11th cranial nerve
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive, authoritative content. Here is the full answer:
Cranial Nerve XI - The Accessory Nerve (Spinal Accessory Nerve)
Fiber Type
CN XI is a purely motor nerve. It carries no sensory fibers (afferent proprioceptive information from its target muscles travels back via the cervical dorsal root ganglia, not within CN XI itself).
Anatomy and Components
The accessory nerve has two roots:
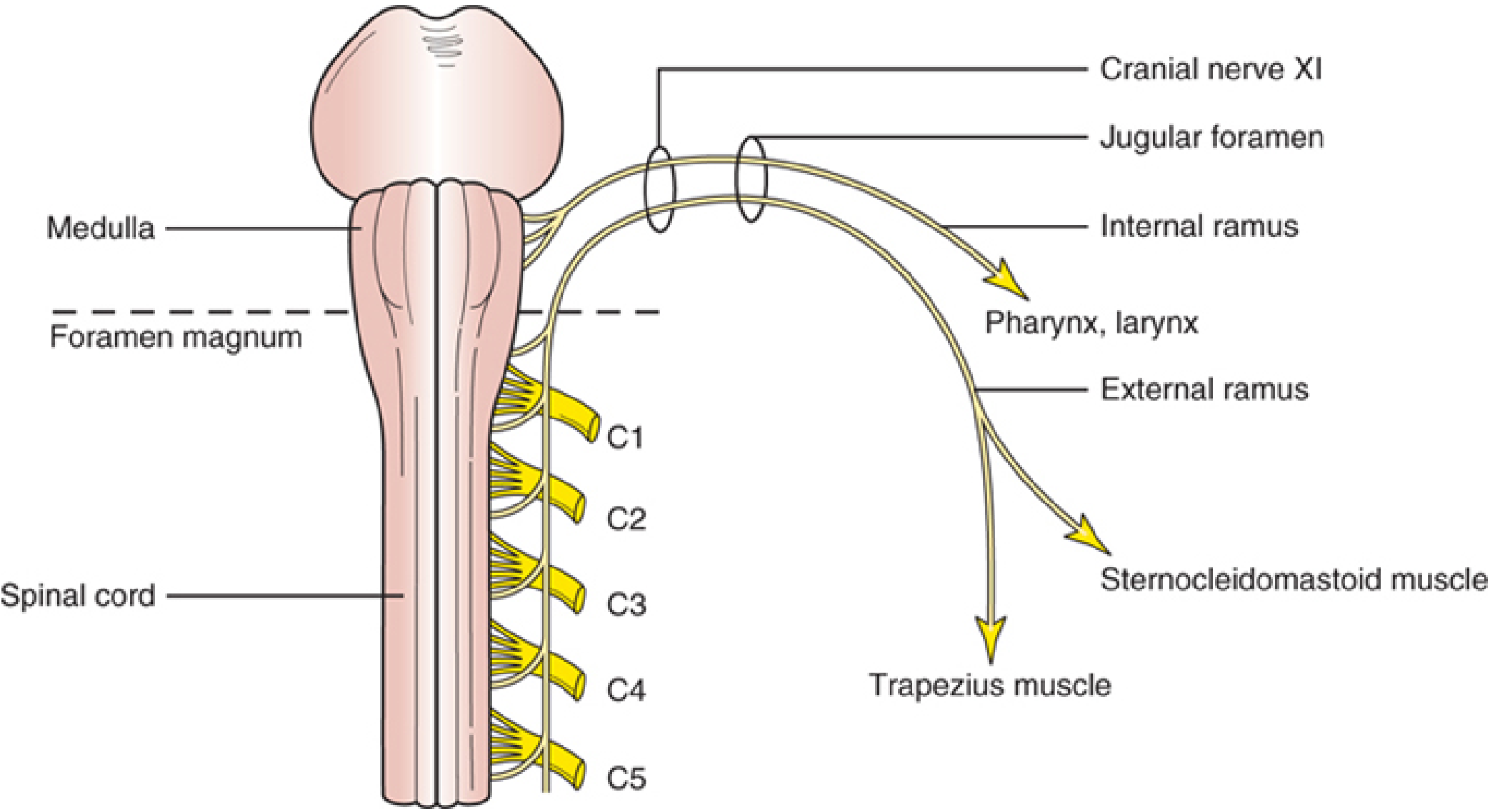
1. Cranial Root (Internal Ramus)
- Arises from cells in the caudal nucleus ambiguus of the medulla
- Emerges from the lateral medulla below the roots of the vagus nerve (CN X)
- After passing through the jugular foramen, branches off as the internal ramus and joins the vagus nerve to supply the pharynx and larynx
- (Note: some recent anatomical studies question the existence of this cranial branch, though a 2014 cadaver study confirmed it in the majority of humans)
2. Spinal Root (External Ramus)
- Arises from the spinal accessory nucleus - a column of cells in the dorsolateral ventral horn of the cervical cord from C1 to C6
- Somatotopic arrangement: C1-C2 innervate the ipsilateral sternocleidomastoid (SCM); C3-C4 innervate the ipsilateral trapezius
- Fibers pass through the lateral funiculus, exit between the dentate ligament and dorsal roots, ascend in the subarachnoid space, and enter the skull through the foramen magnum
Course and Exit
- The cranial and spinal roots unite and exit the cranium via the jugular foramen (together with CN IX and CN X)
- After exiting, the external (spinal) ramus enters the neck between the internal carotid artery and internal jugular vein
- It then penetrates and supplies the SCM, emerges near the middle of the posterior border of the SCM
- Crosses the posterior cervical triangle within the investing fascia to reach the trapezius, running on its deep surface
- In its course, it receives branches from C2, C3, and C4 cervical nerves
The superficial location of CN XI as it crosses the posterior triangle makes it susceptible to iatrogenic injury (e.g., lymph node biopsy) - Gray's Anatomy for Students
Muscles Innervated
| Muscle | Action Tested | How to Test |
|---|---|---|
| Sternocleidomastoid (SCM) | Ipsilateral neck flexion + contralateral head rotation | Ask patient to turn head to the opposite side against resistance; inspect and palpate the contracting muscle |
| Trapezius | Elevates, retracts, and rotates the scapula; assists arm elevation above horizontal | Ask patient to shrug shoulders against resistance; compare both sides |
Supranuclear (Cortical) Innervation
- The corticobulbar pathway for the trapezius is crossed - the left hemisphere controls the right trapezius
- The pathway for the SCM is thought to be ipsilateral (left hemisphere controls left SCM), possibly via a double decussation in the brainstem
- This is why in a left hemispheric stroke, the patient turns their head to the left (right SCM, ipsilateral to the lesion, is intact and unopposed)
- Corticobulbar fibers to the SCM are in the brainstem tegmentum; fibers to the trapezius are in the ventral brainstem - so a ventral pontine lesion can cause trapezius paresis with SCM sparing
Clinical Deficits of CN XI Palsy
Unilateral Spinal Accessory Nerve Palsy:
- SCM weakness: difficulty turning head to the contralateral side; on attempted flexion, the head deviates toward the unaffected side
- Trapezius weakness:
- Shoulder droops (lower on affected side at rest)
- Scapula displaced downward and laterally, with vertebral border slightly winged
- Inability to raise the arm above horizontal after abduction
- Shoulder shrug weakness
- Chronic injury leads to trapezius atrophy
Bilateral CN XI Palsy:
- Bilateral SCM: weakness of neck flexion, head falls backward on standing
- Bilateral trapezius: weakness of neck extension, head falls forward
Causes of CN XI Injury
| Level | Common Causes |
|---|---|
| Spinal accessory nucleus | ALS, intrinsic cord neoplasm, syrinx |
| Jugular foramen | Vernet syndrome (IX, X, XI), Villaret syndrome, Collet-Sicard syndrome; skull base tumors |
| Peripheral branches | Iatrogenic (most common - lymph node biopsy/dissection in neck cancer); trauma; neuralgic amyotrophy; cervical radiotherapy |
| Cervical dystonia treatment | Intentional ablation |
Key Mnemonics / High-Yield Points
- Exits via: Jugular foramen (along with CN IX and X)
- Spinal origin: C1-C6 anterior horn (ventrolateral)
- Targets: SCM + Trapezius (both ipsilateral)
- Pure motor nerve (no sensory component in the nerve itself)
- Most common injury site: Posterior triangle of the neck (superficial location)
- SCM action: rotates head to the opposite side - so right SCM weakness = difficulty turning left
Sources: Localization in Clinical Neurology, 8e | Gray's Anatomy for Students | Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.