day 4 | 5 mg QID (20 mg/day) |
| Day 5 | Stop |
- Adjust up or down based on patient response; careful monitoring still required to avoid undertreatment or oversedation
Mild Withdrawal Alternatives (Outpatient)
- Carbamazepine 200 mg TDS-QID - effective for mild-moderate withdrawal, no seizure/DT prevention data for severe; preferred in some European guidelines
- Gabapentin 300-600 mg TDS - reduces withdrawal symptoms, may also help with post-withdrawal cravings
- Both can be used as alternatives or adjuncts to benzodiazepines in mild cases
STEP 5 - Adjunctive Medications
| Drug | Role | Notes |
|---|---|---|
| Beta-blockers (propranolol, atenolol) | Reduce autonomic hyperactivity (tachycardia, hypertension, tremor) | Not to be used alone - mask sympathetic signs that guide benzodiazepine dosing; useful adjunct only |
| Clonidine (α2-agonist) | Reduces autonomic symptoms | Adjunct; does not prevent seizures or DTs |
| Haloperidol | Controls hallucinations/agitation in DTs | Adjunct to benzodiazepines; lowers seizure threshold - never monotherapy |
| Magnesium sulphate | Reduces seizure risk if hypomagnesaemic | Replace IV if Mg²⁺ < 0.7 mmol/L |
STEP 6 - Refractory / Severe Withdrawal (ICU Level)
| Agent | Dose/Route | Notes |
|---|---|---|
| Phenobarbital | 10-20 mg/kg IV load, then 60-120 mg Q6-8h | Effective where benzodiazepines fail; comparable outcomes in some studies; risk of respiratory depression |
| Propofol | Infusion in intubated patient | For intubated patients in refractory DTs; requires ICU |
| Dexmedetomidine | 0.2-1.5 mcg/kg/h IV infusion | α2-agonist; onset 15 min, half-life 2h; reduces sympathetic tone without respiratory depression; excellent adjunct in ICU; does not prevent seizures alone |
| Ketamine | Adjunctive infusion | Emerging evidence for refractory AWS |
Refractory alcohol withdrawal syndromes are often treated with phenobarbital, propofol, or dexmedetomidine. Dexmedetomidine is an α2-agonist more potent than clonidine that decreases sympathetic tone without causing respiratory depression.
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry
STEP 7 - Delirium Tremens (DTs) - Specific Management
- ICU admission - continuous monitoring
- High-dose IV benzodiazepines - diazepam 10 mg IV q5-10min or lorazepam 2-4 mg IV q15-20min until calm
- Phenobarbital if benzodiazepine-refractory
- Propofol/intubation if unable to protect airway or extremely agitated
- Dexmedetomidine as adjunct to reduce sympathomimetic storm
- Haloperidol for psychotic features (adjunct only - never monotherapy for DTs)
- Correct hyperthermia, fluid/electrolyte imbalances
- Treat precipitating illness (infection, GI bleed, etc.)
STEP 8 - Post-Withdrawal / Long-Term Management
| Drug | Mechanism | Notes |
|---|---|---|
| Naltrexone 50 mg OD PO (or 380 mg IM monthly) | Opioid antagonist - reduces craving and reward | First-line for AUD maintenance; avoid in acute opioid use |
| Acamprosate 666 mg TDS | NMDA/GABA modulator - reduces cravings | Safe in liver disease; avoid in renal failure |
| Disulfiram 250-500 mg OD | Acetaldehyde dehydrogenase inhibitor - aversion therapy | Requires motivation; avoid in cardiovascular disease, psychosis |
| Baclofen | GABA-B agonist | Evidence in cirrhosis; used in some European centres |
| Nalmefene | Opioid system modulator | Licensed in Europe for "as-needed" use to reduce drinking |
- Psychosocial support: Brief intervention, motivational interviewing, AA/SMART Recovery, CBT
- AFP 2021 [PMID: 34523874] - "Primary care physicians should offer to initiate long-term treatment for AUD, including pharmacotherapy, in addition to withdrawal management"
Summary Algorithm
Patient with possible alcohol withdrawal
↓
Thiamine 100 mg IV BEFORE any glucose fluids
↓
CIWA-Ar assessment + electrolytes + bloods
↓
CIWA-Ar < 8 CIWA-Ar 8-15 CIWA-Ar > 15
Mild Moderate Severe
Supportive care Outpatient or Inpatient mandatory
± carbamazepine/ inpatient High-dose benzos
gabapentin Benzodiazepines (symptom-triggered)
(fixed or ± phenobarbital
symptom-triggered) ICU if DTs
↓
Adjuncts: propranolol (autonomic), magnesium (seizures), haloperidol (hallucinations)
↓
Refractory: phenobarbital → propofol/dexmedetomidine → intubation
↓
Post-withdrawal: naltrexone / acamprosate + psychosocial support
Careful monitoring and prompt patient-specific adjustment of benzodiazepine dose is the key to successful management of the alcoholic patient.
- Symptom to Diagnosis 4e