Hiv in microbiology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
I now have comprehensive data. Let me compile the full, well-organized response on HIV in Microbiology.
HIV in Microbiology
1. Classification
HIV belongs to:
- Family: Retroviridae
- Subfamily: Orthoretrovirinae
- Genus: Lentivirus ("lenti" = slow, reflecting the slow, progressive nature of disease)
- Types: HIV-1 (globally dominant) and HIV-2 (less virulent, mainly West Africa)
HIV-1 is further divided into groups M, N, O, and P. Group M contains the major pandemic clades (subtypes A-K), reflecting origin from chimpanzees (SIVcpz). HIV-2 derives from sooty mangabeys (SIVsm). - Harrison's Principles of Internal Medicine 22E, p.1601
2. Structure and Morphology
HIV is an icosahedral, enveloped RNA virus, approximately 100-120 nm in diameter.
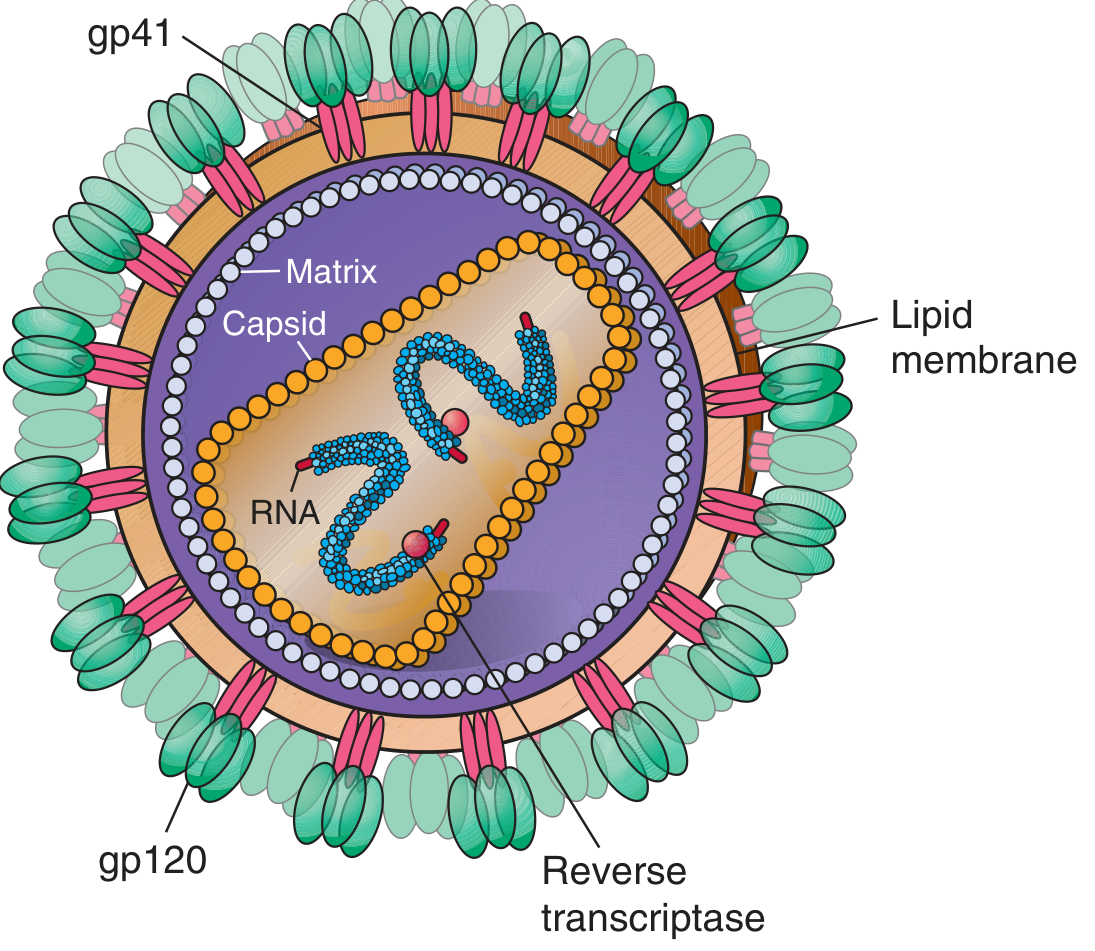
Figure: Cross-section of HIV-1 - Harrison's Principles of Internal Medicine 22E
Key structural components:
| Component | Gene | Function |
|---|---|---|
| gp120 | env | Outer envelope glycoprotein; binds CD4 receptor |
| gp41 | env | Transmembrane; mediates membrane fusion |
| p24 | gag | Capsid protein; diagnostic antigen |
| p17 | gag | Matrix protein; inner membrane |
| p55 | gag | Gag polyprotein precursor |
| Reverse transcriptase | pol | Converts RNA → DNA |
| Integrase | pol | Integrates proviral DNA into host genome |
| Protease | pol | Cleaves polyprotein precursors |
The virion buds from the infected cell surface and incorporates host cell lipid bilayer proteins into its envelope. The envelope spikes exist as trimeric heterodimers of gp120-gp41. - Harrison's Principles of Internal Medicine 22E, p.1601
3. Genome
HIV has a diploid, single-stranded, positive-sense RNA genome (~9.7 kb), flanked by Long Terminal Repeats (LTRs) which contain regulatory elements.
Core genes (shared with all retroviruses):
- gag - encodes core structural proteins (matrix p17, capsid p24, nucleocapsid p7)
- pol - encodes enzymes: protease, reverse transcriptase (p66/p51), RNase H, integrase
- env - encodes envelope glycoproteins (gp160 → gp120 + gp41)
Regulatory/accessory genes (unique to HIV-1):
- tat - transactivates viral transcription (essential)
- rev - regulates export of unspliced mRNA from nucleus (essential)
- nef - downregulates CD4 and MHC class I expression; enhances viral replication
- vif - overcomes host restriction factor APOBEC3G
- vpr - nuclear import of preintegration complex; G2 cell cycle arrest
- vpu (HIV-1 only) - degrades CD4 in ER; enhances virion release
HIV-2 lacks vpu and instead has vpx, which degrades the restriction factor SAMHD1. - Harrison's Principles of Internal Medicine 22E, p.1602
4. Replication Cycle
The replication cycle proceeds through the following steps:
Step 1 - Attachment:
gp120 binds CD4 molecule (55-kDa protein, predominantly on T-helper lymphocytes) with high affinity.
Step 2 - Co-receptor binding:
gp120 undergoes conformational change and binds one of two major co-receptors:
- CCR5 (CC-chemokine receptor 5) - used by macrophage-tropic (M-tropic/R5) strains, predominant early in infection
- CXCR4 (CXC-chemokine receptor 4) - used by T-tropic (X4) strains, emerge later in disease
Both are seven-transmembrane-domain G protein-coupled receptors.
Step 3 - Fusion:
After co-receptor binding, gp41 is exposed and penetrates the target cell plasma membrane, folding upon itself to bring virion and host cell membranes together. Fusion occurs.
Step 4 - Uncoating and reverse transcription:
Capsid uncoating is initiated, forming the preintegration complex (viral RNA + enzymes + accessory proteins). As this complex traverses the cytoplasm toward the nucleus, reverse transcriptase (an error-prone enzyme with ~1 mutation per replication cycle) converts the single-stranded genomic RNA into double-stranded DNA (proviral DNA).
Step 5 - Nuclear import and integration:
The proviral DNA is transported into the nucleus, where integrase catalyzes its integration into the host chromosome, forming provirus. Latency begins.
Step 6 - Transcription and translation:
Host RNA polymerase II transcribes the provirus. Tat amplifies transcription. Rev shuttles unspliced mRNAs to the cytoplasm. Gag, Pol, and Env polyproteins are translated.
Step 7 - Assembly, budding, and maturation:
New virions assemble at the cell membrane and bud off. Protease cleaves the Gag and Pol polyproteins during or after budding, producing mature, infectious virions. - Harrison's Principles of Internal Medicine 22E, p.1601-1602
Key fact: Reverse transcriptase is error-prone and lacks proofreading activity, leading to ~1 mutation per virion per replication cycle. Every nucleotide of the HIV genome likely mutates on a daily basis across the viral population. - Jawetz Melnick & Adelbergs Medical Microbiology 28E, p.665
5. Cellular Tropism
| Cell Type | Co-receptor | Strain Type | Timing |
|---|---|---|---|
| CD4+ T lymphocytes | CXCR4 | T-tropic (X4) | Late infection |
| Monocytes/Macrophages | CCR5 | M-tropic (R5) | Early infection, predominant |
| Dendritic cells | DC-SIGN (binds gp120) | - | Facilitates spread to T cells |
| Microglial cells (brain) | CCR5 | M-tropic | Neuropathogenesis |
Individuals homozygous for the CCR5-Δ32 deletion are largely resistant to HIV-1 infection - a finding that led to the concept of the "Berlin Patient" cure via CCR5-null bone marrow transplant. - Jawetz Melnick & Adelbergs Medical Microbiology 28E
6. Natural History of Infection
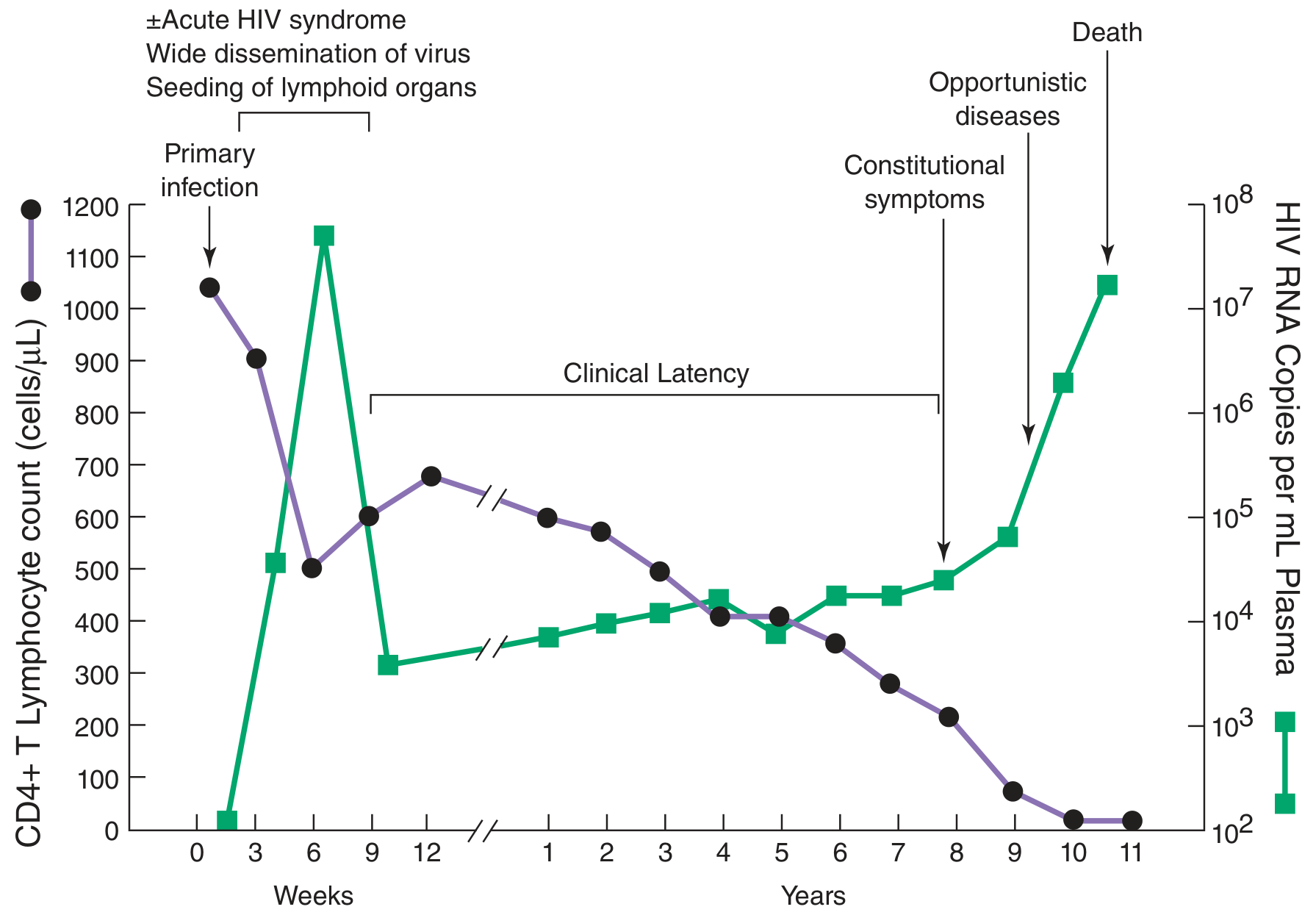
Figure: Typical course of untreated HIV infection - Jawetz Melnick & Adelbergs Medical Microbiology 28E
Phases:
-
Primary (Acute) HIV infection (weeks 1-12): 4-11 day window before detectable viremia. 50-75% develop an acute mononucleosis-like syndrome (fever, rash, lymphadenopathy, pharyngitis) 3-6 weeks post-infection. Sharp drop in CD4 count. Plasma viremia is detectable 8-12 weeks.
-
Clinical Latency (months to ~10 years): CD4 count rebounds but virus continues replicating at a high rate (~10 billion particles produced and destroyed per day, viral half-life ~6 hours). CD4 count slowly declines. This phase is asymptomatic but infectious.
-
Symptomatic HIV / AIDS: As CD4 count falls:
- <500/μL: Constitutional symptoms, recurrent infections
- <200/μL: AIDS-defining illnesses (PCP, toxoplasmosis, CMV retinitis, cryptococcal meningitis)
- <50/μL: MAC (Mycobacterium avium complex), CMV disease
AIDS-defining malignancies: Kaposi sarcoma (HHV-8), non-Hodgkin lymphoma (EBV), invasive cervical carcinoma (HPV). - Jawetz Melnick & Adelbergs Medical Microbiology 28E, p.666
7. Viral Latency
A small fraction of infected CD4 T cells survive and revert to a resting memory state, forming a long-lived, stable latent reservoir. In this state, HIV gene expression is silenced (provirus integrated but not transcribed). This reservoir:
- Contains fewer than 1 cell per million resting CD4 T cells in treated patients
- Decays very slowly - would take ~70 years to clear with standard therapy
- Reactivates when memory cells are stimulated by antigen or when ART is stopped
This latent reservoir is the primary barrier to HIV cure. - Jawetz Melnick & Adelbergs Medical Microbiology 28E
8. Immunity
- Humoral: Antibodies to envelope glycoproteins (gp41, gp120, gp160) persist. Antibodies to Gag proteins (p24, p17) decline as disease progresses; loss of anti-p24 heralds disease progression.
- Cell-mediated: CD8+ cytotoxic T cells respond to HIV antigens, but cannot fully clear infection.
- Immune evasion: HIV mutates rapidly (quasispecies); dense glycosylation of gp120 shields neutralizing antibody epitopes; downregulates MHC I via Nef; depletes the very CD4+ T cells needed to coordinate the immune response.
9. Laboratory Diagnosis
| Test | Detects | Notes |
|---|---|---|
| 4th-generation EIA (Ag/Ab combo) | p24 antigen + HIV-1/2 antibodies | Standard initial test; window period ~18 days |
| 5th-generation assay | HIV-1 Ab, HIV-2 Ab, p24 Ag (differentiated) | Newer; differentiates HIV-1 from HIV-2 |
| Western blot / Immunoblot | HIV antibodies to specific proteins | Confirmatory test; bands at gp160, gp120, p24 |
| HIV RNA (viral load PCR) | HIV-1 RNA copies/mL | Detects acute infection; monitors treatment; window ~7-10 days |
| CD4 count | CD4+ T lymphocyte count | Staging; guides prophylaxis; normal >500/μL |
| HIV DNA PCR | Proviral DNA in cells | Used in neonates (maternal antibodies interfere with serology) |
| HIV Genotype Resistance Test | Mutations in RT and protease genes | Guides ART selection |
| Coreceptor tropism assay | CCR5 vs CXCR4 use | Required before prescribing CCR5 antagonists (maraviroc) |
Seroconversion: Mean time 3-4 weeks post-infection; virtually all seropositive by 6 months. - Jawetz Melnick & Adelbergs Medical Microbiology 28E, p.669-670
10. Antiretroviral Drug Targets
| Drug Class | Target | Examples |
|---|---|---|
| NRTIs | Reverse transcriptase (nucleoside analog) | Zidovudine, Tenofovir, Emtricitabine |
| NNRTIs | Reverse transcriptase (non-nucleoside) | Efavirenz, Nevirapine |
| Protease inhibitors (PIs) | Viral protease | Ritonavir, Lopinavir |
| Integrase inhibitors (INSTIs) | Integrase | Raltegravir, Dolutegravir, Bictegravir |
| Fusion inhibitors | gp41 | Enfuvirtide (T-20) |
| CCR5 antagonists | CCR5 co-receptor | Maraviroc |
| CD4 post-attachment inhibitor | CD4 molecule | Ibalizumab |
Current preferred regimens are 3-drug combinations (typically 2 NRTIs + 1 INSTI) known as ART (antiretroviral therapy). - Jawetz Melnick & Adelbergs Medical Microbiology 28E; Harrison's Principles of Internal Medicine 22E
Key Summary Points for Exams
- HIV-1 belongs to Lentivirus genus, Retroviridae family
- Hallmark enzyme: reverse transcriptase (RNA → DNA)
- Primary receptor: CD4 | Co-receptors: CCR5 (macrophage-tropic, early) and CXCR4 (T-tropic, late)
- AIDS is defined by CD4 count <200 cells/μL or an AIDS-defining illness
- 10 billion viral particles produced and destroyed daily during latency
- p24 antigen is the earliest detectable marker; viral RNA (PCR) has the shortest window period
- Latent reservoir in resting memory CD4 T cells is the main barrier to cure
- Nef downregulates CD4 and MHC-I; Vif overcomes APOBEC3G restriction; Tat is the transcriptional transactivator
This is a shared conversation. Sign in to Orris to start your own chat.