Body temprature physilogy 10 marks question
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a thorough 10-mark answer. Here it is:
Body Temperature Physiology - 10 Marks
1. Normal Body Temperature
The body maintains two functionally distinct temperature zones:
- Core temperature (deep tissues - liver, brain, heart): maintained within a very narrow range of 36°C - 37.5°C (96.8°F - 99.5°F). Oral measurement averages 98.0-98.6°F; rectal is ~1°F higher.
- Skin temperature: varies freely with the environment and is important for heat transfer to surroundings.
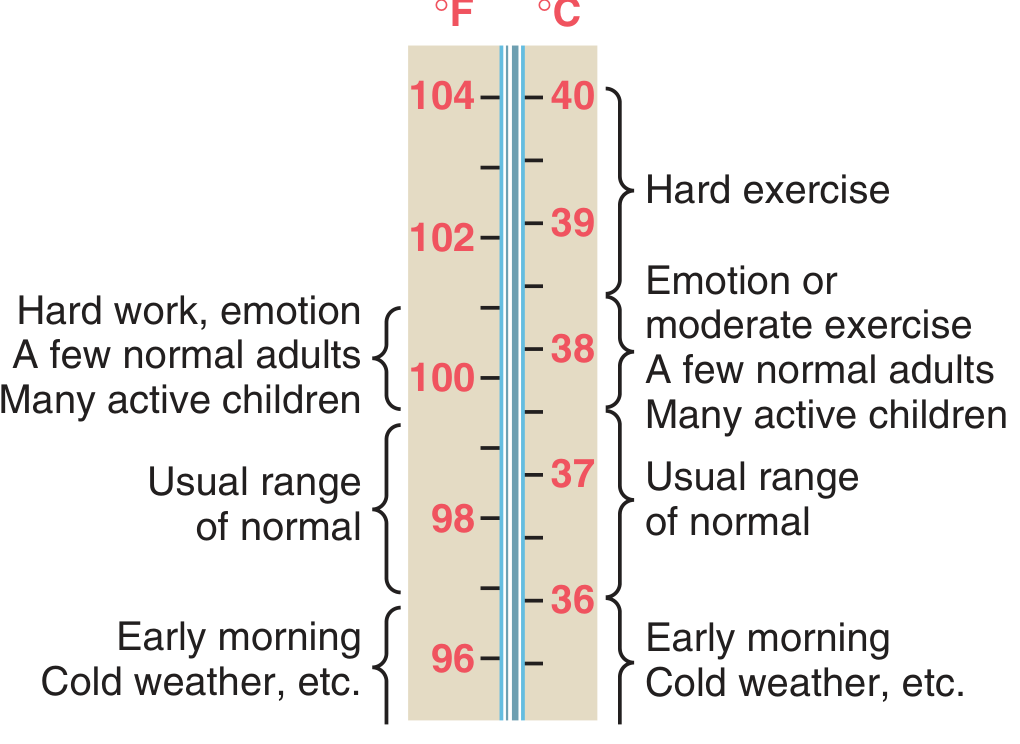
Temperature varies diurnally - lowest (~36°C) in early morning, highest (~37.5°C) in the afternoon. During strenuous exercise it can transiently reach 39-40°C.
2. Heat Balance Equation
Body temperature = Heat Production - Heat Loss
When heat production > heat loss → temperature rises.
When heat loss > heat production → temperature falls.
3. Heat Production
Sources of heat production (metabolic heat):
| Source | Mechanism |
|---|---|
| Basal metabolism | Ongoing cellular reactions |
| Muscle activity / Shivering | Major source; shivering can increase heat 3-5x |
| Thyroid hormones (T3/T4) | Increase cellular metabolic rate |
| Epinephrine / Norepinephrine | Sympathetic stimulation increases cellular metabolism |
| Thermogenic effect of food (SDA) | Especially protein digestion |
| Rising cell temperature | Q10 effect - chemical reactions speed up with heat |
- Guyton and Hall Textbook of Medical Physiology, p. 892
4. Heat Loss Mechanisms
Heat is lost from the body by four physical methods:
A. Radiation (~60%)
Emission of infrared electromagnetic waves from body surface to cooler surroundings. Does not require physical contact or medium.
B. Conduction (~3%)
Direct heat transfer by physical contact with cooler objects (e.g., a chair). Poor contributor under normal conditions since air is a poor conductor.
C. Convection
Transfer of heat by movement of air or water currents over the skin surface. Wind increases convective heat loss significantly.
D. Evaporation (~22-25%)
- Insensible perspiration: 600-700 mL/day evaporates from lungs and skin continuously. Cannot be controlled.
- Sweating (sensible perspiration): Controlled by the hypothalamus via sympathetic cholinergic fibers to eccrine sweat glands. At maximum activity, sweat rate can reach 1.5 L/hour. Each gram of water evaporated loses ~0.58 kcal of heat.
- Evaporation is the only effective mechanism when ambient temperature exceeds body temperature.
E. Role of Skin Blood Flow
Blood flow to skin varies from near-zero to 30% of cardiac output. Skin vasodilation (decreased sympathetic tone to arterioles + AV anastomoses) rapidly transfers heat from the core to the surface. Vasoconstriction retains heat. This ~8-fold variation in conductance makes skin an effective "controlled heat radiator."
- Guyton and Hall Textbook of Medical Physiology, pp. 892-895
5. Thermoregulatory Center - The Hypothalamus
The preoptic area of the anterior hypothalamus is the primary thermostat:
- Contains warm-sensitive neurons (fire when temperature rises → activate heat dissipation)
- Contains cold-sensitive neurons (fire when temperature falls → activate heat conservation)
- Receives input from: peripheral cutaneous receptors (especially cold receptors in skin), spinal cord thermoreceptors, deep tissue receptors, and intrinsic hypothalamic receptors - each contributing approximately 20% of the integrated signal (Ganong)
| Region | Function |
|---|---|
| Anterior hypothalamus | Detects warmth; activates heat dissipation (vasodilation, sweating) |
| Posterior hypothalamus | Integrates cold signals; activates heat conservation (shivering, vasoconstriction) |
Threshold temperatures (Ganong):
-
Sweating and vasodilation: 37°C
-
Vasoconstriction: 36.8°C
-
Non-shivering thermogenesis: 36°C
-
Shivering: 35.5°C
-
Ganong's Review of Medical Physiology, 26th Ed., p. 324
6. Responses to Cold (Heat Conservation & Production)
- Cutaneous vasoconstriction - sympathetic adrenergic activation constricts skin arterioles and AV anastomoses; diverts blood away from skin
- Shivering - involuntary rhythmic muscle contractions; can increase heat production 3-5 times above basal
- Non-shivering thermogenesis - epinephrine/norepinephrine increase cellular metabolism; important in neonates via brown adipose tissue (BAT)
- Thyroid hormone release - increases basal metabolic rate (longer-term adaptation)
- Countercurrent heat exchange - in limbs, warm arterial blood transfers heat to cold venous blood (venae comitantes), conserving core temperature
- Behavioral responses - huddling, adding clothing, seeking warmth
7. Responses to Heat (Heat Dissipation)
- Cutaneous vasodilation - decreased sympathetic tone; skin blood flow rises dramatically
- Sweating - sympathetic cholinergic fibers activate eccrine glands; primary heat-loss mechanism in hot conditions
- Behavioral responses - seeking shade, removing clothing, reducing activity
- Inhibition of shivering and non-shivering thermogenesis
8. Fever
Fever = resetting of the hypothalamic set-point to a higher level by pyrogens.
Mechanism:
Infection/tissue damage → bacterial endotoxins/exotoxins → phagocytosis by macrophages, monocytes, Kupffer cells → release of endogenous pyrogens (cytokines):
- IL-1β (the most important - also called leukocyte pyrogen)
- IL-6, TNF-α, IFN-β, IFN-γ
These cytokines act on the OVLT (organum vasculosum of the lamina terminalis - a circumventricular organ lacking a blood-brain barrier) → stimulates the preoptic hypothalamus → increased local prostaglandin E2 (PGE2) synthesis via cyclooxygenase (COX) → raises the thermostat set-point.
Course of Fever:
- Chill phase: new set-point is higher than current temperature → hypothalamus activates heat-conservation (vasoconstriction) and heat-production (shivering) → patient feels cold, shivers
- Plateau phase: body temperature reaches new set-point; balance between production and loss
- Defervescence (crisis/lysis): pyrogens removed → set-point returns to normal → body temperature now "too high" → hypothalamus activates sweating and vasodilation to dissipate heat
Antipyretics (e.g., Aspirin, NSAIDs):
Inhibit cyclooxygenase (COX) → block PGE2 synthesis → set-point returns to normal → fever breaks via sweating and vasodilation.
- Costanzo Physiology 7th Ed., p. [block 2]; Guyton & Hall, p. 900
9. Clinical Disturbances of Thermoregulation
| Condition | Mechanism | Features |
|---|---|---|
| Heat exhaustion | Excessive sweating → ECF/blood volume loss → decreased BP | Fainting, weakness, nausea |
| Heat stroke | Failure of sweating mechanism → core temp >40°C | Confusion, no sweating, organ damage |
| Hypothermia | Heat loss > production (cold exposure, anesthesia) | Core temp <35°C; cardiac arrhythmias, death |
| Malignant hyperthermia | Massive uncontrolled skeletal muscle metabolism (inhalation anesthetics in susceptible individuals) | Extreme hyperthermia, rigidity, rhabdomyolysis |
Summary Table
| Stimulus | Effector Response | Mediator |
|---|---|---|
| Cold | Vasoconstriction | Sympathetic adrenergic |
| Cold | Shivering | Somatic motor (posterior hypothalamus) |
| Cold | Brown fat thermogenesis | Epinephrine/NE |
| Heat | Vasodilation | Decreased sympathetic tone |
| Heat | Sweating | Sympathetic cholinergic |
| Pyrogens | Fever (set-point rise) | IL-1 → PGE2 → hypothalamus |
Sources: Guyton and Hall Textbook of Medical Physiology (Ch. 74) | Costanzo Physiology 7th Ed. | Ganong's Review of Medical Physiology 26th Ed.
Body temprateure all question answer from 10 years pyq answer 10 marks
Asking for Preferences
Searching the Web
MBBS 1st year physiology body temperature regulation 10 marks PYQ past year questions India university 10 years
Finding Sources
Searching the Web
MBBS 1st year physiology body temperature PYQ "10 marks" "heat stroke" "fever mechanism" "shivering" university exam questions
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading Web Page
https://medical.iqcity.in/wp-content/uploads/2021/03/1st-Pro…
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have all the material needed. Let me compile the complete PYQ-style answer set.
Body Temperature Physiology - MBBS 1st Year PYQ Answers (10 Marks Each)
Based on the most commonly repeated questions across Indian university exams (MUHS, RGUHS, NTRUHS, BFUHS, etc.) over the past 10 years, here are complete model answers:
⭐ PYQ 1 - Most Repeated (Almost Every Year)
"Describe the regulation of body temperature. Add a note on fever." [10 marks]
Also asked as: "Role of hypothalamus in temperature regulation" / "Heat balance and regulation of body temperature"
Definition & Normal Values
- Core temperature: 36°C - 37.5°C (oral avg = 98.6°F / 37°C; rectal = 0.5°C higher)
- Skin temperature: varies with environment
- Diurnal variation: lowest at 6 AM (~36°C), highest at 6 PM (~37.5°C)
- Core temperature = Heat produced - Heat lost
I. HEAT PRODUCTION (Sources)
| Factor | Mechanism |
|---|---|
| Basal metabolism | Ongoing cellular oxidative reactions |
| Muscle activity / Shivering | Can increase heat 3-5x above basal |
| Thyroid hormones (T3/T4) | Increase cellular metabolic rate (calorigenic effect) |
| Epinephrine / NE / Sympathetic stimulation | Uncouples oxidative phosphorylation |
| Specific Dynamic Action of food | Protein > Fat > CHO |
| Brown adipose tissue (BAT) | Non-shivering thermogenesis (neonates) |
| Q10 effect | Rising cell temperature increases chemical reaction rates |
II. HEAT LOSS MECHANISMS
| Mechanism | % Total Loss | Description |
|---|---|---|
| Radiation | ~60% | Infrared waves emitted from skin to cooler surroundings; no contact needed |
| Evaporation | ~22-25% | Sweating (sensible) + insensible perspiration (600-700 mL/day from skin + lungs) |
| Conduction | ~3% | Direct contact with cooler object; air is a poor conductor |
| Convection | ~15% | Air/water currents carry heat away; wind increases this greatly |
Key point: When ambient temperature > body temperature, evaporation is the ONLY effective mechanism. This is why humidity impairs heat loss.
Insulator System: Skin + subcutaneous fat acts as insulator. Fat conducts heat 1/3rd as readily as other tissues. Blood flow to skin varies from near-zero to 30% of cardiac output (8-fold variation), making skin a controlled "heat radiator."
III. THERMOREGULATORY CENTER - HYPOTHALAMUS
The preoptic area of the anterior hypothalamus is the master thermostat.
Afferents (inputs - each ~20%):
- Peripheral cutaneous cold/warm receptors (skin)
- Spinal cord thermoreceptors
- Deep tissue receptors
- Extrahypothalamic brain receptors
- Intrinsic hypothalamic thermosensitive neurons
| Region | Function |
|---|---|
| Anterior hypothalamus (preoptic area) | Detects warmth → activates heat dissipation (vasodilation, sweating) |
| Posterior hypothalamus | Integrates cold signals → activates heat conservation (shivering, vasoconstriction) |
Threshold temperatures (Ganong):
- Vasodilation + sweating onset: 37°C
- Vasoconstriction onset: 36.8°C
- Non-shivering thermogenesis: 36°C
- Shivering onset: 35.5°C
IV. RESPONSES TO COLD (Heat Conservation)
- Cutaneous vasoconstriction - sympathetic adrenergic activation; diverts blood from skin to core
- Shivering - involuntary rhythmic skeletal muscle contractions; increases heat production 3-5x; controlled by posterior hypothalamus
- Non-shivering thermogenesis - epinephrine/NE release → uncoupling of oxidative phosphorylation, especially in BAT (important in neonates)
- Thyroid hormone release - long-term increase in BMR (acclimatization)
- Countercurrent heat exchange - deep veins (venae comitantes) run alongside arteries in limbs; warm arterial blood transfers heat to cold venous blood, conserving core temperature
- Behavioral - seeking warmth, adding clothing, curling up
V. RESPONSES TO HEAT (Heat Dissipation)
- Cutaneous vasodilation - decreased sympathetic tone; AV anastomoses open; skin blood flow → up to 30% cardiac output
- Sweating - sympathetic cholinergic fibers → eccrine sweat glands; max rate ~1.5 L/hour; each gram evaporated = 0.58 kcal heat lost
- Inhibition of shivering and thermogenesis
- Behavioral - removing clothing, reducing activity, seeking shade
Mechanism of sweating: Cholinergic sympathetic nerve → ACh → eccrine gland → primary secretion (plasma-like, no proteins) → duct reabsorbs Na⁺/Cl⁻ → final sweat is hypotonic. Can also be triggered by circulating epinephrine during exercise.
VI. FEVER
Definition: Controlled hyperthermia due to resetting of hypothalamic set-point upward by pyrogens.
Pathogenesis:
Infection/Tissue damage
↓
Exogenous pyrogens (endotoxins, LPS, viral antigens)
↓
Phagocytosis by Macrophages, Monocytes, Kupffer cells
↓
Release of Endogenous Pyrogens (Cytokines):
• IL-1β (most important - "leukocyte pyrogen")
• IL-6
• TNF-α
• IFN-β, IFN-γ
↓
Act on OVLT (Organum Vasculosum of Lamina Terminalis)
[circumventricular organ - lacks BBB]
↓
Stimulate Preoptic Hypothalamus
↓
↑ Arachidonic acid → ↑ COX → ↑ Prostaglandin E2 (PGE2)
↓
SET-POINT RAISED above 37°C
Stages of Fever:
| Stage | What Happens | Patient Feels |
|---|---|---|
| Chill phase (Rigor) | Set-point now higher than body temp → hypothalamus activates vasoconstriction + shivering to raise temp | Cold, shivers, "chills" |
| Plateau phase | Body temp = new set-point; balanced heat production/loss | Hot, flushed |
| Defervescence (Crisis/Lysis) | Pyrogens removed → set-point returns to 37°C → body temp "too high" → sweating + vasodilation | Sweating profusely |
Antipyretics (Aspirin/NSAIDs): Inhibit COX enzyme → block PGE2 synthesis → set-point falls back to normal → fever breaks by sweating + vasodilation.
(Source: Guyton & Hall Textbook of Medical Physiology; Costanzo Physiology 7th Ed.)
⭐ PYQ 2 - Frequently Asked
"Describe the mechanisms of heat loss from the body." [10 marks]
Also: "Enumerate heat loss mechanisms and explain each" / "How does the body maintain temperature in a hot environment?"
Refer to Section II + V above (Radiation, Conduction, Convection, Evaporation + Skin blood flow + Sweating)
Additional points for this specific question:
Insensible water loss:
- Skin: ~300-400 mL/day (diffusion, cannot be controlled)
- Lungs: ~300-400 mL/day (expired air is saturated at 37°C)
- Total insensible loss: 600-700 mL/day
Sweating vs. Insensible perspiration:
| Feature | Insensible Perspiration | Sweating |
|---|---|---|
| Control | Uncontrolled | Controlled by hypothalamus |
| Amount | 600-700 mL/day | Up to 1.5 L/hour |
| Composition | Pure water | Hypotonic NaCl solution + urea, lactic acid |
| Innervation | None | Sympathetic cholinergic |
Role of clothing: Clothing traps a layer of warm air → reduces convection and radiation. Light-colored clothing reflects radiant heat.
⭐ PYQ 3 - Common Short/Long Note
"Write a note on Heat Stroke and Heat Exhaustion." [10 marks]
Also asked as: "Differentiate heat exhaustion from heat stroke" / "Clinical disorders of temperature regulation"
Heat Illnesses Classification (Park's Textbook)
| Feature | Heat Stroke | Heat Exhaustion | Heat Cramps | Heat Syncope |
|---|---|---|---|---|
| Core temp | >40°C (104°F) | Normal or slightly raised (<39°C) | Normal | Normal |
| Sweating | ABSENT (anhidrosis) | Present (profuse) | Present | Present |
| Thermoregulation | FAILED | Intact | Intact | Intact |
| Cause | Failure of heat-dissipation mechanisms | Hypovolemia from excessive sweating (water/salt depletion) | Loss of NaCl in sweat | Blood pooling in lower limbs |
| Consciousness | Altered/coma | Preserved | Preserved | Brief loss |
| Mortality | 40%+ if untreated | Low | Very low | Very low |
Heat Stroke - Details
Definition: Core temperature >40°C with CNS dysfunction and anhidrosis due to complete failure of thermoregulation.
Types:
- Classic heat stroke: Elderly, sedentary, during heat waves; not due to exertion
- Exertional heat stroke: Young athletes/military; vigorous exercise in hot humid conditions
Pathophysiology:
- Extreme rise in temp → positive feedback loop begins at ~41°C
- Hypothalamus itself damaged by heat → thermoregulation fails
- Multiorgan dysfunction: rhabdomyolysis, DIC, renal failure, hepatic failure
Treatment:
- Rapidly cool body in ice-water bath until rectal temp falls below 38.9°C (102°F)
- Monitor rectal temperature continuously
- Supportive: treat hypovolemia, hyperkalemia, rhabdomyolysis, hypocalcemia
Heat Exhaustion - Details
Pathophysiology:
- Prolonged heat + sweating → loss of water and electrolytes → ECF/blood volume ↓ → BP ↓ → cardiovascular failure
- Heat-dissipating mechanisms (sweating) are still functional
- Spontaneously resolves if the victim can rehydrate
Features: Dizziness, weakness, fatigue, pallor, cool moist skin, normal or slightly raised temp
Treatment: Rest in cool place, oral/IV fluids and electrolyte replacement
Heat Cramps
- Painful spasmodic contractions of skeletal muscles during heavy work in heat
- Cause: Loss of sodium and chloride in sweat
- Treatment: Salt and water replacement
⭐ PYQ 4 - Frequently Asked (5-10 marks)
"Write a note on Hypothermia." [5-10 marks]
Definition: Core body temperature below 35°C (95°F)
Causes: Prolonged cold exposure, wet/inadequate clothing, alcohol (causes vasodilation), anesthesia, hypothyroidism
Stages:
| Core Temp | Effects |
|---|---|
| 35-32°C | Shivering, tachycardia, hypertension, confusion |
| 32-28°C | Shivering stops (at ~30-32°C); bradycardia, atrial fibrillation, loss of consciousness |
| <28°C | Ventricular fibrillation |
| ~21°C | Cardiac arrest, death |
Pathophysiology of cold injury (Frostbite):
- Direct effects: Crystallization of intra/extracellular water → disruption of plasma membranes
- Indirect effects: Slow chilling → vasoconstriction + increased capillary permeability → edema → nerve damage → gangrene. Rapid chilling → vascular injury + increased blood viscosity → ischemia → infarction
Treatment: Gradual rewarming, prevent further heat loss. Do NOT rub frostbitten areas.
⭐ PYQ 5 - Explain Why / Short Note
"Why does sweating not cool the body in humid conditions?" / "Role of humidity in heat regulation"
- Heat loss by evaporation depends on the vapor pressure gradient between sweat on skin and surrounding air
- In high humidity, air is already saturated with water vapor → vapor pressure gradient is minimal → sweat cannot evaporate efficiently
- Sweat drips off instead of evaporating → no cooling effect
- Body continues to sweat → progressive dehydration without effective temperature control
- This is why humid heat is more dangerous than dry heat at the same temperature
⭐ PYQ 6 - Short Note
"Write a note on Acclimatization to heat." [5 marks]
After 1-2 weeks in a hot climate:
| Change | Significance |
|---|---|
| Sweating begins at a lower core temp | Earlier activation of cooling |
| Increased sweat volume (up to 3x) | More heat loss |
| Reduced NaCl concentration in sweat | Aldosterone-mediated Na⁺ conservation; prevents heat cramps |
| Increased plasma volume | Maintains cardiovascular performance |
| Lower heart rate at same workload | Improved efficiency |
| Earlier vasodilation | Improved skin blood flow |
- Mechanism: aldosterone (from adrenal cortex) is secreted in response to Na⁺ loss in sweat → increases reabsorption of Na⁺ in sweat ducts
- Unacclimatized persons need extra salt in first 10 days only
Quick Revision Table - All Key Points
| Topic | Key Fact |
|---|---|
| Normal core temp | 36-37.5°C; oral 98.6°F |
| Thermostat location | Preoptic area, anterior hypothalamus |
| Cold center | Posterior hypothalamus |
| Main heat loss at rest | Radiation (~60%) |
| Only mechanism when ambient temp > body temp | Evaporation |
| Sweating innervation | Sympathetic cholinergic |
| Shivering increases heat by | 3-5x |
| Key endogenous pyrogen | IL-1β |
| Pyrogen acts via | PGE2 (COX pathway) |
| Aspirin works by | COX inhibition → ↓ PGE2 |
| Heat stroke hallmark | Anhidrosis + hyperthermia + CNS dysfunction |
| Heat exhaustion cause | Hypovolemia (sweating intact) |
| Shivering stops at | ~30-32°C |
| Death by cardiac arrest | ~21°C |
Sources: Guyton and Hall Textbook of Medical Physiology (Ch. 74) | Costanzo Physiology 7th Ed. | Ganong's Review of Medical Physiology 26th Ed. | Park's Textbook of Preventive & Social Medicine | Robbins & Kumar Basic Pathology
This is a shared conversation. Sign in to Orris to start your own chat.