Explain each and everything about Spinal Cord and Ascending, Descending, and lntersegmental Tracts. I want even the minor details about the topic. Also explain all the clinicals along the content
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
The Spinal Cord: Complete Guide to Structure, Tracts, and Clinical Correlations
Sources: Gray's Anatomy for Students; Neuroanatomy through Clinical Cases 3rd Ed; Medical Physiology (Boron & Boulpaep); Adams & Victor's Principles of Neurology 12th Ed
PART 1: GROSS ANATOMY AND EXTERNAL FEATURES
The spinal cord is the elongated cylindrical part of the CNS housed within the vertebral canal. It extends from the foramen magnum (continuous with the medulla oblongata) to approximately the level of L1-L2 vertebra in adults, ending as the conus medullaris. Below this, spinal nerve roots continue as the cauda equina ("horse's tail").
Dimensions: About 45 cm long in males, 42 cm in females. Diameter: ~1 cm.
Two enlargements:
- Cervical enlargement (C5-T1): Accommodates the brachial plexus innervating the upper limb
- Lumbosacral enlargement (L1-S3): Accommodates the lumbosacral plexus innervating the lower limb
External sulci and fissures:
- Anterior median fissure: Deep midline groove anteriorly, contains the anterior spinal artery
- Posterior median sulcus: Shallow midline groove posteriorly
- Posterolateral sulcus (bilateral): Where dorsal roots enter; separates posterior and lateral funiculi
- Anterior lateral sulcus: Where ventral roots exit
- Posterior intermediate sulcus (cervical only): Divides the posterior funiculus into fasciculus gracilis (medial) and fasciculus cuneatus (lateral)
- Lissauer's tract (posterolateral tract): Small, visible zone at the dorsal root entry zone
Meningeal coverings (from outside in):
- Dura mater (tough outer layer)
- Arachnoid mater
- Subarachnoid space (contains CSF - clinically important for lumbar puncture)
- Pia mater (closely applied to cord surface)
Ligamentum denticulatum: Lateral extensions of pia mater that attach to the dura between nerve roots, suspending the cord within the dural sac.
Filum terminale: A thread of pia mater descending from the conus medullaris. The internal filum terminale continues to the level of S2; the external filum terminale (filum of the dural sac) continues to the coccyx.
PART 2: INTERNAL STRUCTURE
A cross-section of the spinal cord reveals two distinct zones:
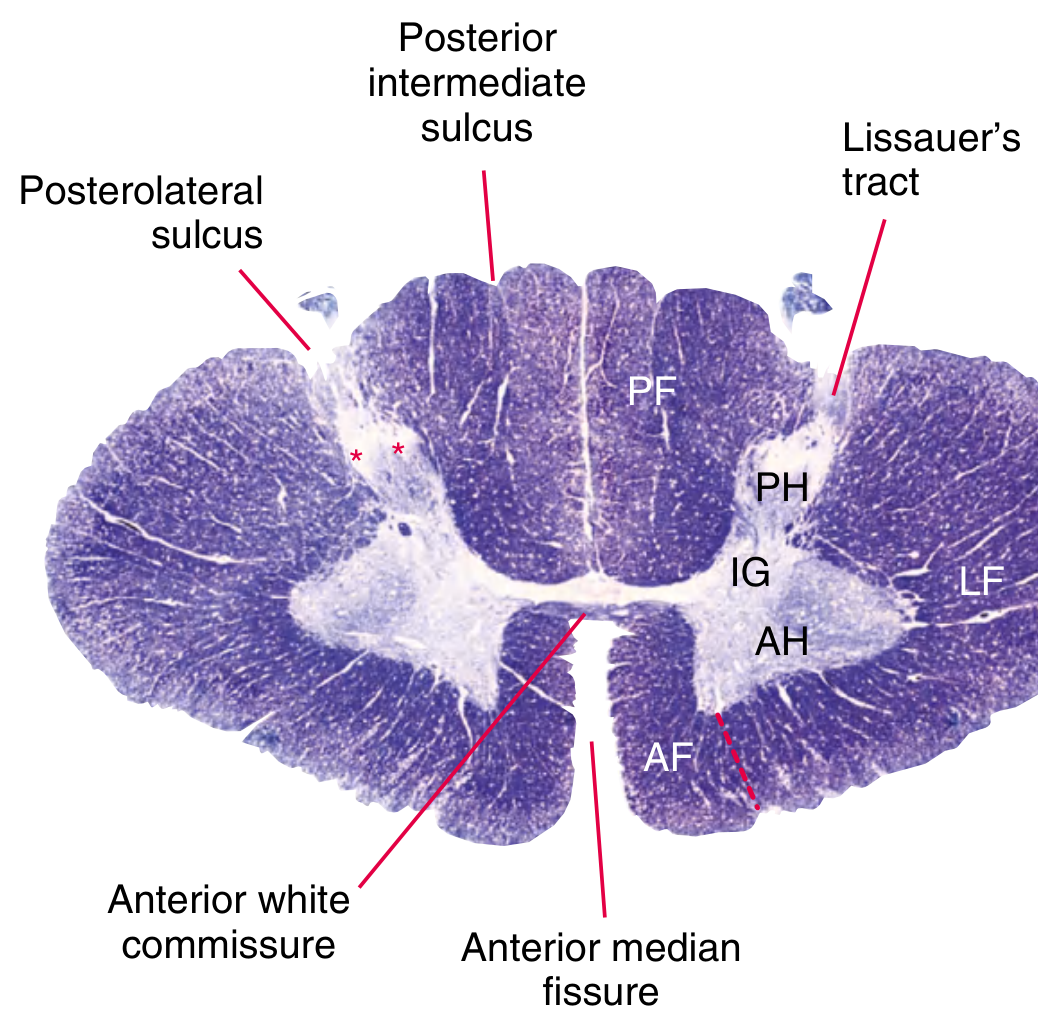
2A. Gray Matter (Inner H-shape or "Butterfly")
The gray matter consists of neuronal cell bodies, dendrites, unmyelinated axons, and glia. It is arranged in anterior (ventral) and posterior (dorsal) horns connected by the gray commissure (which surrounds the central canal).
Anterior (Ventral) Horns: Contain alpha motor neuron cell bodies (large, multipolar) and gamma motor neuron cell bodies. These are the lower motor neurons (LMNs) that project peripherally via the ventral roots.
- Medial motor nuclei: innervate axial and girdle muscles
- Lateral motor nuclei: present in cervical and lumbosacral enlargements; innervate distal limb muscles
Posterior (Dorsal) Horns: Receive incoming sensory information from the dorsal root ganglia. They relay sensory signals onward.
Lateral Horn (Intermediolateral Cell Column): Present only at T1-L2 (sympathetic) and S2-S4 (parasympathetic). Contains preganglionic autonomic neurons.
- The T1-L2 lateral horn gives rise to preganglionic sympathetic fibers
- S2-S4 gives rise to preganglionic parasympathetic fibers (pelvic splanchnic nerves)
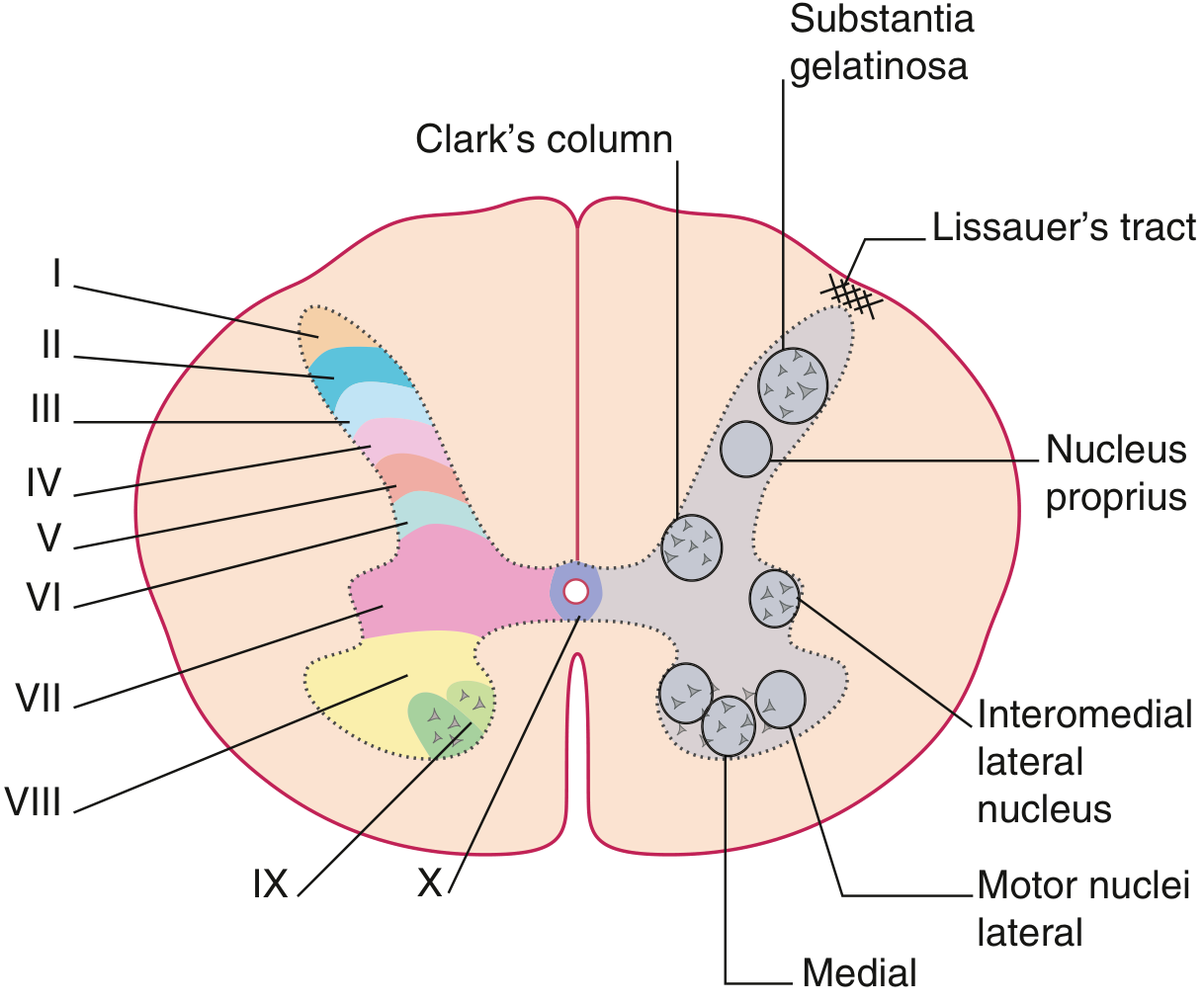
2B. Rexed's Laminae (10 zones of cytoarchitecture)
| Lamina | Location | Function / Key Contents |
|---|---|---|
| I | Dorsal horn tip (marginal zone) | Pain and temperature (sharp pain, nociception); receives input from A-delta and C fibers |
| II | Substantia gelatinosa | Pain modulation gate; receives C fiber input; site of enkephalin-mediated inhibition |
| III-IV | Nucleus proprius | Fine touch, pressure, vibration; relay for dorsal column collaterals |
| V | Neck of dorsal horn | Wide-dynamic-range neurons; convergence of somatic and visceral pain; receives descending control |
| VI | Base of dorsal horn (limb enlargements only) | Proprioception from muscle spindles |
| VII | Intermediate zone | Clark's column (nucleus thoracicus, C8-L3): origin of dorsal spinocerebellar tract; also the intermediolateral column |
| VIII | Medial anterior horn | Interneurons; receives descending medial motor system input |
| IX | Motor nuclei (lateral and medial anterior horn) | Alpha and gamma motor neurons |
| X | Around central canal | Visceral afferents; pain modulation |
2C. White Matter
Surrounds the gray matter and consists of myelinated axon bundles organized into funiculi (columns):
- Anterior (ventral) funiculus: Between the anterior median fissure and anterior lateral sulcus. Contains mainly motor (descending) axons.
- Posterior (dorsal) funiculus: Between the posterior median sulcus and posterior lateral sulcus. Contains sensory (ascending) axons.
- Lateral funiculus: Between anterior and posterior lateral sulci. Contains both ascending sensory and descending motor tracts.
Central canal: A tiny remnant of the neural tube lumen lined by ependymal cells. It is patent in children but often obliterates in adults. Contains CSF.
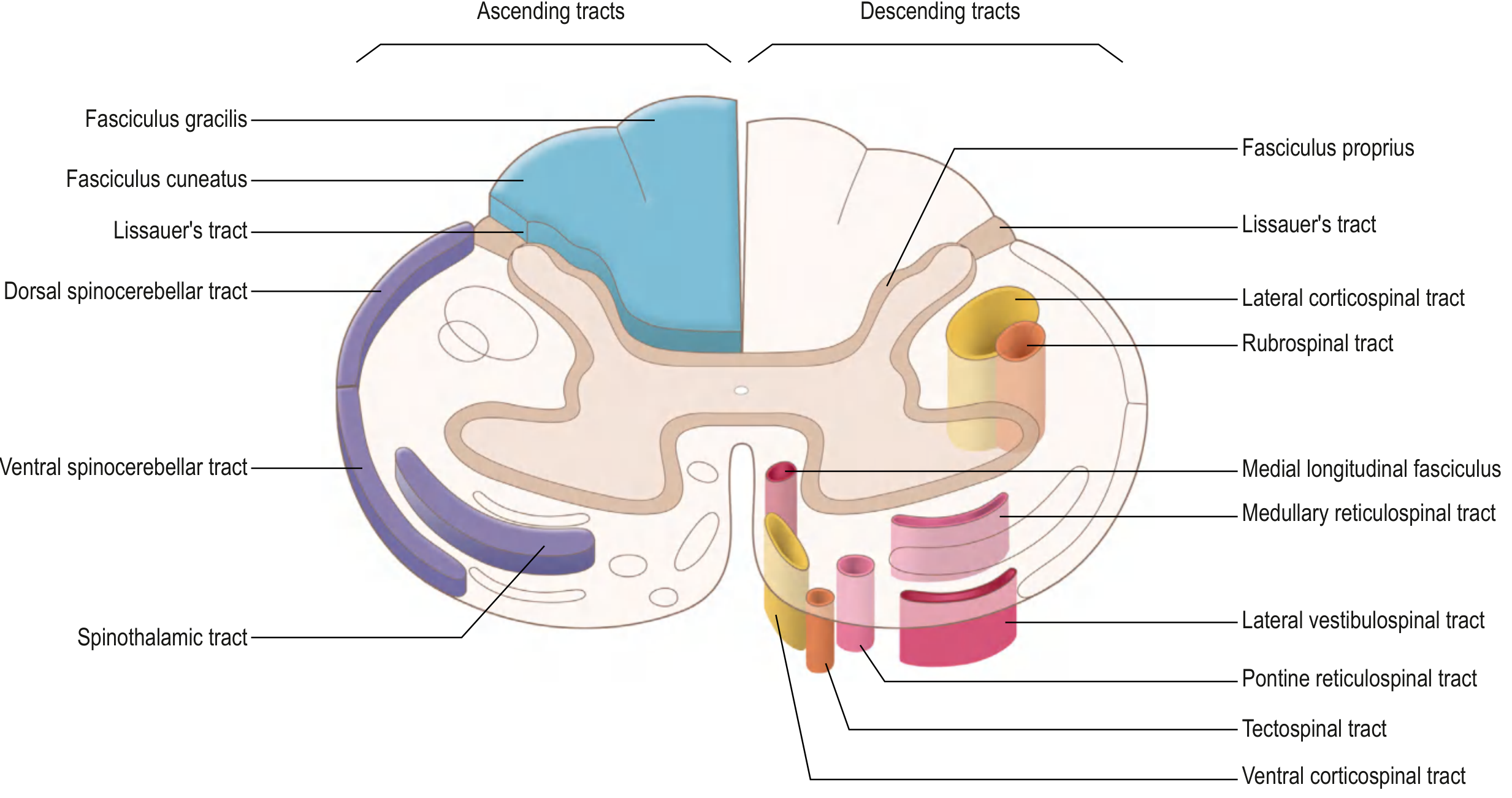
PART 3: ASCENDING TRACTS (Sensory Pathways)
"Two somatosensory pathways ascend within the spinal cord to reach the cortex: the anterolateral pathways, which convey sensations of pain, temperature, and crude touch; and the posterior column-medial lemniscal pathway, which conveys sensations of discriminative or fine touch, vibration, and conscious proprioception." - Gray's Anatomy for Students
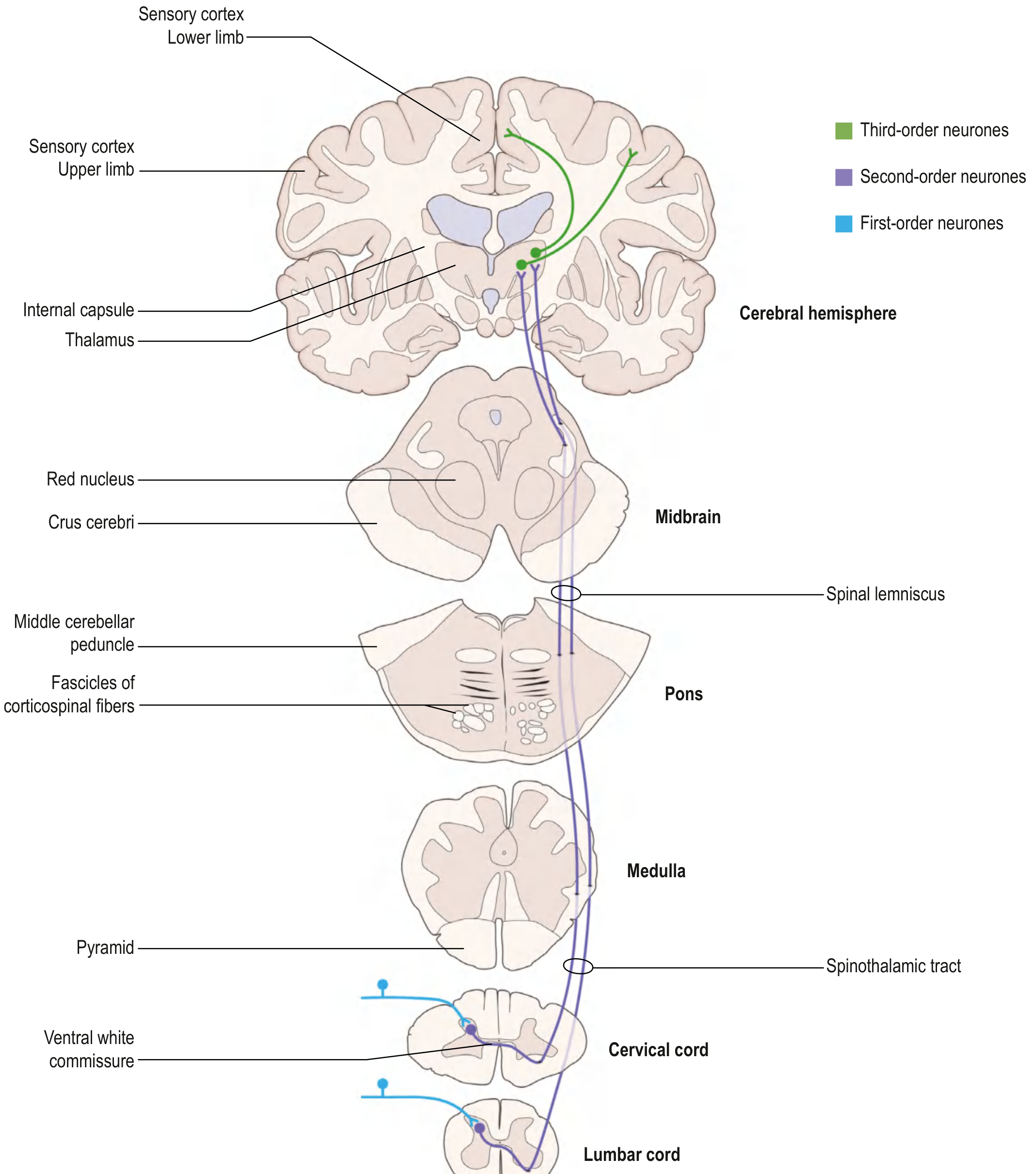
3A. ANTEROLATERAL PATHWAYS (Spinothalamic System)
Location in cord: Anterolateral white matter (lateral funiculus predominantly)
This system transmits pain, temperature, crude touch, and itch. It consists of three tracts:
3A.1 Lateral Spinothalamic Tract (Neospinothalamic)
Modalities: Sharp, localized pain and temperature
Three-neuron pathway:
1st-order neuron:
- Cell body in the dorsal root ganglion (DRG)
- Peripheral process: receives input from free nerve endings (pain, temperature)
- A-delta (thinly myelinated): sharp, fast pain and cold temperature
- C fibers (unmyelinated): dull, burning pain and warm temperature
- Central process enters spinal cord via the posterolateral sulcus (dorsal root entry zone)
- Travels 1-2 segments up or down in Lissauer's tract (posterolateral tract of Lissauer) before synapsing
- Synapses on 2nd-order neurons in dorsal horn laminae I and V (and some in laminae IV and VII)
2nd-order neuron:
- Cell body in dorsal horn (laminae I and V)
- Axon crosses obliquely through the anterior (ventral) white commissure to the contralateral side
- Critically: this crossing takes 2-3 spinal cord segments, so the spinothalamic tract represents contralateral pain/temperature beginning 2-3 segments below the level of entry
- After crossing, axons ascend in the anterolateral white matter as the spinothalamic tract (lateral portion)
- Somatotopic arrangement: sacral fibers are MOST lateral, cervical fibers are most medial (fibers from the anterior commissure add on medially as they ascend)
- Continues through medulla (lateral position, between olive and inferior cerebellar peduncle), pons (just lateral to medial lemniscus), midbrain tegmentum
- Synapses in the ventral posterior lateral (VPL) nucleus of the thalamus
3rd-order neuron:
- Cell body in VPL thalamus
- Projects via posterior limb of the internal capsule and corona radiata
- Terminates in primary somatosensory cortex (postcentral gyrus, Brodmann areas 3, 1, 2)
- Also sends collaterals to secondary somatosensory cortex in the parietal operculum
3A.2 Spinoreticular Tract (Paleospinothalamic)
Modalities: Diffuse, burning, poorly localized pain; the emotional and arousal aspects of pain ("suffering")
Course:
- 1st-order neuron: same as spinothalamic
- 2nd-order neuron: Cell body in dorsal horn laminae I, V, VII, VIII
- Axons cross (mostly) to the contralateral side and ascend in the anterolateral system
- Terminate in the medullary and pontine reticular formation
- From there, neurons project to intralaminar thalamic nuclei (central lateral nucleus) and medial thalamic nuclei (mediodorsal nuclei)
- Final projections reach widespread cortical areas and the limbic system (accounting for the emotional component of pain)
3A.3 Spinomesencephalic Tract (Spinotectal)
Modalities: Pain modulation; contributes to central pain control
Course:
- 2nd-order neurons in dorsal horn laminae I, IV, V
- Cross and ascend with the spinothalamic tract
- Terminate in the periaqueductal gray matter (PAG) and the superior colliculus of the midbrain
- The PAG is critical for descending pain modulation (stimulation produces analgesia via serotonergic and noradrenergic descending pathways)
- The superior colliculus component helps mediate visual-nociceptive reflexes
3B. POSTERIOR COLUMN - MEDIAL LEMNISCAL PATHWAY (PCML)
Location in cord: Posterior funiculus
Modalities: Fine (discriminative) touch, two-point discrimination, vibration sense, conscious proprioception (joint position sense), stereognosis, graphesthesia
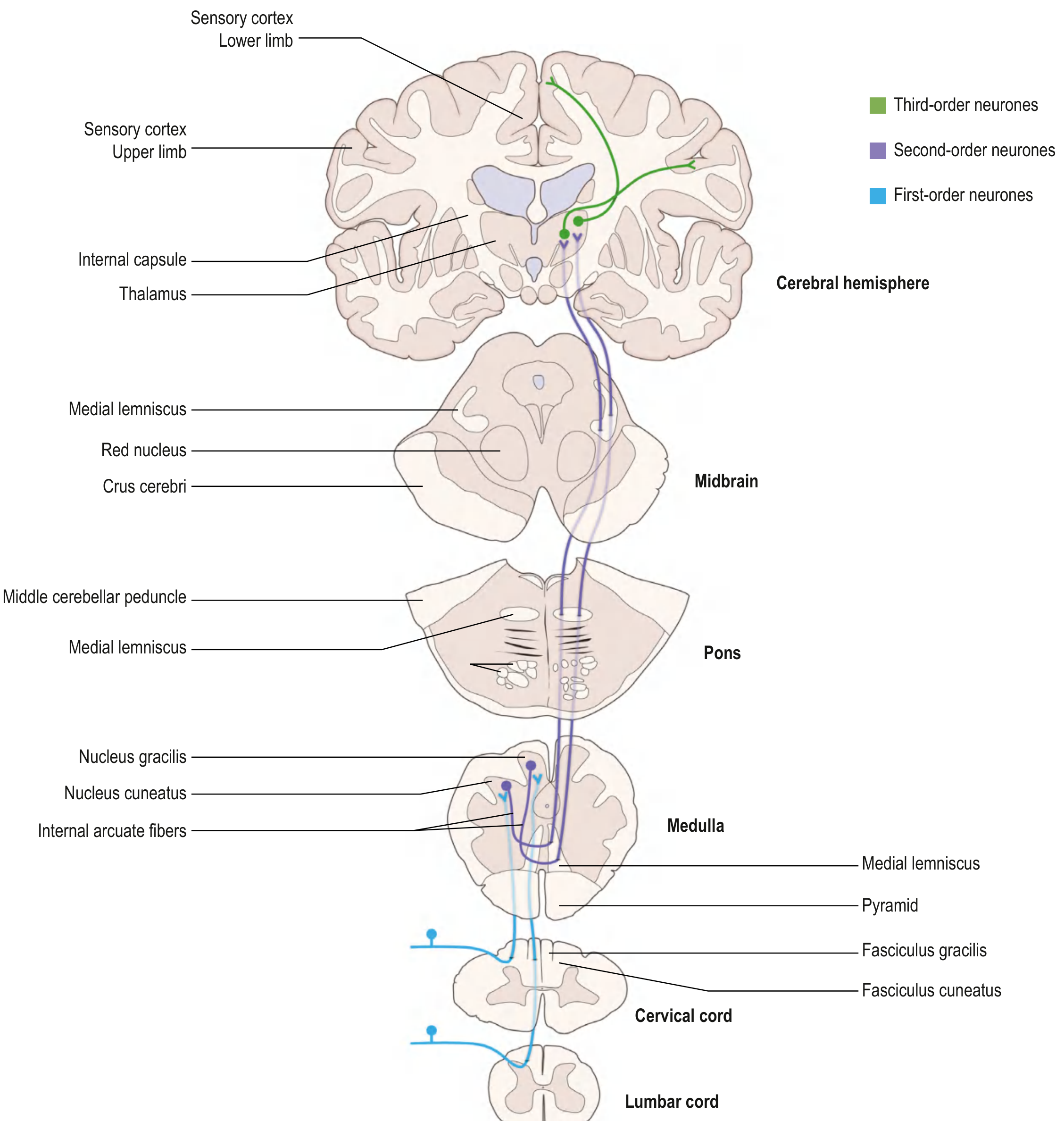
Three-neuron pathway:
1st-order neuron:
- Cell body in the DRG
- Peripheral process from specialized mechanoreceptors (Meissner's corpuscles, Pacinian corpuscles, Merkel's discs, muscle spindles, Golgi tendon organs)
- Central process enters the spinal cord and immediately ascends ipsilaterally in the posterior funiculus (no synapse in the cord itself)
- Fasciculus gracilis (medial): Carries information from the lower limb and lower trunk (T7 and below). Present throughout the cord.
- Fasciculus cuneatus (lateral): Carries information from the upper limb, upper trunk, and neck (T6 and above). Only present above T6.
2nd-order neuron:
- Fasciculus gracilis terminates in nucleus gracilis in the caudal medulla
- Fasciculus cuneatus terminates in nucleus cuneatus in the caudal medulla
- 2nd-order axons sweep anteromedially as internal arcuate fibers and decussate in the caudal medulla
- After decussation, these fibers form the medial lemniscus on the contralateral side
- The medial lemniscus ascends through the brainstem (lies medially in the medulla, rotates laterally as it ascends through pons and midbrain)
- Terminates in the VPL nucleus of the thalamus
3rd-order neuron:
- VPL projects via posterior limb of internal capsule to primary somatosensory cortex (postcentral gyrus)
- Somatotopic map: foot and leg most medial (near interhemispheric fissure), face most lateral
Key distinction from spinothalamic: The PCML pathway decussates in the medulla (not the spinal cord). Therefore, spinal cord lesions affect the PCML ipsilaterally but the spinothalamic contralaterally - the basis of Brown-Sequard syndrome (see clinicals).
3C. SPINOCEREBELLAR TRACTS (Subconscious Proprioception)
These pathways carry proprioceptive information to the cerebellum for coordination - they do NOT reach conscious perception.
3C.1 Dorsal (Posterior) Spinocerebellar Tract
Modality: Unconscious proprioception and kinesthesia from the lower limb and trunk
Course:
- 1st-order neuron: DRG
- 2nd-order neuron: Clarke's nucleus (nucleus thoracicus dorsal) - located in lamina VII at C8-L3
- Axons ascend ipsilaterally (uncrossed) in the lateral funiculus as the dorsal spinocerebellar tract
- Enters the cerebellum via the inferior cerebellar peduncle
- Terminates in the ipsilateral cerebellar cortex (vermis)
Note: Information from sacral/lower lumbar segments reaches Clarke's column by traveling up the posterior column to the level where Clarke's column begins.
3C.2 Ventral (Anterior) Spinocerebellar Tract
Modality: Unconscious proprioception from the lower limb; uniquely carries information about the activity of interneuronal circuits (efference copy)
Course:
- 2nd-order neurons in laminae V-VII (spinal border cells)
- Most axons cross in the anterior commissure and ascend contralaterally in the lateral funiculus
- Ascend all the way to the pons and midbrain
- Enter the cerebellum via the superior cerebellar peduncle, then re-cross within the cerebellum
- Net result: the information reaches the ipsilateral cerebellum (double crossover)
3C.3 Cuneocerebellar Tract (Rostral Spinocerebellar Tract)
Modality: Unconscious proprioception from the upper limb (analogous to dorsal spinocerebellar for the arms)
- 2nd-order neurons in the accessory (external) cuneate nucleus in the medulla
- Ascends ipsilaterally via the inferior cerebellar peduncle to the cerebellar cortex
3D. SPINOCERVICAL TRACT
- Axons ascend ipsilaterally in the dorsolateral funiculus to the lateral cervical nucleus (at C1-C2)
- Then cross and join the medial lemniscus to reach the thalamus
- Function: fine touch and proprioception (a phylogenetically older alternative to the PCML)
PART 4: DESCENDING TRACTS (Motor Pathways)
"Descending tracts through the spinal cord are involved in voluntary movements; postural movements; and coordination of head, neck, and eye movements. These pathways originate from the cerebral cortex and brainstem and are influenced by sensory input and feedback from the cerebellum and basal ganglia." - Gray's Anatomy for Students
Descending tracts are divided into two systems:
- Lateral motor system - controls distal limb muscles (skilled voluntary movement)
- Medial motor system - controls axial and proximal muscles (posture, balance, gait)
LATERAL MOTOR SYSTEM
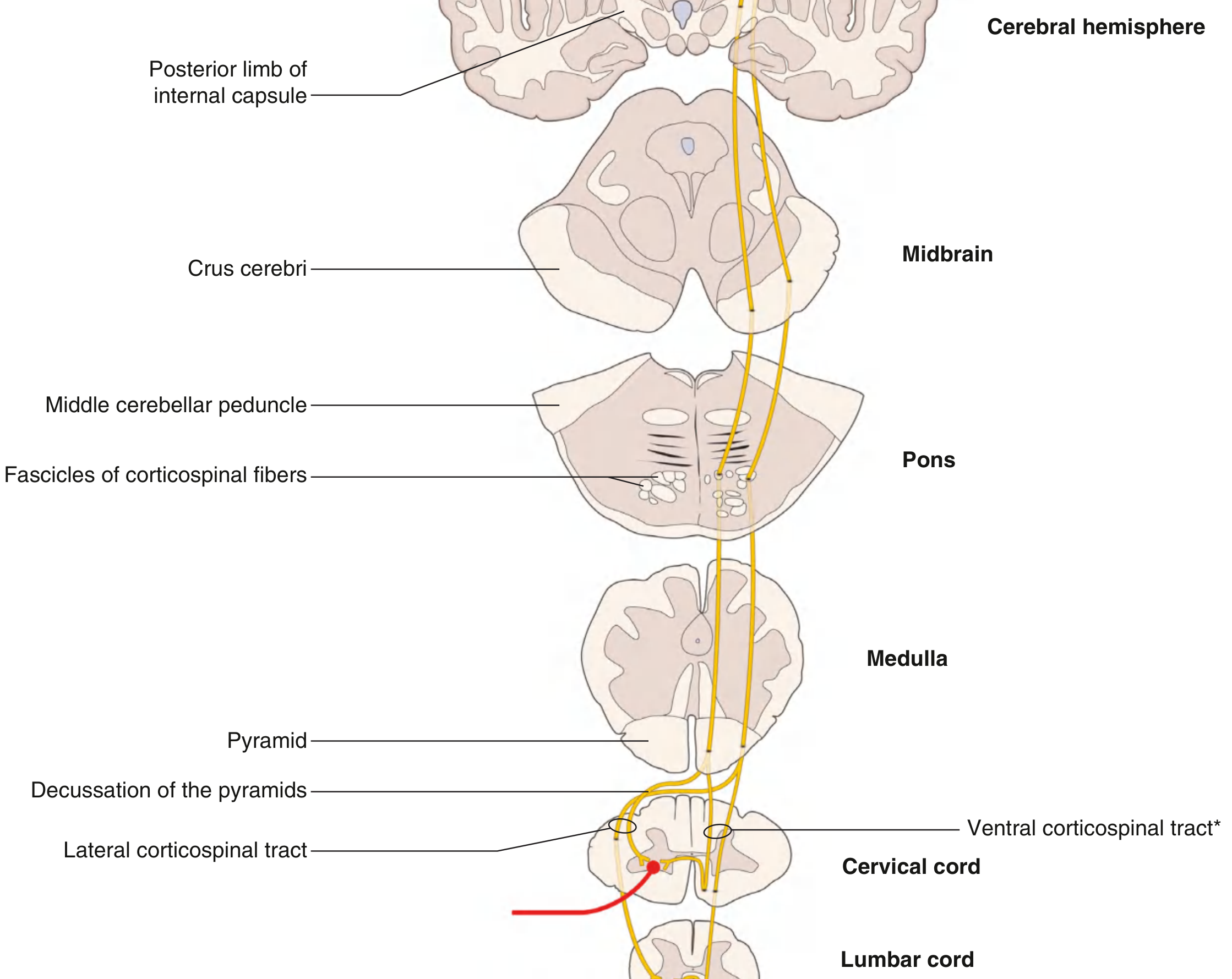
4A. Lateral Corticospinal Tract (LCST) - THE PYRAMIDAL TRACT
The most clinically important descending tract in the spinal cord.
Location: Lateral funiculus (posterior half)
Function: Voluntary, skilled, fractionated movements of contralateral limbs - especially fine finger movements
Full course (Upper Motor Neuron - UMN):
Origin: Primary motor cortex (precentral gyrus, Brodmann area 4) - the large Betz cells (giant pyramidal cells). Also contributions from premotor cortex (area 6), supplementary motor area (SMA), and somatosensory cortex (areas 3,1,2).
-
Axons descend through the corona radiata → posterior limb of the internal capsule (somatotopically: face anterior, arm middle, leg posterior) → crus cerebri (middle three-fifths) of the midbrain
-
As the tract passes through the pons, it breaks up into small fascicles to accommodate transverse pontocerebellar fibers
-
Re-forms into the pyramids at the ventral medulla (visible as longitudinal ridges on the anterior surface of the medulla)
-
At the cervicomedullary junction, approximately 85-90% of fibers decussate as the pyramidal (motor) decussation → become the lateral corticospinal tract in the contralateral lateral funiculus
-
Remaining 10-15% do NOT decussate and instead descend as the anterior corticospinal tract (see medial system)
-
LCST descends the entire length of the cord in the lateral funiculus
-
Synapses:
- Directly on alpha motor neurons (lamina IX) - especially for fine distal movements
- On interneurons (lamina VII, VIII) - for most proximal movements
LMN (Lower Motor Neuron):
- Cell bodies in lamina IX (anterior horn)
- Exit via ventral roots → spinal nerves → peripheral nerves → neuromuscular junction
Somatotopic organization of LCST in cord:
- Cervical fibers (arm): medial
- Lumbar fibers (leg): lateral
4B. Rubrospinal Tract
Location: Lateral funiculus, just anterior to LCST
Function: Assists in flexor muscle activity of the contralateral upper limb; may partially compensate after LCST damage (important in lower vertebrates; uncertain significance in adult humans)
Course:
- Origin: Magnocellular division of the red nucleus in the midbrain tegmentum
- Axons immediately decussate at the level of origin as the ventral tegmental decussation (in the midbrain)
- Descend in the lateral funiculus
- Terminate only on cervical cord interneurons (anterior horn, lamina V-VII)
- Synapse on interneurons facilitating flexor muscles and inhibiting extensor muscles of the upper limb
MEDIAL MOTOR SYSTEM
4C. Anterior (Ventral) Corticospinal Tract
Location: Anterior funiculus (near midline)
Function: Control of bilateral axial and girdle muscles; involved in postural adjustments
Course:
- Origin: Primary motor cortex and SMA
- The 10-15% of corticospinal fibers that do NOT decussate at the pyramidal decussation
- Descend ipsilaterally in the anterior funiculus
- Terminate only in cervical and upper thoracic cord
- Most fibers eventually cross in the anterior white commissure at the segmental level before synapsing on interneurons in lamina VIII (and some lamina IX)
- Projects bilaterally to medial anterior horn motor neurons controlling axial muscles
4D. Vestibulospinal Tracts
Location: Anterior funiculus (medial)
Function: Maintaining balance and upright posture by facilitating extensor/antigravity muscles and inhibiting flexor muscles
There are two vestibulospinal tracts:
Lateral Vestibulospinal Tract (LVST):
- Origin: Lateral vestibular nucleus (Deiters' nucleus) in the pons/medulla
- Input to lateral vestibular nucleus: ipsilateral cerebellum and vestibular labyrinth
- Course: Descends ipsilaterally (uncrossed) through the entire length of the cord
- Terminates on interneurons in laminae VII-VIII (facilitates extensor alpha and gamma motor neurons)
- When you stumble, the LVST activates extensors to prevent falling
Medial Vestibulospinal Tract (MVST):
- Origin: Medial and inferior vestibular nuclei
- Travels within the medial longitudinal fasciculus (MLF)
- Projects bilaterally to cervical and upper thoracic cord only
- Function: Reflexive control of head and neck position
4E. Reticulospinal Tracts
Location: Anterior and lateral funiculi
Function: Regulation of voluntary movement, spinal reflex activity, tone, and autonomic outflow
Two reticulospinal tracts:
Pontine (Medial) Reticulospinal Tract:
- Origin: Nucleus reticularis pontis caudalis and oralis (pontine reticular formation)
- Descends ipsilaterally (largely) in the anterior funiculus
- Facilitates extensor tone (reinforces vestibulospinal facilitation of extensors)
- Terminates on laminae VII-VIII interneurons throughout the cord
Medullary (Lateral) Reticulospinal Tract:
- Origin: Nucleus reticularis gigantocellularis (medullary reticular formation)
- Descends bilaterally in the lateral funiculus
- Inhibits extensor tone (opposes the pontine reticulospinal)
- Also important for transmission of descending pain modulation signals
Combined function: Balance between pontine facilitation and medullary inhibition determines extensor muscle tone. Disruption (e.g., spasticity after UMN lesion) results from disinhibition of the vestibulo- and pontine reticulospinal tracts.
4F. Tectospinal Tract
Location: Anterior funiculus (near midline, medial to MLF)
Function: Reflex coordination of head and neck movements in response to visual and auditory stimuli
Course:
- Origin: Superior colliculus of the midbrain (visual reflex center)
- Axons decussate immediately as the dorsal tegmental decussation in the midbrain
- Descend only to cervical cord (C4 and above)
- Terminate on interneurons in laminae VI-VIII
- When a sudden visual stimulus appears to your side, the tectospinal tract reflexively turns your head toward it
4G. Medial Longitudinal Fasciculus (MLF) in the Cord
The MLF is primarily a brainstem tract but has a descending spinal component that carries:
- Descending vestibulospinal fibers (medial vestibulospinal tract)
- Connections from cranial nerve nuclei to cervical cord
- Function: Integrates eye, head, and neck movements for coordinated gaze
Motor Tract Summary Tables
Lateral Motor System:
| Tract | Origin | Decussation | Cord Level | Function |
|---|---|---|---|---|
| Lateral Corticospinal | Primary motor cortex | Pyramidal decussation (cervicomedullary junction) | Entire cord | Voluntary movement of contralateral limbs |
| Rubrospinal | Red nucleus (magnocellular) | Ventral tegmental decussation (midbrain) | Cervical cord only | Flexor activity of contralateral upper limb |
Medial Motor System:
| Tract | Origin | Decussation | Cord Level | Function |
|---|---|---|---|---|
| Anterior Corticospinal | Motor cortex + SMA | At segmental level (anterior commissure) | Cervical + upper thoracic | Bilateral axial/girdle muscles |
| Lateral Vestibulospinal | Lateral vestibular nucleus | None (ipsilateral) | Entire cord | Extensor facilitation (balance) |
| Medial Vestibulospinal | Medial/inferior vestibular nuclei | Bilateral | Cervical + upper thoracic | Head/neck positioning |
| Pontine Reticulospinal | Pontine reticular formation | Mostly ipsilateral | Entire cord | Extensor facilitation |
| Medullary Reticulospinal | Medullary reticular formation | Bilateral | Entire cord | Extensor inhibition, autonomic |
| Tectospinal | Superior colliculus | Dorsal tegmental decussation | Cervical cord only | Head-eye coordination reflexes |
PART 5: INTERSEGMENTAL TRACTS (Propriospinal Fibers)
Intersegmental tracts (also called propriospinal fibers or fasciculus proprius) are a critically important but often under-appreciated system that is unique to the spinal cord.
What Are They?
These are axons that originate and terminate entirely within the spinal cord - they do not project to the brain or to the periphery. They interconnect different levels (segments) of the spinal cord with one another.
Location
The fasciculus proprius surrounds the gray matter on all sides, forming a thin band of white matter directly adjacent to the gray:
- Anterior fasciculus proprius: around the anterior horn
- Lateral fasciculus proprius: around the lateral horn
- Posterior fasciculus proprius: between the posterior horn and the posterior funiculus
As noted in the spinal cord cross-section diagram above, the fasciculus proprius is visible surrounding the H-shaped gray matter.
Types Based on Length
-
Short intersegmental fibers: Connect adjacent 1-2 segments. Coordinate movements of closely related spinal cord segments (e.g., shoulder and elbow muscles during reach-and-grasp)
-
Long intersegmental fibers: Connect many segments, including connections between cervical and lumbosacral cord. Coordinate upper and lower limb movements (e.g., arm-leg coupling during walking/swimming)
Functions
-
Locomotor pattern generation: Propriospinal neurons are a key component of central pattern generators (CPGs) - neural circuits in the spinal cord that generate rhythmic, alternating limb movements for walking. The CPG can produce coordinated stepping without input from the brain (as demonstrated in spinalized animal preparations).
-
Interlimb coordination: Long propriospinal neurons in the cervical cord project to the lumbosacral cord to coordinate upper and lower limb movements during gait (e.g., the natural arm-swing that coordinates with leg movement during walking).
-
Reflex integration: Intersegmental reflexes (e.g., crossed extension reflex, long-spinal reflexes) are mediated through these fibers.
-
Relay for descending commands: Some descending motor commands (e.g., from the reticulospinal tract) reach spinal motor neurons not directly but via propriospinal relay neurons. This is particularly important for proximal limb movements.
-
Relay for ascending sensory: Some sensory information ascends via propriospinal chains rather than the dedicated sensory tracts.
The C3-C4 Propriospinal System (Clinically Important)
A particularly important group are the C3-C4 propriospinal neurons (PNs):
- Cell bodies in the C3-C4 segments
- Receive direct input from the corticospinal tract as well as reticulospinal inputs
- Project to motor neurons in the C6-Th1 segments controlling arm muscles
- Proposed to mediate a "propriospinal relay" in humans for reaching movements
- After corticospinal tract injury (e.g., stroke, spinal cord injury), these neurons can potentially mediate motor recovery by acting as an alternate relay
Lissauer's Tract (Posterolateral Tract)
While primarily an intersegmental tract for pain fibers, Lissauer's tract deserves special mention:
- Located at the tip of the posterior horn (dorsal root entry zone)
- Contains:
- Collateral branches of entering primary sensory axons (A-delta and C fibers from DRG) that ascend or descend 1-2 segments before entering the dorsal horn
- Propriospinal fibers from dorsal horn neurons
- Function: Allows one nociceptive stimulus to activate a broader zone of dorsal horn cells ("spreading" of pain signals). This is the basis for referred pain and pain radiation patterns.
PART 6: VASCULAR SUPPLY TO THE SPINAL CORD (Clinical Relevance)
Understanding the vascular supply helps explain specific clinical syndromes:
Arterial supply:
- Anterior spinal artery (ASA): Single midline vessel; formed by union of two branches from the vertebral arteries; runs in the anterior median fissure; supplies the anterior 2/3 of the cord, including the anterior horns, spinothalamic tracts, and corticospinal tracts (but NOT the posterior columns)
- Posterior spinal arteries (PSA): Two vessels (bilateral) running along the posterolateral sulci; branches of PICA or vertebral artery; supply the posterior 1/3 of the cord, including the posterior columns
- Artery of Adamkiewicz (arteria radicularis magna): The largest segmental medullary artery, usually at T9-L2 (predominantly left side); provides the dominant supply to the lower thoracic and lumbar cord
Venous drainage:
- Anterior and posterior spinal veins drain into a venous plexus (Batson's plexus), which connects to the azygous system
PART 7: CLINICAL CORRELATIONS
7A. Spinal Cord Injury (SCI) - Level and Completeness
Complete SCI: All motor, sensory, and autonomic function is lost below the lesion level. AIS grade A (ASIA Impairment Scale).
Signs below the lesion:
- Loss of all sensory modalities (both posterior column and spinothalamic)
- Upper motor neuron signs (spasticity, hyperreflexia, extensor plantar response/Babinski sign) - develop after initial spinal shock
- Loss of bladder, bowel, and sexual function
- Autonomic dysfunction
Spinal Shock: In the acute phase, there is flaccid paralysis and areflexia below the lesion (despite UMN lesion) due to loss of descending excitatory input to motor neurons. Returns to spasticity over days-weeks.
7B. Brown-Sequard Syndrome (Hemisection of Spinal Cord)
Cause: Penetrating trauma (knife wound), tumor compressing one half, demyelinating lesion
Classic triad:
| Finding | Side | Explanation |
|---|---|---|
| Ipsilateral loss of fine touch, vibration, proprioception (below lesion) | Same side as lesion | Posterior columns decussate in medulla - ipsilateral until then |
| Contralateral loss of pain and temperature (2-3 segments below lesion) | Opposite side to lesion | Spinothalamic tract decussates in cord, 2-3 segments above where fibers entered |
| Ipsilateral UMN weakness (spasticity, Babinski) below lesion | Same side as lesion | Corticospinal tract decussates in medulla - ipsilateral in cord |
| Ipsilateral LMN weakness at the level of lesion | Same side as lesion | Damage to anterior horn cells at the lesion level |
| Ipsilateral band of hyperesthesia just above lesion | Same side | Irritation of entering dorsal root fibers |
Clinical Pearl: Pure Brown-Sequard is rare; more commonly a "Brown-Sequard Plus" pattern is seen.
7C. Anterior Cord Syndrome (Anterior Spinal Artery Syndrome)
Cause: Occlusion of the anterior spinal artery; anterior cord compression (e.g., burst fracture)
Structures affected: Anterior 2/3 of cord - spinothalamic tracts, corticospinal tracts, anterior horns
Clinical features:
- Bilateral loss of pain and temperature below the lesion (both spinothalamic tracts)
- Bilateral motor weakness (UMN below; LMN at level)
- PRESERVED: Fine touch, vibration, and proprioception (posterior columns supplied by posterior spinal arteries are SPARED)
7D. Posterior Cord Syndrome
Cause: Posterior spinal artery occlusion (rare); tabes dorsalis (syphilis); subacute combined degeneration (B12 deficiency)
Structures affected: Posterior columns
Clinical features:
- Loss of ipsilateral proprioception, vibration, fine touch
- Preserved: Pain, temperature, and motor function
- Results in sensory ataxia - wide-based gait, positive Romberg sign (falls when eyes closed)
7E. Central Cord Syndrome
Most common incomplete SCI - usually from hyperextension injury in elderly with spondylosis
Mechanism: The central gray matter and fibers crossing in the anterior commissure are selectively vulnerable to ischemia/edema
Clinical features:
- Bilateral loss of pain and temperature at the level of the lesion (crossing spinothalamic fibers in anterior commissure are damaged) - "cape-like" distribution
- Bilateral weakness: arms > legs (because corticospinal tract is somatotopically organized: arm fibers are more central/medial, leg fibers are more peripheral/lateral)
- Bladder dysfunction (urinary retention)
- Partial preservation of sacral sensation (sacral LCST fibers are peripheral, spared)
7F. Syringomyelia
Cause: Cavity (syrinx) formation within the spinal cord, often cervical; associated with Arnold-Chiari malformation, trauma, tumors
Mechanism: Expanding fluid-filled cavity first destroys the anterior white commissure (crossing spinothalamic fibers), then expands to affect anterior horns and then lateral funiculi
Clinical features (classic):
- Early: Suspended (cape-like) bilateral loss of pain and temperature at the level of the syrinx (crossing spinothalamic fibers in anterior commissure destroyed) - with PRESERVED touch (posterior columns intact). This selective loss of pain/temperature with preserved touch is called dissociated sensory loss.
- As syrinx expands:
- LMN signs at level of lesion (wasting, fasciculations, weakness) due to anterior horn involvement
- UMN signs below due to lateral corticospinal involvement
- Autonomic features: Horner's syndrome (if cervical: ptosis, miosis, anhidrosis) due to damage to the intermediolateral column/descending sympathetic fibers
- Late: Posterior column involvement - proprioceptive loss
The hallmark is the dissociation pattern: Pain and temperature lost, but touch preserved at the affected levels.
7G. Subacute Combined Degeneration of the Spinal Cord (SCD)
Cause: Vitamin B12 deficiency; rarely copper deficiency, nitrous oxide toxicity
Structures affected: Posterior columns AND lateral corticospinal tracts (hence "combined")
Clinical features:
- Posterior column: Proprioceptive loss, vibration loss, sensory ataxia, Romberg positive
- Lateral corticospinal: UMN weakness, hyperreflexia, Babinski sign
- Initially: Absent knee jerks may occur due to associated peripheral neuropathy (LMN), giving a mixed UMN/LMN picture
- Peripheral neuropathy (stocking-glove sensory loss)
7H. Tabes Dorsalis
Cause: Tertiary neurosyphilis; selective degeneration of posterior columns and dorsal roots
Clinical features:
- Severe proprioceptive loss → tabetic gait (high-stepping, stamping gait)
- Positive Romberg sign
- Loss of vibration and joint position sense
- Lancinating (lightning) pains (sudden, severe, brief pains in limbs/trunk)
- Charcot's joints (neuropathic arthropathy due to proprioception loss)
- Loss of deep tendon reflexes (dorsal root involvement)
- Argyll Robertson pupils (miosis, irregular, no reaction to light but react to accommodation)
7I. Amyotrophic Lateral Sclerosis (ALS)
Cause: Progressive degeneration of BOTH upper and lower motor neurons
Classical mixed UMN + LMN picture:
- UMN signs: Spasticity, hyperreflexia, Babinski, pseudobulbar palsy
- LMN signs: Fasciculations, muscle wasting, weakness
- Bulbar signs: Dysarthria, dysphagia (corticobulbar involvement)
- Sensory spared (pure motor system disease)
- The coexistence of UMN and LMN signs in the same muscle group is the diagnostic hallmark
7J. Conus Medullaris Syndrome vs. Cauda Equina Syndrome
Conus Medullaris (lesion at S1-S5 levels of cord):
- Mixed UMN + LMN bladder (hyperreflexic initially, then flaccid)
- Saddle anesthesia (S2-S5 dermatomes)
- Erectile dysfunction
- Absent bulbocavernosus reflex
- Relatively preserved lower limb strength
Cauda Equina (below conus - LMN roots only):
- Pure LMN: Flaccid paralysis, areflexia
- Severe saddle anesthesia
- Urinary retention (overflow incontinence)
- Bilateral sciatica
- Less symmetric pattern than conus
7K. Spinal Cord Compression (Epidural)
Causes: Metastatic tumor, epidural abscess, hematoma, prolapsed disc
Clinical triad (classic):
- Pain (local and radicular)
- Motor weakness (UMN below, LMN at level)
- Sensory loss (posterior column and spinothalamic)
Sensory level: The highest dermatome level at which sensation is impaired. Due to the somatotopic organization of the spinothalamic tract (sacral fibers most lateral), external cord compression classically causes a sacral-sparing pattern initially, while central lesions affect sacral fibers first.
7L. Horner's Syndrome from Spinal Cord Lesion
Mechanism: The descending sympathetic fibers travel in the lateral funiculus through the cervicothoracic cord. Lesions at C8-T2 can disrupt these fibers.
Signs: Ipsilateral ptosis (partial), miosis (pupil constriction), anhidrosis (absence of sweating on that side of the face)
7M. Upper vs. Lower Motor Neuron Lesion - Key Clinical Differences
| Feature | UMN Lesion (Corticospinal) | LMN Lesion (Anterior Horn/Root) |
|---|---|---|
| Tone | Increased (spastic) | Decreased (flaccid) |
| Reflexes | Hyperreflexia | Hyporeflexia/Areflexia |
| Plantar | Extensor (Babinski +) | Flexor (normal) |
| Wasting | Disuse atrophy (mild, late) | Severe neurogenic wasting |
| Fasciculations | Absent | Present |
| Weakness pattern | Pyramidal (flexors in arm, extensors in leg) | Depends on nerve/root distribution |
| Clonus | Present | Absent |
7N. Spinothalamic Tract - Clinical Testing
- Pinprick and temperature testing are used clinically to test the spinothalamic/anterolateral system
- Loss of pain/temperature with preserved touch = dissociated sensory loss → suggests central cord pathology (syrinx) or Brown-Sequard
- The 2-3 segment lag: After a spinal cord lesion, the spinothalamic sensory level is typically 2-3 segments BELOW the actual lesion level (because fibers cross obliquely over 2-3 segments before ascending)
7O. Descending Pain Modulation - Gate Control Theory
The substantia gelatinosa (Lamina II) is the anatomical substrate for gate control of pain:
- Large myelinated fibers (A-beta: carrying touch) activate inhibitory interneurons in lamina II that "close the gate" to pain signals from C fibers
- This is why rubbing a bruised area reduces pain
- Descending pathways from the PAG (via spinomesencephalic tract afferents) and the raphe nuclei release serotonin and enkephalins to suppress pain at lamina I, II, V
- The locus coeruleus descending noradrenergic fibers similarly suppress pain
- This system is the basis for opioid analgesia (mu receptors abundant in laminae I, II, and PAG)
Summary: Tract Quick Reference
| Tract | Column | Modality | 1st Synapse | Decussation Level |
|---|---|---|---|---|
| Spinothalamic | Lateral | Pain, temperature | Dorsal horn (I, V) | Spinal cord (anterior commissure) |
| Spinoreticular | Lateral | Emotional pain | Dorsal horn | Spinal cord |
| Spinomesencephalic | Lateral | Pain modulation | Dorsal horn | Spinal cord |
| Posterior column (gracilis) | Posterior | Vibration, proprioception, fine touch (T7-sacral) | Nucleus gracilis (medulla) | Medulla (internal arcuate) |
| Posterior column (cuneatus) | Posterior | Same (T6-cervical) | Nucleus cuneatus (medulla) | Medulla (internal arcuate) |
| Dorsal spinocerebellar | Lateral | Unconscious proprioception (leg) | Clarke's column (C8-L3) | None (ipsilateral) |
| Ventral spinocerebellar | Lateral | Unconscious proprioception (leg) | Spinal border cells | Crosses twice (net ipsilateral) |
| Lateral corticospinal | Lateral | Voluntary movement (contralateral limbs) | - | Pyramidal decussation (medulla) |
| Anterior corticospinal | Anterior | Bilateral axial muscles | - | Segmental (anterior commissure) |
| Vestibulospinal (lateral) | Anterior | Balance, extensor tone | - | None (ipsilateral) |
| Reticulospinal (pontine) | Anterior | Extensor facilitation | - | Mostly ipsilateral |
| Reticulospinal (medullary) | Lateral/Anterior | Extensor inhibition | - | Bilateral |
| Tectospinal | Anterior | Head-eye reflexes | - | Dorsal tegmental decussation |
| Rubrospinal | Lateral | Flexor facilitation (arm) | - | Ventral tegmental decussation |
| Fasciculus proprius | Perigraymatter | Intersegmental coordination | - | Variable (both) |
Gray's Anatomy for Students, Neuroanatomy through Clinical Cases 3rd Ed, Medical Physiology (Boron & Boulpaep), Adams & Victor's Principles of Neurology 12th Ed
This is a shared conversation. Sign in to Orris to start your own chat.