Head injury management
Reading File
Finding Sources
Finding Sources
Searching PubMed
"traumatic brain injury" AND "management"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile the full, detailed response.
Head Injury Management
Head injury (traumatic brain injury, TBI) management centers on one core principle: the primary injury cannot be reversed, so all efforts target prevention of secondary brain injury. Secondary injury arises from raised ICP, hypoxia, hypotension, seizures, hyperglycemia, hyperthermia, and impaired autoregulation.
1. Classification of TBI Severity
Based on Glasgow Coma Scale (GCS) at presentation:
| Severity | GCS | Findings |
|---|---|---|
| Mild | 13-15 | Concussion, brief LOC or none |
| Moderate | 9-12 | Confusion, amnesia, focal deficits |
| Severe | 3-8 | Coma, requires ICU management |
2. Primary Survey - ATLS Approach
All TBI patients are managed first with standard ATLS resuscitation. Secondary brain injury begins within minutes and is directly worsened by systemic hypoxia and hypotension.
Airway & Breathing
- Intubate if GCS ≤8 or airway is compromised
- Target SpO2 ≥90% (PaO2 ≥60 mmHg); hypoxia is directly toxic to injured neurons
- Avoid prophylactic hyperventilation (PaCO2 <30 mmHg) - it causes vasoconstriction and worsens ischemia. Hyperventilation is reserved for acute herniation as a temporizing measure only
Circulation - Blood Pressure Targets
Hypotension (SBP <90 mmHg) is one of the most potent predictors of mortality in TBI:
- Ages 15-49 or >70 years: maintain SBP >110 mmHg
- Ages 50-69 years: maintain SBP >100 mmHg
- A 10-point drop in SBP across the range 40-119 mmHg is associated with an 18.8% increase in in-hospital mortality (Brain Trauma Foundation, Level III)
(Schwartz's Principles of Surgery, 11th Ed.)
Disability
- GCS score, pupillary response, lateralizing signs
- Cervical spine immobilization if indicated (high-energy mechanism, age >65, fall >3m, serious multi-trauma)
3. Imaging
- Non-contrast CT head is the first-line imaging modality for moderate/severe TBI
- Identifies epidural, subdural, subarachnoid hemorrhage, contusions, skull fractures, midline shift
- CT angiography if vascular injury is suspected
- Concussion: Routine CT/MRI is NOT indicated if GCS is 15 and there are no red flag features; structural imaging is normal in concussion
4. ICP Monitoring
Indications (Brain Trauma Foundation - Level IIB):
- Severe TBI (GCS 3-8 after resuscitation) + abnormal CT scan
- Severe TBI + normal CT if patient is >40 years, shows motor posturing, or SBP <90 mmHg (Level III)
Treatment thresholds:
- Treat ICP when >20-22 mmHg
- Target Cerebral Perfusion Pressure (CPP) = MAP - ICP: range 60-70 mmHg
- Avoid aggressive attempts to raise CPP >70 mmHg (risk of ARDS)
- Avoid CPP <50 mmHg
(Bradley and Daroff's Neurology in Clinical Practice; Schwartz's Surgery)
5. Medical Management of Raised ICP
Hyperosmolar Therapy
- Mannitol: 0.25-1 g/kg IV - Level II evidence; first-line for acute ICP crises. Restrict use without ICP monitoring to those with signs of herniation
- Hypertonic saline: 3% at 2-5 mL/kg IV over 15 min for acute ICP crises (pediatric guideline); increasingly preferred in adults due to less diuresis-related hypotension
Sedation & Analgesia
- Propofol is recommended for ICP control (not for mortality benefit)
- Avoid fentanyl and midazolam boluses during ICP crises (can cause acute ICP spikes)
- High-dose barbiturates (pentobarbital/thiopental) for ICP refractory to all other measures - hemodynamic stability essential before use
Head Position
- 30-degree head-of-bed elevation reduces ICP
- Head neutral (avoid jugular venous compression)
Hyperventilation
- Target PaCO2 35-40 mmHg normally
- Brief hyperventilation to PaCO2 30-35 mmHg only as a bridge to definitive treatment during acute herniation
Temperature
- Fever must be actively controlled (antipyretics ± cooling); hyperthermia is toxic to injured neurons
- Prophylactic hypothermia is NOT recommended (no mortality benefit shown)
(Bradley and Daroff's; Schwartz's; Rosen's Emergency Medicine)
6. What NOT to Do - Contraindicated Therapies
| Intervention | Evidence | Recommendation |
|---|---|---|
| Corticosteroids | CRASH trial (n=9,673): methylprednisolone increased 6-month mortality (47% vs 42%, p=0.0024) | Level I: CONTRAINDICATED in TBI |
| Prophylactic hyperventilation | Worsens cerebral ischemia | Avoid |
| Prophylactic hypothermia | No mortality benefit | Not recommended |
| Routine ventricular catheter exchange/prophylactic antibiotics for EVD | No infection benefit | Not recommended |
7. Seizure Prophylaxis
- Levetiracetam (Keppra): 1g loading dose + 500mg twice daily x 7 days
- Reduces incidence of early post-traumatic seizures (within 7 days)
- No evidence supports long-term prophylaxis beyond 7 days
- Phenytoin is the historically studied agent, but Keppra is preferred in practice due to a better side-effect profile
(Schwartz's Principles of Surgery)
8. Other Medical Management
Glucose control: Hyperglycemia is toxic to injured neurons - monitor and control with sliding-scale insulin.
GI prophylaxis: Head injury patients have elevated risk of peptic ulceration (Cushing's ulcers from raised ICP); use PPI or H2 blocker prophylaxis.
DVT prophylaxis:
- Mechanical (intermittent pneumatic compression stockings) - initiate immediately
- Low-molecular-weight heparin or unfractionated heparin may be added - reasonable to initiate 24 hours after hematoma deemed stable
- Risk-benefit analysis required; risk of hematoma expansion vs. PE/DVT
Anticoagulation reversal: If patient is on anticoagulants and has intracranial hemorrhage, reverse to INR <1.3 within 4 hours - associated with reduced hematoma expansion (19.8% vs 41.5%).
9. Surgical Management
Epidural hematoma (EDH):
- Surgical evacuation if >30 mL, >15mm thickness, or >5mm midline shift
- Emergency craniotomy if clinical deterioration (blown pupil, GCS drop)
Subdural hematoma (SDH):
- Acute SDH with thickness >10mm or midline shift >5mm: surgical evacuation
- Burr-hole drainage may suffice for chronic SDH
Intracerebral contusions/hemorrhage:
- Surgical if: significant mass effect, refractory ICP, or accessible location with neurological deterioration
Depressed skull fracture:
- Open/compound depressed fractures need surgical elevation and debridement
- Closed depressed fractures: surgical if depression >thickness of skull, over eloquent cortex, or cosmetically significant
Decompressive craniectomy:
- For refractory elevated ICP not responsive to medical management
- Bifrontal or unilateral hemicraniectomy
10. Surgical Timing Consideration
The PRIMARY GOAL per Sabiston's Textbook of Surgery is to prevent secondary brain injury - the penumbra of recoverable cells around the traumatic focus. Early airway control, hemorrhage control, and normalization of blood pressure/oxygenation are the highest-priority interventions.
11. Pediatric Considerations
The pediatric brain has unique vulnerabilities: higher water content, less myelination, predisposing it to diffuse axonal injury. Key differences in management:
- Target CPP >40 mmHg, ICP treatment threshold <20 mmHg
- Seizure prophylaxis with phenytoin or levetiracetam
- Bolus 3% hypertonic saline at 2-5 mL/kg for ICP crises
- Avoid fentanyl/midazolam boluses during ICP crises
- Concussion: no routine CT unless red flag features; return-to-play protocol is gradual
(Rosen's Emergency Medicine, Brain Trauma Foundation Pediatric Guidelines 2019)
12. Brain Death Assessment
Applicable after severe TBI when clinical exam is consistent:
Requirements: normotension, normothermia, no sedatives/paralytics
Criteria: nonreactive pupils, absent corneal/oculocephalic/oculovestibular reflexes, positive apnea test (no breathing with PaCO2 ≥60 mmHg)
Confirmatory studies: cerebral angiography, radionuclide scan, transcranial Doppler (to-and-fro pattern), or EEG silence
Summary Algorithm
Head Injury
↓
Primary Survey (ABCs) + C-spine control
↓
Correct hypotension (SBP >110) + hypoxia (SpO2 >90%)
↓
GCS + Neurological Exam + Non-contrast CT Head
↓
Mild TBI (GCS 13-15) Moderate-Severe TBI (GCS ≤12)
↓ ↓
Observation/discharge ICU admission
(if CT normal) ICP monitoring (if GCS ≤8)
↓
Medical: Mannitol/HTS, Keppra, head-up 30°,
normoglycemia, antipyretics, PPIs
↓
Surgical if: mass lesion, herniation,
refractory ICP
Sources:
- Schwartz's Principles of Surgery, 11th Ed. - Management of Traumatic Brain Injury
- Sabiston Textbook of Surgery - Traumatic Brain Injury Management
- Bradley and Daroff's Neurology in Clinical Practice - Table 62.5, Guidelines for Severe TBI
- Rosen's Emergency Medicine - Box 160.8, Emergent Management of Severe TBI
- Morgan and Mikhail's Clinical Anesthesiology, 7th Ed. - Management Considerations for Acute TBI
Management of seizure in children
Reading File
Finding Sources
Finding Sources
Searching PubMed
"seizures" AND "children" AND "management"
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Reading File
I now have all the key information needed for a comprehensive answer. Let me compile everything.
Management of Seizures in Children
1. Definitions and Epidemiology
- Epilepsy is defined (ILAE) as: (1) ≥2 unprovoked seizures >24 hours apart; OR (2) one unprovoked seizure with ≥60% recurrence risk over 10 years; OR (3) diagnosis of an epilepsy syndrome
- ~1-1.5% of children will have a non-febrile seizure in their lifetime
- Febrile seizures are the most common seizure condition in pediatrics, occurring in ~4-5% of children aged 6-60 months
(Kaplan & Sadock's Comprehensive Textbook of Psychiatry; Harriet Lane Handbook, 23rd Ed.)
2. Seizure Classification (ILAE)
| Onset Type | Subtypes |
|---|---|
| Focal onset | Aware / Impaired awareness; Motor (automatisms, clonic, tonic) / Non-motor |
| Generalized onset | Motor: tonic-clonic, clonic, tonic, myoclonic; Non-motor: absence |
| Unknown onset | Tonic-clonic, epileptic spasms |
3. Febrile Seizures
Simple vs. Complex
| Feature | Simple | Complex |
|---|---|---|
| Duration | <15 minutes | ≥15 minutes |
| Focality | Generalized (non-focal) | Focal onset |
| Recurrence in 24h | No | Yes (≥2 in 24h) |
| Age | 6-60 months | Any |
Management of Simple Febrile Seizure
- Identify the source of fever - this is the primary workup
- No routine neuroimaging, EEG, or bloodwork required in a well-appearing, fully immunized child with normal neuro exam and no meningeal signs
- Lumbar puncture: NOT routinely indicated
- Do consider LP if: <6 months of age, signs of meningitis, incomplete immunizations (H. influenzae type b, S. pneumoniae), pretreated with antibiotics
- Children 6-12 months: consider LP if immunization status unknown
- Antiseizure medications: NOT required for a simple febrile seizure
- Recurrence risk: >33% - counsel family
(Harriet Lane Handbook, 23rd Ed.; Tintinalli's Emergency Medicine; Rosen's Emergency Medicine)
Long-term AED Prophylaxis for Febrile Seizures
- Not recommended for simple febrile seizures
- Small increased risk (~2-5%, double the baseline) of developing afebrile epilepsy - family counseling is important
4. Acute Seizure Management (Active Seizure)
Immediate Priorities (All Seizures)
- Position - lateral decubitus (recovery position) to prevent aspiration
- Airway - nasopharyngeal airway if needed; avoid oral airways (risk of vomiting post-seizure)
- Oxygen - by nasal cannula or face mask; bag-valve-mask if ventilation inadequate
- C-spine protection if trauma suspected
- IV/IO access - send glucose (bedside), electrolytes (Na, Ca, Mg), CBC, LFTs, AED levels, urine toxicology
- Correct metabolic causes: hypoglycemia (D10W 5 mL/kg IV in children), hyponatremia, hypocalcemia, hypomagnesemia
- Head-of-bed elevation if raised ICP is suspected
5. Status Epilepticus - Step-by-Step Protocol
Definition: Continuous seizure activity >30 minutes, OR repeated seizures without return to baseline consciousness
Key principle: Every 10-minute delay in starting benzodiazepines is associated with higher death rates, longer seizure duration, and more complications.
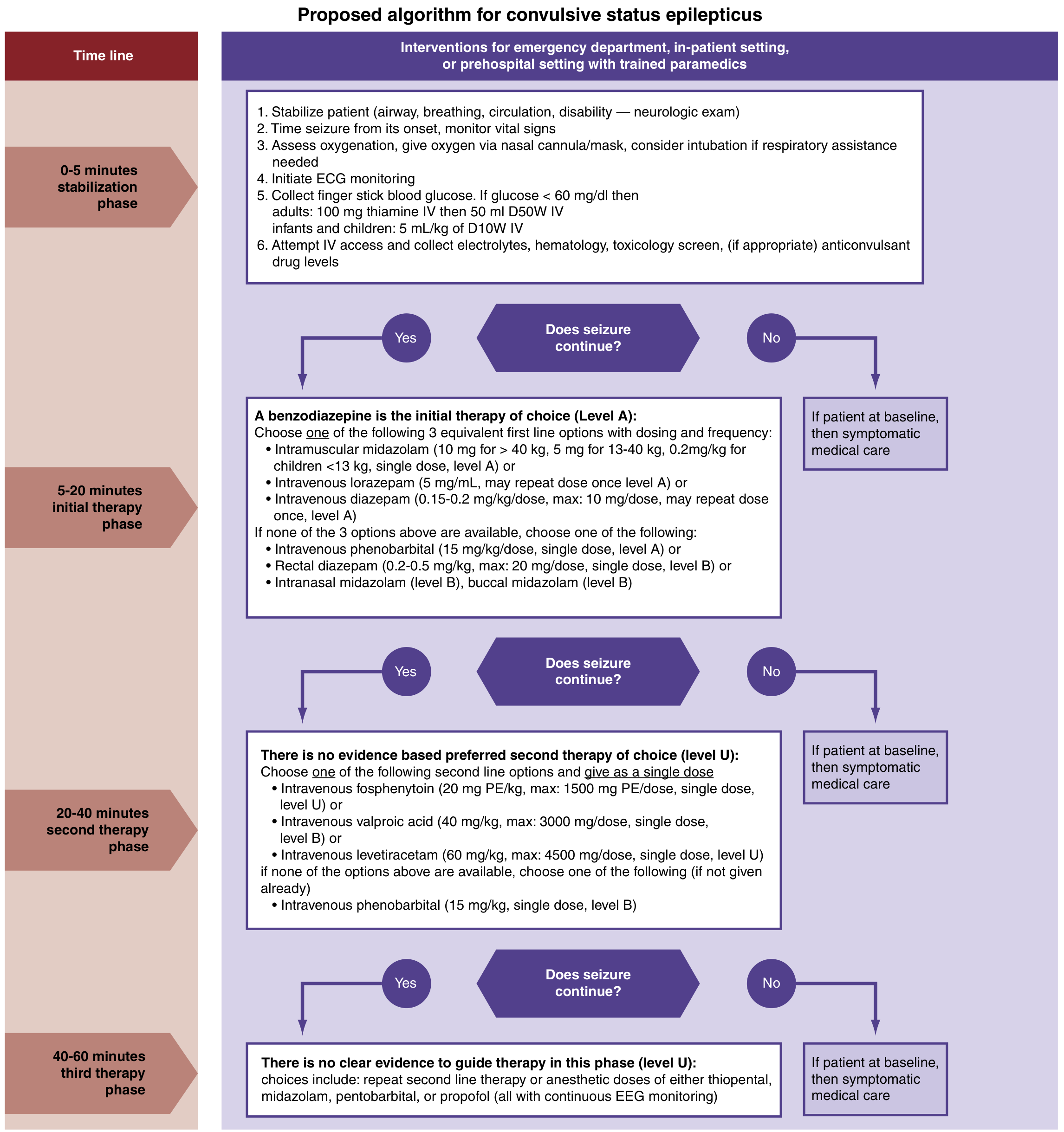
(Rosen's Emergency Medicine - Fig. 169.3, based on American Epilepsy Society Guidelines 2016)
Phase 1: Stabilization (0-5 minutes)
- ABCs + neurological exam
- Time the seizure from onset
- Oxygen, ECG monitoring
- Fingerstick glucose - if <60 mg/dL: D10W 5 mL/kg IV in infants/children
- IV/IO access + labs (electrolytes, hematology, toxicology, AED levels)
Phase 2: Initial Therapy (5-20 minutes) - Benzodiazepines (Level A)
Choose one of the following first-line options:
| Route | Drug | Dose |
|---|---|---|
| IM (preferred if no IV) | Midazolam | 10 mg for >40 kg; 5 mg for 13-40 kg; 0.2 mg/kg for <13 kg; single dose |
| IV | Lorazepam | 0.1 mg/kg IV (max 4 mg/dose); may repeat once |
| IV | Diazepam | 0.15-0.2 mg/kg/dose IV (max 10 mg/dose); may repeat once |
If IV/IO not available:
- Rectal diazepam: 0.2-0.5 mg/kg (max 20 mg/dose) - Level B
- Intranasal midazolam - Level B (0.2 mg/kg IN; shown superior to rectal diazepam with more rapid onset)
- Buccal midazolam - Level B
Diazepam pediatric IV dosing (Harriet Lane):
- Child 1 month-<5 years: 0.2-0.5 mg/dose IV Q2-5 min, max total 5 mg
- Child ≥5 years: 1 mg/dose IV Q2-5 min, max total 10 mg
Second benzodiazepine dose: give only after 5 minutes of continued activity following first dose
Benzodiazepines terminate seizures 70% of the time via rapid CNS diffusion.
Phase 3: Second-Line Therapy (20-40 minutes) - if seizure persists after 2 BZD doses
No single agent is proven superior (Level U evidence). Choose one:
| Drug | Dose | Notes |
|---|---|---|
| IV Levetiracetam | 60 mg/kg IV (max 4,500 mg), single dose | Preferred; fewer adverse effects than phenytoin; comparable efficacy |
| IV Fosphenytoin | 20 mg PE/kg IV (max 1,500 mg PE), single dose | Water-soluble; less cardiotoxic than phenytoin; can be given IM |
| IV Valproic acid | 40 mg/kg IV (max 3,000 mg), single dose | Level B; contraindicated in liver disease, thrombocytopenia, possible metabolic disease |
| IV Phenobarbital | 15 mg/kg IV, single dose | Level B; if others unavailable |
Fosphenytoin vs. Phenytoin: Fosphenytoin can be given 3x faster, is less cardiotoxic, less sclerosing, and can be given IM - preferred over phenytoin.
Phase 4: Third-Line / Refractory Status (40-60+ minutes)
- Refractory status epilepticus = failure of ≥2 adequate antiseizure drug doses
- Anesthetic doses with continuous EEG monitoring required:
- Midazolam infusion OR
- Propofol infusion (if intubated) OR
- Pentobarbital / Thiopental OR
- Ketamine (limited case-report evidence; may be effective vs. conventional anesthetics)
- Inhalant anesthetics
- All cause apnea, hypotension, and depressed consciousness - intubation and hemodynamic monitoring mandatory
- Consult neurology for refractory pediatric status epilepticus
6. Long-Term AED Selection by Seizure Type
(Adams and Victor's Principles of Neurology, 12th Ed. - Table 15-7)
| Seizure Type | First-Line | Second-Line | Third-Line |
|---|---|---|---|
| Generalized tonic-clonic | Valproate, Carbamazepine | Lamotrigine, Oxcarbazepine | Phenytoin |
| Myoclonic | Valproate, Levetiracetam | Lamotrigine | Phenobarbital, Clobazam |
| Absence | Valproate | Topiramate, Levetiracetam, Ethosuximide | Lamotrigine |
| Focal | Carbamazepine, Phenytoin | Valproate, Levetiracetam, Oxcarbazepine | Lamotrigine, Vigabatrin, Topiramate |
| Infantile spasms | ACTH, Vigabatrin, Valproate | Valproate | Lamotrigine |
| Lennox-Gastaut | Valproate | Topiramate, Lamotrigine | Levetiracetam |
Important genetic exceptions:
- Dravet syndrome (SCN1A mutation): Avoid lamotrigine - often worsens seizures
- Glucose transporter deficiency (SLC2A1): Responds to ketogenic diet
7. Breakthrough Seizures in Known Epilepsy
Common causes to check in the ED:
- Sub-therapeutic drug levels (child outgrew dose, vomiting, drug interactions, non-adherence) - check serum AED levels
- Febrile illness (lowers seizure threshold even with therapeutic levels)
- Sleep deprivation, stress
Management: Identify cause, consult neurologist for dose adjustment; LP not needed unless meningitis signs present.
8. Special Situations
Seizures with Trauma
- Benzodiazepines remain first-line for active seizure
- Load with fosphenytoin or levetiracetam (not diazepam alone) to prevent short-term recurrence that can worsen TBI and raise ICP
- "Impact seizures" (within minutes of injury) do not increase risk of intracranial injury by themselves - but delayed seizures suggest more severe injury
Abusive Head Trauma
- Suspect in infants <2 years with seizures and vague history; often no external injury
- Subdural hematoma is the most common inflicted intracranial injury
- Maintain high index of suspicion
VP Shunt Patients
- Consider: underlying epilepsy, shunt malfunction, CNS infection
- Shunt-related seizures with fever more likely infectious than mechanical
- Evaluate: shunt series X-ray + head CT for ventricular size; LP/shunt tap if infection suspected
9. Post-Seizure Workup
After seizure is controlled:
- Neuroimaging: indicated after status epilepticus or focal/complex seizures
- Lumbar puncture: if CNS infection suspected, or after status epilepticus without clear cause
- EEG: not needed after a first simple febrile seizure; required for refractory/nonconvulsive status (EEG is the only way to diagnose nonconvulsive SE)
- Intubation note: if RSI needed, use agents with antiepileptic activity (propofol, ketamine); prefer short-acting neuromuscular blocker (succinylcholine) to allow ongoing seizure monitoring
Sources:
- Harriet Lane Handbook, Johns Hopkins, 23rd Ed. - Febrile seizure classification & dosing
- Rosen's Emergency Medicine - Status epilepticus algorithm (American Epilepsy Society 2016)
- Tintinalli's Emergency Medicine, Comprehensive Study - Febrile seizures, epilepsy in children
- Adams and Victor's Principles of Neurology, 12th Ed. - AED choice by seizure type (Table 15-7)
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry - Pediatric epilepsy syndromes
- Textbook of Family Medicine, 9th Ed. - Status epilepticus, AED dosing table
This is a shared conversation. Sign in to Orris to start your own chat.