Teach me Meniningiomyocele like a neonataologist/ paeditrician in depth
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Searching PubMed
myelomeningocele neonatal management outcomes
I now have comprehensive material from multiple authoritative textbooks. Let me compile everything into a thorough, neonatologist/paediatrician-oriented teaching document.
Myelomeningocele (Meningomyelocele) - A Neonatologist's Deep Dive
Terminology note: The terms myelomeningocele (MMC) and meningomyelocele are used interchangeably. "Myelomeningocele" is the preferred modern term. It is a subset of open spina bifida and the most severe common form of neural tube defect (NTD) compatible with life.
1. The Anatomy - What Exactly Is It?
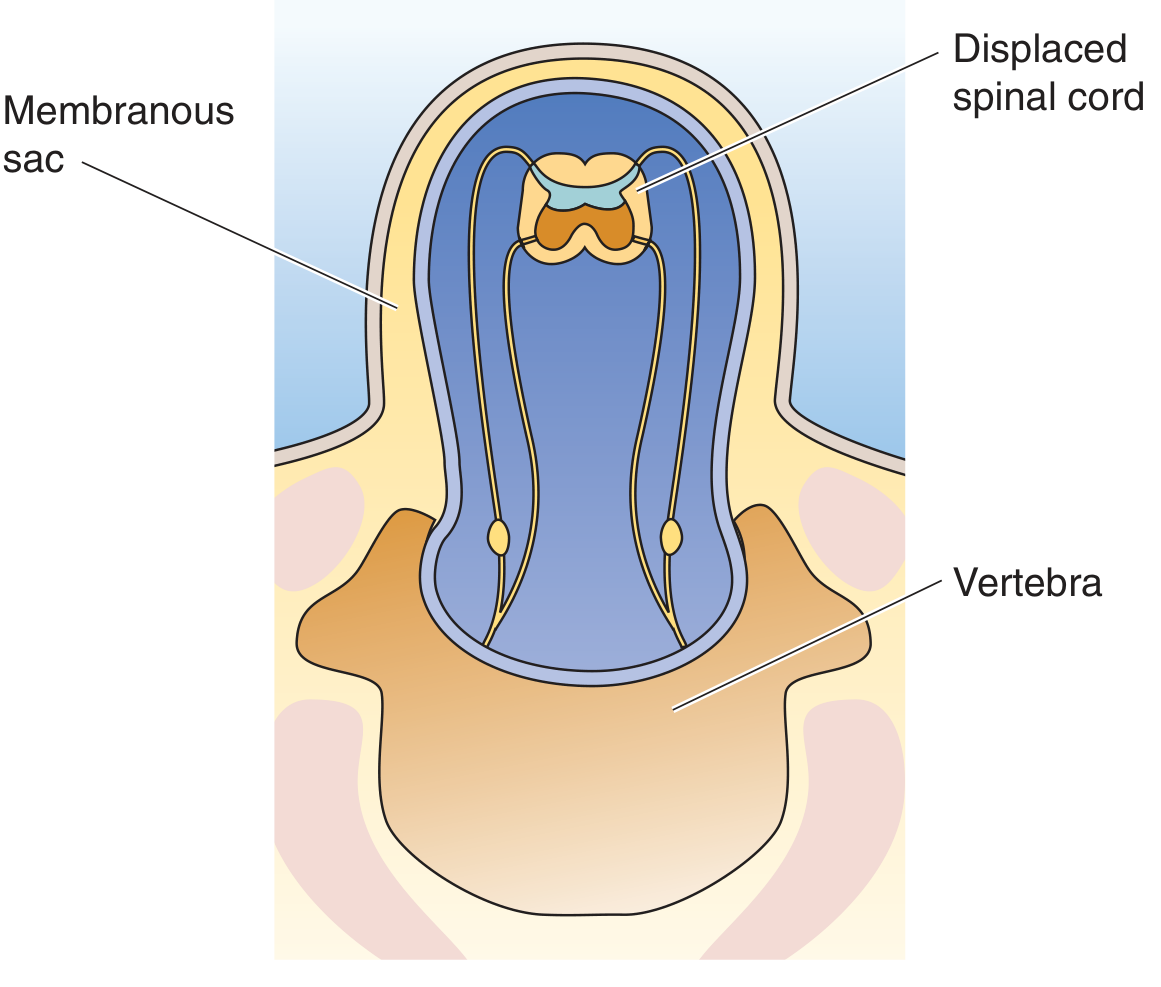
Cross-section showing the displaced spinal cord and nerve roots herniated into the membranous sac through the unfused vertebral arch (Medical Physiology, Fig. 10-7C)
Understand the spectrum first:
| Type | What herniates | Neural elements? | Neurological deficit |
|---|---|---|---|
| Spina bifida occulta | Nothing - vertebral arch unfused only | No | Usually none |
| Meningocele | Meninges + CSF only | No | Usually none |
| Myelomeningocele | Meninges + spinal cord + nerve roots | Yes | Always present |
| Myeloschisis | Open spinal cord, no sac - exposed neural plate | Yes | Severe |
In MMC, the spinal cord itself (the placode) lies within or at the surface of the sac. The neural tissue is directly exposed to amniotic fluid - this is critical to understanding why postnatal (or prenatal) closure is urgent.
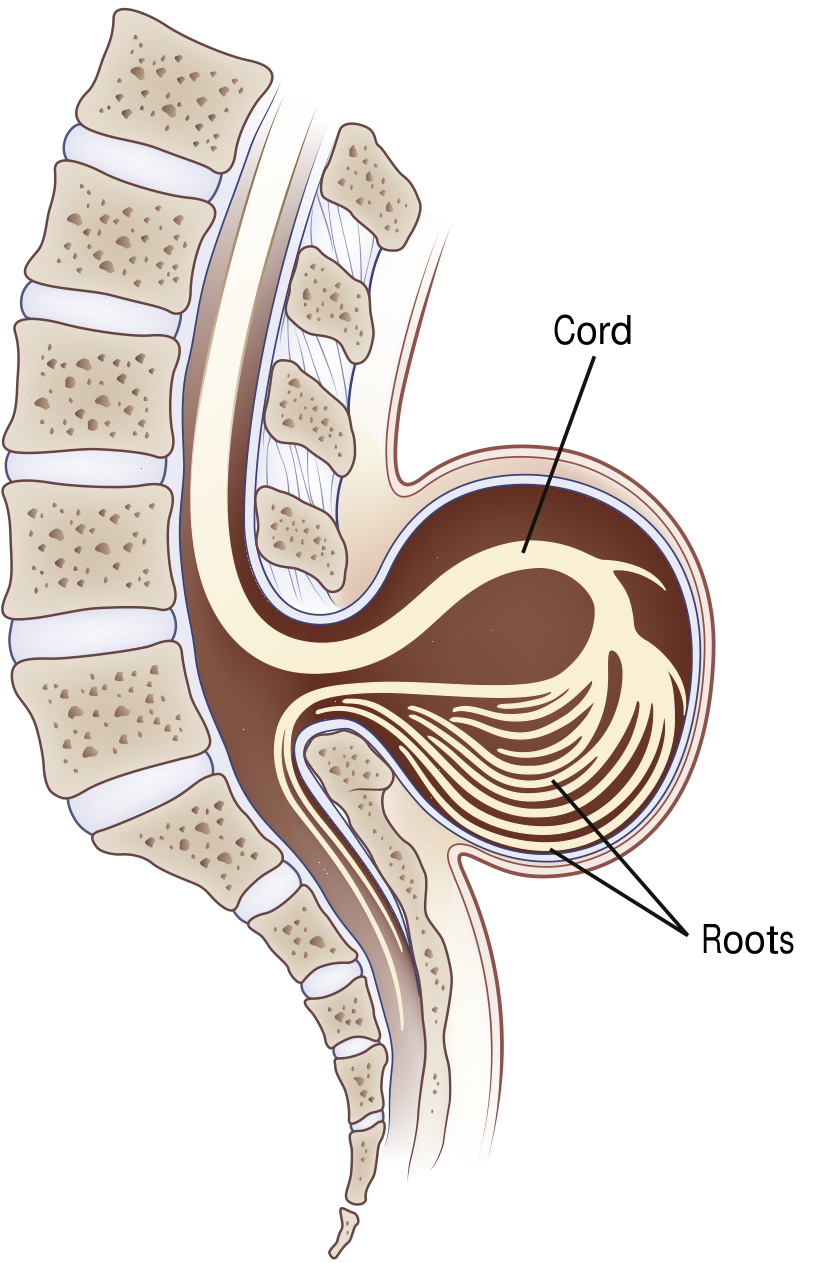
Sagittal view of myelomeningocele showing the cord and roots descending into the sac (Bradley & Daroff's Neurology, Fig. 104.10)
2. Embryology - Why Does It Happen?
Timeline: Weeks 3-4 of gestation (days 18-28). This is before most women know they are pregnant.
The neural plate folds to form the neural tube through a process called primary neurulation. Failure of this closure - specifically the caudal neuropore (which closes last, around day 26-28) - results in open defects at lumbar/sacral levels.
Two-hit hypothesis (Creasy & Resnik MFM, 2022):
- First hit: Primary failure of neural tube closure at ~week 4
- Second hit: Progressive damage from chronic exposure of the open neural placode to neurotoxic amniotic fluid throughout gestation - amniotic fluid contains substances directly toxic to neural tissue, and there is also mechanical trauma
This two-hit model is the entire rationale for in utero surgery - closing the defect early stops the second hit.
3. Epidemiology
- Incidence: approximately 1 in 3,000 live births (post-folate supplementation era)
- Folate supplementation has reduced MMC prevalence by ~50%, but a plateau has been reached
- 25-40% of MMC pregnancies are terminated following prenatal diagnosis
- Most common in lumbar and sacral regions (>75% of cases)
- Slight female predominance
Risk factors:
- Maternal folate/B12 deficiency (most important modifiable factor)
- Valproic acid during early pregnancy (1-2% risk of NTD - one of the highest teratogen risks known)
- Carbamazepine
- Family history of NTDs
- Prior affected pregnancy
- Maternal obesity, diabetes, hyperthermia in early pregnancy
4. Prenatal Diagnosis
Screening:
- Maternal serum AFP (MSAFP) at 14-16 weeks - elevated in ~85% of open NTDs. Open defects leak AFP into amniotic fluid then into maternal blood.
- Amniotic fluid AFP + acetylcholinesterase (more specific than AFP alone)
- Second-trimester ultrasound (18-20 weeks): Detects >90% of NTDs
Ultrasound signs - the classic triad:
| Sign | What you see | Significance |
|---|---|---|
| Lemon sign | Frontal bone scalloping (skull looks like a lemon) | Chiari II pulling on brain |
| Banana sign | Curved cerebellum wrapping around brainstem | Chiari II herniation |
| Splayed vertebrae | U-shaped or V-shaped vertebrae on axial view | Direct sign of spina bifida |
Fetal MRI at 19-25 weeks provides superior characterization of the lesion level, hindbrain herniation, and cortical anomalies.
5. Associated Anomalies - What Else to Look For
Chiari II Malformation (THE most important associated anomaly)
Present in virtually 100% of MMC cases. The downward traction of the tethered cord pulls the hindbrain through the foramen magnum:
- Cerebellar vermis + caudal brainstem (medulla, sometimes pons) herniate through enlarged foramen magnum
- Small posterior fossa
- Kinked medulla
- Polymicrogyria can be seen
Clinical consequences of Chiari II in neonates/infants:
- Stridor (inspiratory) - from vocal cord palsy due to cranial nerve X dysfunction
- Apnea - central (brainstem compression) or obstructive
- Swallowing dysfunction - aspiration risk
- Central hypoventilation - life-threatening
- Opisthotonus in severe cases
- These symptoms = brainstem dysfunction = 35% mortality by 5 years even with repair
Hydrocephalus
- Present in 64-85% of MMC cases requiring VP shunt (lumbosacral lesions)
- Mechanism: obstruction of CSF flow at the fourth ventricle due to Chiari II malformation
- Higher lesion level = higher risk of shunt-dependent hydrocephalus
- Mean IQ with VP shunt: ~80 (low normal); lower than those who don't require a shunt
- Monitor for shunt malfunction throughout childhood
Other associations:
- Tethered cord syndrome - progressive neurological deterioration post-repair as cord gets re-tethered
- Latex allergy - critically important. Children with MMC have a dramatically higher prevalence (10-40%) of latex allergy from repeated early latex exposure during multiple procedures. Strict latex-free environment from day 1.
- Craniolacunia (Lückenschädel) - depressed non-ossified areas on inner calvaria
- Syringomyelia
- Orthopedic deformities (hip dislocation, clubfoot, scoliosis, kyphosis)
- Neurogenic bladder and bowel
6. The Lesion Level - Functional Anatomy for Neonatologists
The motor level predicts functional ability. In MMC, the functional level is often better than the anatomic level.
| Lesion Level | Motor Function Preserved | Ambulation Potential | Bladder/Bowel |
|---|---|---|---|
| Thoracic | Arms, trunk partially | Wheelchair-dependent | Neurogenic |
| L1-L2 | Hip flexors (iliopsoas) | Braces + wheelchair | Neurogenic |
| L3-L4 | Knee extensors (quads) | May walk with braces | Neurogenic |
| L4-L5 | Ankle dorsiflexors, knee flexors | Walk with AFOs | Neurogenic (partial) |
| Sacral | Intrinsic foot muscles | Independent walking | Variable |
Key point for neonatologists: Almost ALL patients with MMC have neurogenic bladder regardless of lesion level, due to involvement of sacral roots. This means:
- Urinary retention with overflow incontinence if untreated
- Risk of upper urinary tract damage (hydronephrosis, reflux, renal failure)
- Clean intermittent catheterization (CIC) must be started early - often within days of birth
- Baseline renal ultrasound and urodynamics in first weeks of life
7. Neonatal Presentation and Initial Assessment
At Delivery - What You See
The neonate is born with a visible posterior midline mass, most commonly in the lumbosacral region:
- Intact sac: Translucent membrane covered sac containing CSF, meninges, and neural tissue - relatively protected
- Ruptured/exposed placode: Raw, red, weeping area - urgent surgical priority (meningitis risk)
- Look for motor posturing of lower limbs (flaccid = bad)
Neurological Examination in the Delivery Room
| What to assess | How | What it tells you |
|---|---|---|
| Spontaneous leg movement | Observe | Level of function |
| Response to pin-prick on lower limbs | Careful dermatomal testing | Sensory level |
| Anal wink reflex | Perianal stimulation | Sacral root integrity |
| Tone of lower limbs | Passive movement | LMN injury pattern |
| Head circumference | OFC measurement | Pre-existing hydrocephalus |
| Fontanelle tension | Palpation | ICP |
| Respiratory pattern | Observe | Brainstem function |
| Cry/voice quality | Listen | Vocal cord palsy |
Immediate Neonatal Orders (First Hour)
- Positioning: Prone or lateral decubitus - never supine over the sac. Place on a "doughnut" (ring pad) to protect the sac.
- Sterile moist saline gauze over the defect (non-adherent) - prevents desiccation and infection
- Latex-free environment immediately - use only latex-free gloves, equipment
- Thermoregulation: High insensible losses from the exposed defect - prone to hypothermia and heat loss. Incubator.
- Fluid management: Increase maintenance fluids to account for insensible losses from the sac
- IV access - anticipate early surgery
- Cranial ultrasound - assess ventricular size, rule out acute hydrocephalus
- Renal ultrasound - baseline upper tract
- Neurosurgical consultation - within hours for surgical planning
- Urology consultation - for bladder management plan
8. Timing and Type of Repair
Postnatal Repair
- Standard of care for decades
- Goal: Close within 24-72 hours of birth (reduces meningitis risk, though exact timing evidence varies)
- Rationale for urgency: open defect = direct route for ascending infection; CSF leak
- Surgical steps: separation of placode from surrounding skin, dural closure, fascial closure, skin closure
- Anesthesia considerations: prone positioning for intubation (doughnut under the sac), risk of brainstem herniation on induction, anticipate significant insensible fluid loss, vocal cord palsy risk
In Utero (Fetal) Repair - The MOMS Trial Revolution
The landmark Management of Myelomeningocele Study (MOMS Trial) was a randomized controlled trial (2003-2010, n=183) comparing prenatal open fetal repair vs. standard postnatal repair:
Benefits of prenatal repair (at 30 months):
- Reduced need for VP shunt placement before 1 year (40% vs 82%)
- Reversal of hindbrain herniation (Chiari II improvement)
- Better lower extremity motor function: 44.8% vs 23.9% walked independently
- Function ≥2 levels better than anatomic level: 26.4% vs 11.4%
- Better Bayley Mental Development Index scores
- Better Peabody Motor Scale scores
Costs of prenatal repair:
- Higher risk of preterm birth, preterm PROM
- Uterine dehiscence at delivery (11%)
- Maternal hysterotomy scar (affects future pregnancies - cesarean delivery required)
- Two perinatal deaths in each group
Window for fetal surgery: 19-26 weeks' gestation
Current eligibility criteria (strict patient selection):
- Singleton pregnancy
- MMC between T1 and S1 with hindbrain herniation
- Gestational age 19-25+6 weeks at evaluation
- Normal chromosomes
- No other major fetal anomalies
- No maternal contraindications
Fetoscopic (minimally invasive) repair is increasingly explored but remains associated with higher PPROM rates (91% vs 36%) and CSF leak from repair site, though it allows potential vaginal delivery.
Recent 2025 meta-analysis (PMID: 40492626) and comparative systematic review (PMID: 40779058) continue to compare open vs fetoscopic approaches, with open fetal surgery remaining the reference standard.
9. Postoperative Neonatal Care
After surgical closure (whether 24 hours or day 3 of life):
Immediate post-op:
- Positioning: Still prone for 5-7 days to allow wound healing; avoid pressure on repair
- Monitor for hydrocephalus: Head circumference daily; serial cranial ultrasounds; fontanelle examination. May develop or worsen post-repair as CSF dynamics change.
- VP shunt decision: Most will need a shunt (64-85% of lumbosacral MMC). Usually placed days to weeks after closure.
- Wound care: Monitor for CSF leak at repair site, infection
- Ventilatory monitoring: Apnea, central hypoventilation from Chiari II - may require prolonged monitoring, some require home apnea monitor
- Feeding: Assess swallow function before oral feeds - risk of aspiration with Chiari II-related bulbar dysfunction. NG feeds initially.
- Bladder management: Initiate CIC as soon as urology clears (typically within days)
Ongoing monitoring before discharge:
- Ophthalmology: strabismus, papilledema
- Audiology: sensorineural hearing loss can be associated
- Neurodevelopmental team engagement
- Social work / family counseling
10. Long-Term Complications and Follow-up (The Lifespan Perspective)
As a neonatologist, you are launching a child into a life of multidisciplinary care. Understand what's ahead:
| System | Problem | When |
|---|---|---|
| CNS | Shunt malfunction/infection | Anytime |
| CNS | Tethered cord syndrome (progressive deficits) | Childhood, adolescence |
| CNS | Syringomyelia | Any age |
| Urological | Neurogenic bladder, UTIs, vesicoureteral reflux, CKD | Lifelong |
| Orthopedic | Scoliosis, kyphosis, hip dislocation, clubfoot, pressure ulcers | Childhood onwards |
| Cognitive | Learning disabilities, executive function deficits, attention problems | School age |
| Skin | Pressure ulcers (insensate skin) | Any age |
| Allergy | Latex reactions (anaphylaxis risk) | Lifelong |
| Endocrine | Precocious puberty (associated with hydrocephalus) | Childhood |
| Respiratory | Central sleep apnea | Any age |
Intellectual outcomes: >70% of survivors have IQ >80. However, executive function, attention, and processing speed are disproportionately affected. With VP shunting, mean IQ ~80 (low normal). Without shunting, cognitive outcomes are better. Most children with lumbar lesions are educable.
Ambulation: 46-75% of children with lumbosacral MMC will walk (with or without assistive devices), depending on lesion level.
11. Prevention - What You Tell Parents and Primary Care
Folic acid - the key message:
- ALL women of childbearing age: 0.4 mg (400 mcg) daily (CDC recommendation)
- Women with a prior NTD pregnancy or on antiepileptic drugs: 4 mg/day (10x dose), starting 1 month before conception and continuing for first 3 months
- Mechanism: folate is essential for DNA synthesis, methylation reactions, and neural tube closure. Deficiency impairs closure at exactly the critical window (days 18-28)
- Fortification of cereal/grain products in many countries has reduced NTD rates by ~30-50%
Drugs to avoid in pregnancy (especially 1st trimester):
- Valproic acid (1-2% NTD risk)
- Carbamazepine
- Trimethoprim (folate antagonist)
- Methotrexate
12. Quick Summary for the Bedside
"Spot diagnosis" of MMC at birth:
- Posterior midline sac (lumbosacral most common)
- Flaccid lower limbs or absent voluntary movement
- Absent anal wink
- Macrocephaly / bulging fontanelle (hydrocephalus)
- Possible stridor (Chiari II vocal cord palsy)
Your first 6 steps:
- Latex-free protocol - from this moment
- Prone positioning with sac protected (sterile moist gauze + doughnut)
- Thermoregulation in incubator (high insensible losses)
- IV access + extra fluids
- Cranial ultrasound + renal ultrasound
- Urgent Neurosurgery + Urology consults
Remember the triad of associated anomalies: Chiari II + Hydrocephalus + Neurogenic bladder - all three need active management.
Sources: The Developing Human (Moore & Persaud, 9e); Bradley & Daroff's Neurology in Clinical Practice (8e); Miller's Anesthesia 10e; Creasy & Resnik's Maternal-Fetal Medicine; Medical Physiology (Boron & Boulpaep); Medical Physiology (Guyton). Recent evidence: Kunpalin et al., 2025, PMID 40492626 and Oliveira et al., 2025, PMID 40779058.
This is a shared conversation. Sign in to Orris to start your own chat.