Neonatal hyperbilirubememia paediatrics from ghai
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive and well-illustrated content. Let me compile a detailed, Ghai-style answer covering all the key aspects of neonatal hyperbilirubinemia.
Neonatal Hyperbilirubinemia
Note: Ghai's Essential Paediatrics is not available in this library. The content below is drawn from Rosen's Emergency Medicine and Tietz Textbook of Laboratory Medicine - both authoritative sources that closely follow the same AAP-based framework Ghai uses.
Definition
Neonatal jaundice (icterus neonatorum) is the yellow discoloration of the skin and sclerae due to elevated serum bilirubin. It becomes clinically visible when total serum bilirubin (TSB) rises above ~5 mg/dL. Nearly every newborn develops an unconjugated bilirubin >1 mg/dL (the adult upper limit) in the first week of life.
Bilirubin Metabolism in the Neonate
Three physiologic factors combine to produce neonatal jaundice:
- Increased bilirubin production - Fetal Hb has a shorter RBC lifespan (~70-90 days vs. 120 days in adults); neonates have a higher RBC mass that breaks down rapidly after birth.
- Decreased clearance and excretion - Immature hepatic glucuronyl transferase activity limits conjugation.
- Increased enterohepatic resorption - Neonatal gut flora is sparse; unconjugated bilirubin is reabsorbed from the gut.
Unconjugated (indirect) bilirubin is lipid-soluble and crosses the blood-brain barrier, making it neurotoxic. Conjugated (direct) hyperbilirubinemia in neonates is always pathological.
Classification
A. Unconjugated (Indirect) Hyperbilirubinemia
| Category | Causes |
|---|---|
| Physiologic / Benign | Physiologic jaundice of the newborn, Breast milk jaundice |
| Hemolytic | ABO incompatibility, Rh incompatibility, G6PD deficiency, Spherocytosis, Elliptocytosis, Sickle cell, Thalassemia, Pyruvate kinase deficiency, Cephalhematoma |
| Infectious | TORCHS infections, UTI, Sepsis |
| Metabolic / Endocrine | Hypothyroidism, Hypopituitarism, Galactosemia |
| Inherited enzyme defects | Crigler-Najjar syndrome (Type I - complete UGT1A1 deficiency; Type II - partial), Gilbert syndrome |
| Other | Dehydration, Polycythemia, Swallowed blood |
B. Conjugated (Direct) Hyperbilirubinemia - Always Pathological
- Biliary atresia
- Neonatal hepatitis (viral, metabolic)
- Choledochal cyst
- Alagille syndrome (bile duct paucity)
- TORCHS infections with hepatic involvement
- Gram-negative sepsis
- TPN-associated cholestasis
- Dubin-Johnson / Rotor syndromes
Physiologic Jaundice
- Occurs in ~50% of normal term newborns
- Bilirubin peaks on day 2-5 of life (usually day 3)
- Peak level typically does not exceed 12-13 mg/dL in term infants
- Resolves within 2 weeks in term infants, up to 3 weeks in preterm
- Absent on day 1 - any jaundice within 24 hours of birth is pathological
Mechanism
Immature glucuronyl transferase + high Hb turnover + increased enterohepatic circulation.
Breast Milk Jaundice
- Second most common cause of neonatal jaundice
- Pathophysiology uncertain: may be hormonally mediated or from increased enterohepatic resorption of bilirubin
- Peaks later than physiologic jaundice: around day 10-21
- Elevated levels may persist 3-10 weeks
- Mild unconjugated hyperbilirubinemia; typically <15 mg/dL
- Breast-feeding jaundice (distinct): occurs in first week from poor intake/dehydration - treated by optimizing feeds
Risk Factors for Severe Hyperbilirubinemia
- Prematurity (especially 35-37 weeks)
- Isoimmune hemolysis (ABO/Rh incompatibility)
- G6PD deficiency
- Sepsis
- Cephalhematoma
- Dehydration
- Hereditary spherocytosis
- East Asian ethnicity
Neurotoxicity: Bilirubin-Induced Neurologic Dysfunction (BIND)
Unconjugated bilirubin crosses the blood-brain barrier and deposits in the basal ganglia, subthalamic nuclei, and brainstem nuclei causing cell death.
Acute Bilirubin Encephalopathy (ABE) - Early, potentially reversible
- Phase 1 (Mild): Poor feeding, lethargy, hypotonia, high-pitched cry
- Phase 2 (Moderate): Hypertonia, retrocollis (neck arching), opisthotonos, fever, irritability
- Phase 3 (Severe): Seizures, coma, death
Kernicterus - Chronic, irreversible sequelae of BIND
- Choreoathetoid cerebral palsy
- Sensorineural hearing loss
- Upward gaze palsy (Parinaud-like)
- Intellectual disability
- Dental dysplasia
Risk increases significantly at TSB >20-25 mg/dL in term infants.
Clinical Assessment
Jaundice appears in a cephalocaudal progression (Kramer's zones):
| Zone | Area | Approximate bilirubin (mg/dL) |
|---|---|---|
| 1 | Face/head | ~5-7 |
| 2 | Chest to umbilicus | ~8-11 |
| 3 | Umbilicus to knees | ~12-15 |
| 4 | Knees to ankles | ~15-18 |
| 5 | Palms and soles | >18-20 |
Note: Clinical estimation is unreliable; always confirm with serum/transcutaneous measurement.
Indications for Evaluation (Red Flags)
- Jaundice appearing within 24 hours of birth
- Elevated direct (conjugated) bilirubin at any level
- Rapidly rising TSB unexplained by history/exam
- TSB approaching exchange transfusion threshold or not responding to phototherapy
- Jaundice persisting beyond 3 weeks of age
- Sick-appearing infant
Diagnostic Workup
- Transcutaneous bilirubinometry (TcB): Quick screening for well-appearing infants >24 hours, not applicable post-phototherapy
- Total and fractionated serum bilirubin (direct vs. indirect)
- Blood group and Coombs (DAT): ABO/Rh incompatibility
- CBC with peripheral smear: Hemolysis, polycythemia, spherocytes
- G6PD screen
- In sick infants: blood glucose, electrolytes, urine reducing substances, serum ammonia, lactate, blood culture, LFTs
- Conjugated hyperbilirubinemia workup: USG abdomen, HIDA scan, liver biopsy (biliary atresia)
Management
1. Phototherapy
Light in the blue-green spectrum (430-490 nm) converts unconjugated bilirubin in the skin via:
- Photoisomerization (lumirubin) - main pathway, water-soluble, excreted without conjugation
- Structural isomerization
- Photooxidation
Indications: TSB exceeds the age- and risk-stratified AAP threshold (see graph below).
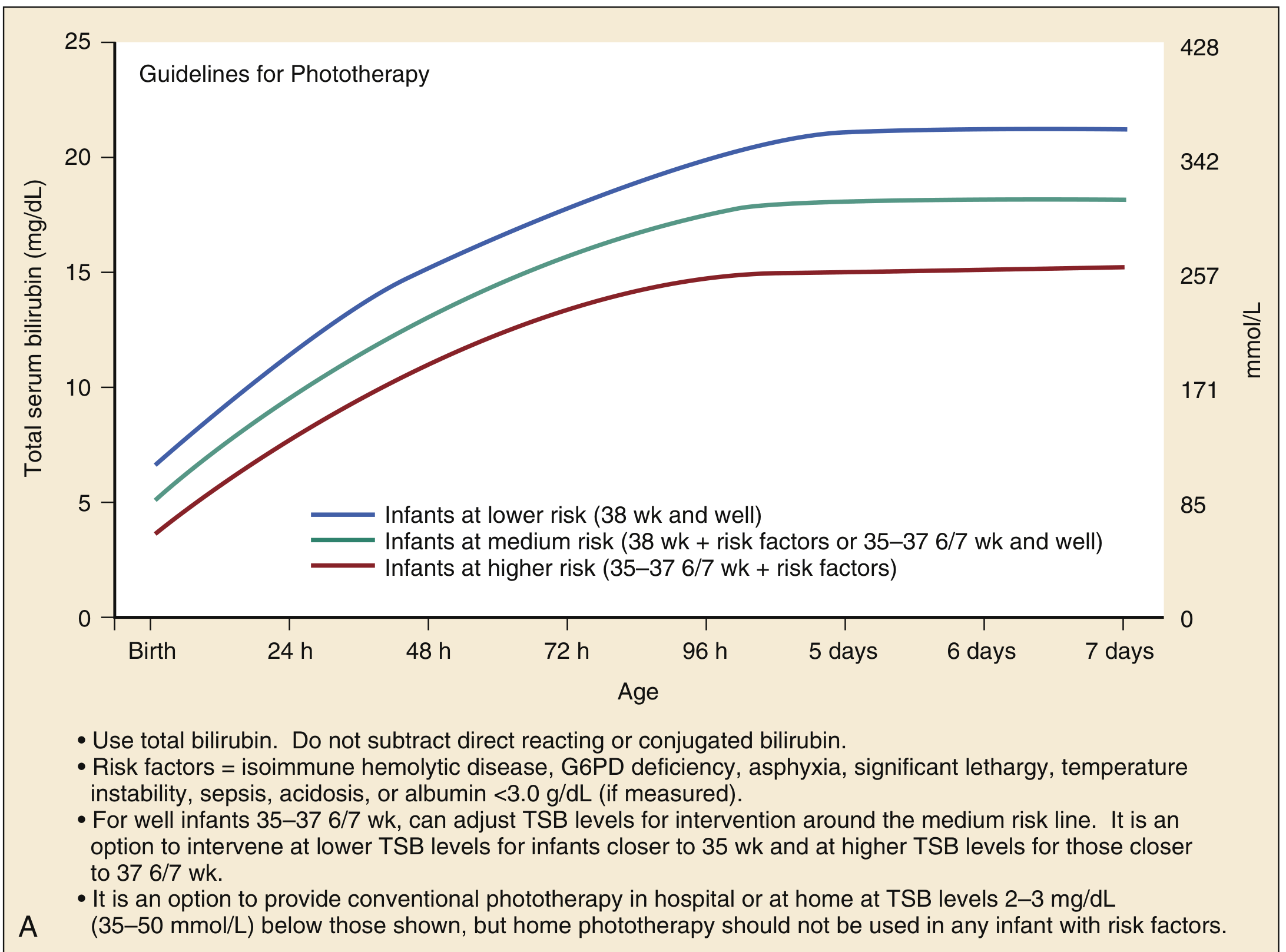
Risk factors (for placing in higher-risk category):
- Isoimmune hemolytic disease
- G6PD deficiency
- Asphyxia
- Significant lethargy
- Temperature instability
- Sepsis / acidosis
- Albumin <3.0 g/dL
Intensive phototherapy: All lights on maximum intensity; expose maximum skin surface area; maintain hydration.
Side effects of phototherapy: Bronze baby syndrome (with direct hyperbilirubinemia), loose stools, hyperthermia, dehydration, retinal damage (cover eyes), skin rash.
2. Exchange Transfusion
The most effective and rapid method to remove bilirubin.
Indications:
- TSB above age-specific AAP exchange transfusion threshold (see graph below)
- Failure of phototherapy (TSB continues to rise despite intensive phototherapy)
- Jaundiced infant with signs/symptoms of BIND
- Immediate exchange if TSB is 5 mg/dL above the threshold line
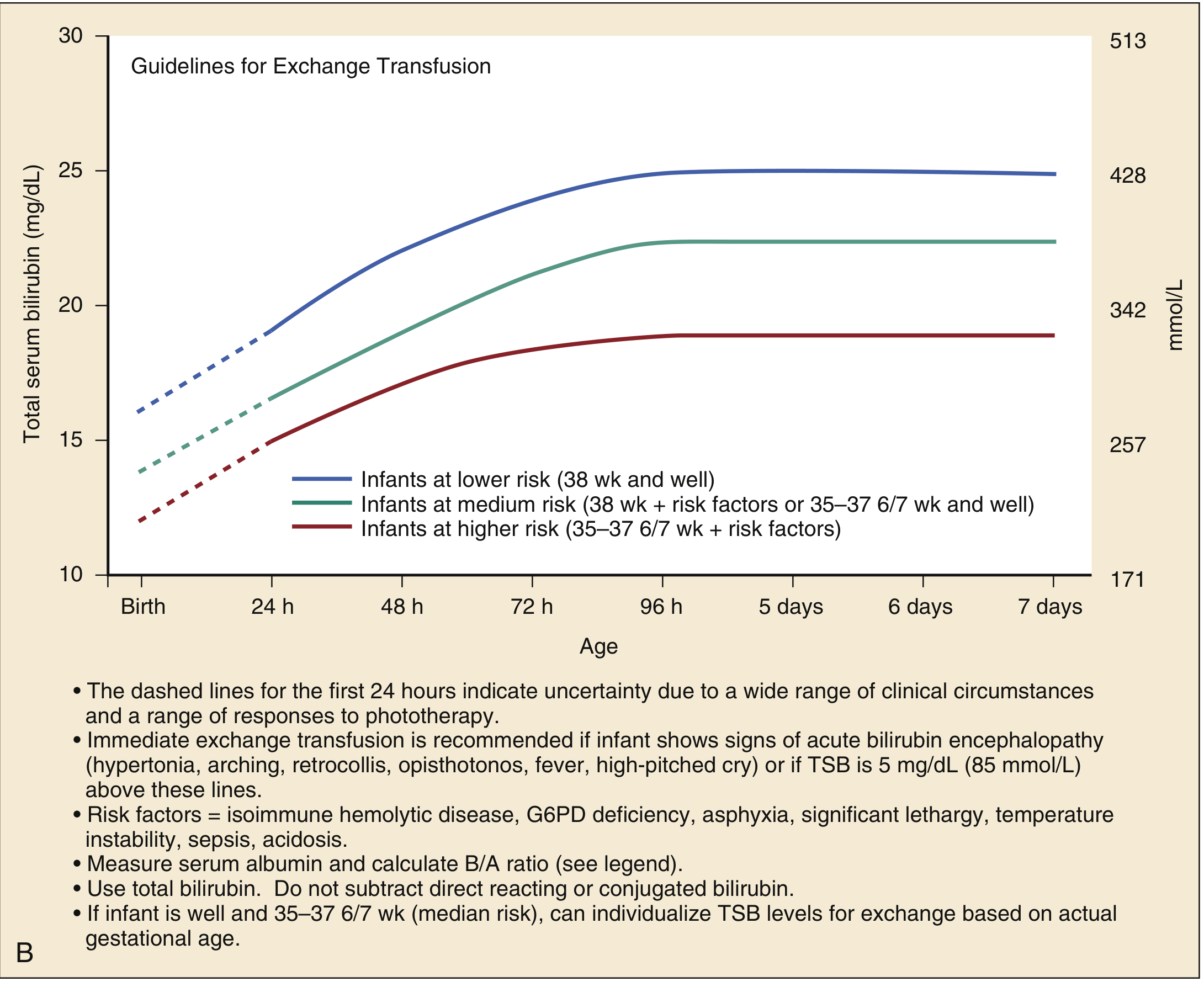
Procedure: Double-volume exchange (180-190 mL/kg packed RBCs) via umbilical venous catheter. Serial aliquots of 5-10 mL/kg are removed and replaced. Replaces ~85% of infant's blood volume and reduces TSB by at least 50%.
Complications: Electrolyte disturbances, thrombocytopenia, NEC, air embolism, infection, cardiac arrhythmia, death (~1%).
3. Intravenous Immunoglobulin (IVIG)
Used in isoimmune hemolytic disease (ABO/Rh). Blocks Fc receptors on macrophages and reduces hemolysis. Dose: 0.5-1 g/kg IV.
4. Tin-mesoporphyrin
Heme oxygenase inhibitor - reduces bilirubin production. Not routinely used.
5. Supportive
- Ensure adequate hydration and feeding (reduces enterohepatic circulation)
- Treat underlying cause (sepsis, hypothyroidism, metabolic disorders)
- Home phototherapy is an option for otherwise well, term infants with reliable caregivers + follow-up within 24 hours
Disposition
| Situation | Management |
|---|---|
| TSB above phototherapy threshold | Phototherapy (inpatient or home based on severity) |
| Ill-appearing, poor feeding, unable to maintain intake | Hospital admission, phototherapy, IV hydration |
| TSB approaching or above exchange threshold | NICU admission, exchange transfusion |
| Direct hyperbilirubinemia (any) | Admit for evaluation; subspecialty consultation |
| Responding to phototherapy, well-appearing | Outpatient follow-up within 24 hours |
Prognosis
- Physiologic and breast milk jaundice: Excellent, self-limiting
- BIND/kernicterus: Devastating if untreated; 70% mortality in severely affected term infants in historical series; survivors have severe neurologic sequelae
- Early intervention with phototherapy and exchange transfusion prevents kernicterus
Sources: Rosen's Emergency Medicine, 9e (Ch. 166); Tietz Textbook of Laboratory Medicine, 7e (Ch. 51); AAP Subcommittee on Hyperbilirubinemia guidelines (Pediatrics, 2004;114:297-316)
Difference between breastfeeding jaundice and brestmilk jaundice
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Excellent - I now have comprehensive textbook content from multiple sources. Here is the full comparison:
Breastfeeding Jaundice vs. Breast Milk Jaundice
These are two distinct syndromes that are commonly conflated. The key distinction is: one is caused by too little breast milk (feeding problem), the other by something in breast milk itself (milk composition problem).
Side-by-Side Comparison
| Feature | Breastfeeding Jaundice | Breast Milk Jaundice |
|---|---|---|
| Other names | Starvation jaundice, Breast-non-feeding jaundice, Lactation failure jaundice | Late-onset breast milk jaundice |
| Timing of onset | Days 2-5 (first week of life, early) | After day 4-7, peaks around day 10-21 |
| Cause | Inadequate milk intake / dehydration - mother's milk supply not yet established | Substance(s) in mature breast milk that inhibit bilirubin clearance |
| Mechanism | Poor oral intake → reduced bowel movements → reduced bilirubin excretion via GI tract + relative dehydration → accentuates physiologic jaundice (increased enterohepatic circulation) | β-glucuronidases and other factors in breast milk deconjugate bilirubin in the gut → increased enterohepatic resorption. May also be hormonally mediated (pregnanediol inhibiting glucuronyl transferase) |
| Bilirubin type | Unconjugated (indirect) | Unconjugated (indirect) |
| Peak bilirubin level | Can be significant, parallels physiologic jaundice but worsened by dehydration | Usually mild - rarely exceeds 20 mg/dL; typically 10-20 mg/dL |
| Duration | Resolves when feeds improve (within days) | May persist 3-10 weeks before gradually declining |
| Weight pattern | Excessive weight loss (>10% birth weight), poor weight gain | Weight gain usually normal once milk supply established |
| Urine output | Reduced (few wet diapers) | Normal |
| Stool frequency | Reduced | Normal |
| Risk of kernicterus | Can be significant if severe and untreated | Unlikely to cause kernicterus - generally benign |
| Treatment | Optimize feeding - encourage frequent breastfeeding; supplementation with expressed breast milk, donor milk, or formula as needed if severe | Continue breastfeeding; phototherapy if TSB reaches treatment threshold. Temporary cessation of breastfeeding for 24-48 hours causes rapid decline in bilirubin (but is not routinely recommended) |
| Serum bilirubin trend | Follows physiologic curve but higher/slower to fall | Continues rising after day 5-7, persists beyond 2 weeks |
Pathophysiology - Detailed
Breastfeeding Jaundice
The mother's colostrum is transitioning to mature milk in the first 2-4 days. During this period, if the infant is not fed frequently enough (or latch is poor), caloric and fluid intake is insufficient. This leads to:
- Dehydration → concentrated bilirubin, reduced renal excretion
- Reduced gut motility and stooling → bilirubin already excreted into gut gets reabsorbed (increased enterohepatic circulation)
- Net effect: amplification of physiologic jaundice
Breast Milk Jaundice
The exact mechanism is not fully established, but two main theories exist:
- β-glucuronidase theory: Mature breast milk contains β-glucuronidases that deconjugate bilirubin glucuronide in the neonatal gut back to unconjugated bilirubin, which is then reabsorbed
- Pregnanediol / fatty acid inhibition theory: Certain hormones and fatty acids in breast milk inhibit hepatic UDP-glucuronyl transferase (UGT1A1), reducing bilirubin conjugation
- Lipoprotein lipase theory: Unsaturated fatty acids from lipolysis of milk triglycerides may also inhibit conjugation
(Robbins Pathologic Basis of Disease notes: β-glucuronidases in milk impair bilirubin conjugation)
Diagnostic Clue - Temporary Cessation Test
If breast milk jaundice is suspected, temporarily stopping breastfeeding for 24-48 hours causes a rapid fall in bilirubin (confirming the diagnosis). This test is rarely needed in clinical practice and cessation is not routinely recommended as it may disrupt breastfeeding.
Management Summary
Breastfeeding jaundice:
- Increase frequency of breastfeeding (8-12 feeds/day)
- Ensure proper latch and milk transfer
- Supplement with expressed breast milk / formula only if medically indicated (e.g., >10% weight loss, poor wet diapers)
- Phototherapy if TSB reaches threshold
- Do NOT give glucose water (no benefit, may reduce breast milk intake)
Breast milk jaundice:
- Continue breastfeeding - reassure the mother
- Monitor TSB to ensure it is not approaching treatment threshold
- Phototherapy if TSB reaches threshold
- Temporary interruption of breastfeeding for 24-48 h may be considered diagnostically or if TSB is rising significantly, but is not routine
- Total and direct bilirubin should be checked in any infant with jaundice beyond 3 weeks to rule out pathologic conjugated causes
Memory Aid
| Breastfeeding Jaundice | Breast Milk Jaundice | |
|---|---|---|
| Mnemonic | "Not enough milk IN" | "Something IN the milk" |
| Week | Week 1 (early) | Week 2 onwards (late) |
| Fix | Feed more | Usually self-limiting |
Sources: Tintinalli's Emergency Medicine, 8e (Ch. 116); Rosen's Emergency Medicine, 9e (Ch. 166); Textbook of Family Medicine, 9e (Ch. 21); Robbins Pathologic Basis of Disease, 10e
This is a shared conversation. Sign in to Orris to start your own chat.