Drugs of parkison
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content. Let me compile the full answer from all the textbook data gathered.
Drugs of Parkinson's Disease
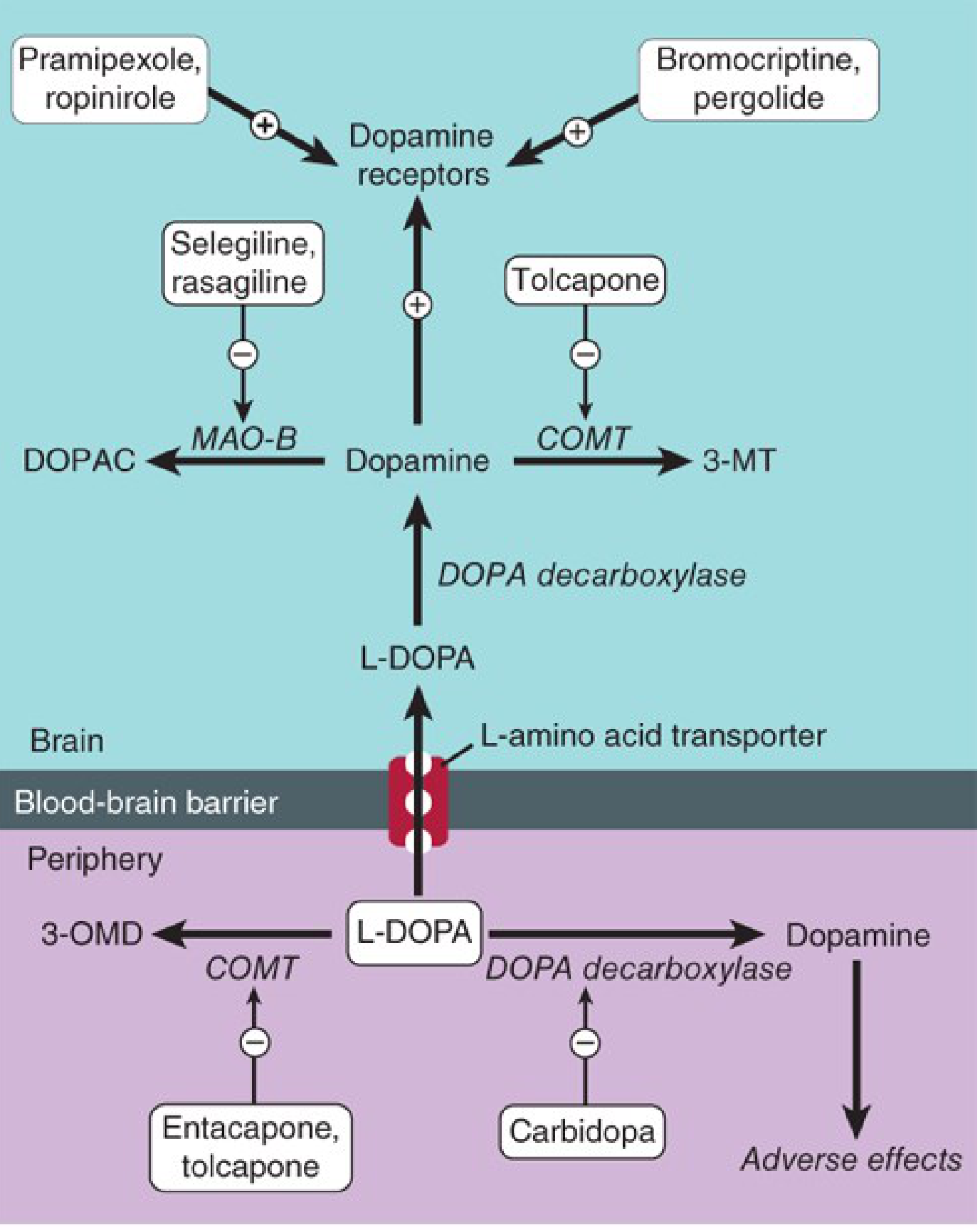
Pathophysiological Basis: Parkinson's disease results from selective loss of dopaminergic neurons in the substantia nigra pars compacta, causing dopamine depletion in the striatum. Normally, dopaminergic neurons inhibit GABAergic striatal output while cholinergic neurons excite it. Loss of dopamine tips this balance toward cholinergic dominance - bradykinesia, rigidity, and tremor result.
This diagram from Katzung's Pharmacology shows the key sites of drug action:
DRUG CLASSES AT A GLANCE
| Class | Examples | Mechanism |
|---|---|---|
| Dopamine precursor | Levodopa + Carbidopa | Replenishes dopamine |
| Dopamine agonists | Pramipexole, Ropinirole, Rotigotine | Directly stimulate D2/D3 receptors |
| MAO-B inhibitors | Selegiline, Rasagiline, Safinamide | Block dopamine breakdown |
| COMT inhibitors | Entacapone, Tolcapone, Opicapone | Block levodopa/dopamine metabolism |
| Anticholinergics | Trihexyphenidyl, Benztropine | Reduce cholinergic excess |
| NMDA antagonist | Amantadine | Reduces dyskinesias |
| Adenosine A2A antagonist | Istradefylline | Novel adjunct for "off" periods |
1. LEVODOPA (+ Carbidopa)
The gold standard and most effective drug for Parkinson's disease.
- Mechanism: Dopamine itself cannot cross the blood-brain barrier. Levodopa (L-DOPA), its precursor, crosses via the L-amino acid transporter (LAT) and is decarboxylated to dopamine in the brain.
- Why combine with carbidopa? Carbidopa is a peripheral DOPA decarboxylase inhibitor that cannot cross the blood-brain barrier. It prevents peripheral conversion of levodopa to dopamine, thereby:
- Reducing peripheral side effects (nausea, vomiting, hypotension)
- Increasing the fraction of levodopa reaching the brain
- Allowing a 75% dose reduction of levodopa
- Brand names: Sinemet (carbidopa/levodopa), Rytary (extended-release)
Adverse Effects of Levodopa
| Category | Effects |
|---|---|
| GI | Nausea, vomiting (early, peripheral) |
| Cardiovascular | Postural hypotension, arrhythmias |
| Dyskinesias | Chorea, athetosis, dystonia (peak-dose; after 2-5 yrs of therapy in ~50%) |
| Motor fluctuations | "Wearing-off," "on-off" phenomenon |
| CNS | Confusion, hallucinations, psychosis, vivid dreams |
| Endocrine | Darkening of urine, inhibits prolactin |
Motor Complications
- Wearing-off (end-of-dose akinesia): Benefit duration shortens; symptoms worsen before next dose
- On-off phenomenon: Unpredictable, abrupt swings between mobility ("on") and immobility ("off")
- Management of fluctuations: Increase dose frequency, use controlled-release preparations, add COMT inhibitor, add MAO-B inhibitor, or consider continuous intestinal gel infusion
Key point: Levodopa does not alter disease progression, but it is the most effective symptomatic treatment even after 20+ years. - Goldman-Cecil Medicine
2. DOPAMINE RECEPTOR AGONISTS
Act directly on striatal dopamine receptors without requiring conversion. Benefits:
- Lower risk of dyskinesias compared to levodopa (non-pulsatile stimulation)
- Useful as initial monotherapy (especially in younger patients <65 yrs)
- Used adjunctively when levodopa response fluctuates
Non-ergot Agonists (Preferred)
| Drug | Receptor | Notes |
|---|---|---|
| Pramipexole | D3 > D2 | Oral; also approved for restless legs syndrome; may cause impulse control disorders |
| Ropinirole | D2, D3 | Oral; similar to pramipexole |
| Rotigotine | D1-D5 | Transdermal patch; useful for continuous delivery |
| Apomorphine | D1+D2 | Subcutaneous injection; used as "rescue" for sudden off episodes |
Ergot Agonists (Less used / Avoided)
- Bromocriptine: D2 agonist; rarely used now
- Pergolide: D1+D2 agonist; withdrawn from US market due to valvular heart disease (fibrotic reactions)
- Cabergoline: Long-acting; similar cardiac valvulopathy risk
Adverse Effects of Dopamine Agonists
- Nausea, postural hypotension, somnolence ("sleep attacks" while driving!)
- Psychiatric: hallucinations, psychosis, confusion (more than levodopa)
- Impulse control disorders (gambling, hypersexuality, binge eating) - specific to non-ergot agonists
- Peripheral edema
- Contraindicated in psychotic illness, recent MI, active peptic ulcer
3. MAO-B INHIBITORS
Monoamine oxidase B selectively metabolizes dopamine in the brain. Inhibiting it prolongs dopamine action.
| Drug | Dose | Use |
|---|---|---|
| Selegiline (deprenyl) | 5 mg BID (breakfast + lunch) | Adjunct to levodopa; some monotherapy use |
| Rasagiline | 1 mg/day (monotherapy); 0.5-1 mg/day (adjunct) | More potent than selegiline; possible neuroprotective role |
| Safinamide | 50 mg → 100 mg once daily | Adjunct only; also has glutamate-modulating activity |
- Selegiline is metabolized to amphetamine metabolites - can cause insomnia (avoid evening dosing), anxiety
- Rasagiline is not metabolized to amphetamine; cleaner profile
- All three: do not combine with meperidine, tramadol, SSRIs, TCAs (risk of serotonin syndrome), or non-selective MAO inhibitors
4. COMT INHIBITORS (Catechol-O-Methyltransferase Inhibitors)
COMT is a major enzyme for degrading levodopa peripherally (to 3-O-methyldopa / 3-OMD) and dopamine centrally. COMT inhibitors extend the half-life of levodopa and reduce "wearing-off."
| Drug | Site of Action | Notes |
|---|---|---|
| Entacapone | Peripheral COMT only | 200 mg with each levodopa dose; most used; combined pill = Stalevo (carbidopa/levodopa/entacapone) |
| Tolcapone | Peripheral + Central COMT | More effective; risk of fatal hepatotoxicity - requires liver monitoring |
| Opicapone | Peripheral COMT | Once-daily; newer agent; no hepatotoxicity concern |
- Adverse effects: worsening levodopa side effects (dyskinesias, nausea, hallucinations), diarrhea, orange discoloration of urine
- Tolcapone: black-box warning for fulminant hepatic failure - restrict use
5. ANTICHOLINERGICS (Antimuscarinic Agents)
Reduce the relative cholinergic excess that results from dopamine depletion in the striatum.
| Drug | Notes |
|---|---|
| Trihexyphenidyl | Most commonly used; oral |
| Benztropine | Also used IV/IM in drug-induced parkinsonism |
| Biperiden | Less commonly used |
- Best for: Tremor (less effective for bradykinesia and rigidity)
- Most useful in: Drug-induced parkinsonism, younger patients with tremor-predominant disease
- Adverse effects: Dry mouth, urinary retention, constipation, blurred vision, confusion, memory impairment, hallucinations
- Avoid in: Elderly (cognitive side effects), patients with dementia, prostatic hypertrophy, glaucoma
6. AMANTADINE
Originally an antiviral drug, found to have anti-parkinsonian properties.
- Mechanism: NMDA glutamate receptor antagonist; also enhances dopamine release and has mild anticholinergic properties
- Uses:
- Mild early Parkinson's disease (modest benefit)
- Reduces levodopa-induced dyskinesias (primary current use)
- Extended-release form (Gocovri) is FDA-approved specifically for dyskinesias
- Adverse effects: Livedo reticularis, leg edema, confusion, hallucinations
- Eliminated renally - reduce dose in renal impairment
7. NEWER/ADJUNCT AGENTS
Istradefylline
- Adenosine A2A receptor antagonist
- Approved as adjunctive therapy with levodopa/carbidopa to reduce "off" time
- Mechanism: A2A receptors modulate dopamine signaling in basal ganglia; blocking them enhances dopaminergic tone
- Adverse effects: Dyskinesias, dizziness, nausea
Apomorphine (rescue)
- Potent D1+D2 agonist; subcutaneous injection (or sublingual film - Kynmobi)
- Acts within minutes; used for sudden, unpredictable "off" episodes
- Must pretreat with antiemetic (trimethobenzamide, NOT domperidone with certain preparations)
TREATMENT STRATEGY SUMMARY
Early disease (mild symptoms)
├── Age <65 years, cognitively intact
│ → Start dopamine agonist (pramipexole/ropinirole)
│ OR MAO-B inhibitor (rasagiline) if very mild
│
└── Age >65 years OR cognitive dysfunction OR severe disability
→ Start Levodopa/Carbidopa (Sinemet)
Motor fluctuations develop
→ Add COMT inhibitor (entacapone)
→ Add MAO-B inhibitor (rasagiline/selegiline)
→ Add dopamine agonist
→ Consider extended-release levodopa (Rytary)
→ Apomorphine for rescue
Dyskinesias develop
→ Reduce levodopa dose + add dopamine agonist
→ Add amantadine
→ Consider deep brain stimulation (DBS)
DRUGS TO AVOID IN PARKINSON'S DISEASE
These drugs worsen Parkinson's or cause drug-induced parkinsonism:
- Antipsychotics (haloperidol, phenothiazines) - block D2 receptors
- Metoclopramide - dopamine blocker
- Reserpine, tetrabenazine - deplete monoamines
- Non-selective MAO inhibitors combined with levodopa - hypertensive crisis
Sources:
- Katzung's Basic and Clinical Pharmacology, 16th Edition, Chapter 28 (Pharmacology of Parkinson Disease)
- Goldman-Cecil Medicine, 2-Vol Set, Chapter 378 (Parkinson Disease - Medical Treatment)
This is a shared conversation. Sign in to Orris to start your own chat.