Trans colonic sepsis spread
Reading File
Finding Sources
Finding Sources
Searching PubMed
colonic perforation sepsis spread peritonitis
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
bacterial translocation gut colon sepsis
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
I now have thorough content to give a comprehensive answer. Here is the full response:
Trans-Colonic Sepsis Spread
"Trans-colonic spread" refers to the various mechanisms by which infection originating within the colon - or the colonic lumen - crosses the bowel wall to cause local, regional, or systemic sepsis. There are two distinct but related concepts: bacterial translocation (microorganisms crossing an intact mucosa) and transmural spread following perforation/breach of the colonic wall.
1. Mechanisms of Trans-Colonic Sepsis Spread
A. Bacterial Translocation (Intact Wall)
Under normal conditions, the colonic mucosa acts as a barrier preventing luminal bacteria from entering the systemic circulation. This barrier can be breached by:
- Increased mucosal permeability - from ischemia, obstruction, inflammation, trauma, or critical illness
- Disrupted tight junctions between enterocytes
- Failure of local immunity (IgA secretion, gut-associated lymphoid tissue)
Once translocation occurs, gram-negative enteric organisms (Enterobacteriaceae - E. coli, Klebsiella) and anaerobes (Bacteroides fragilis) enter the mesenteric lymphatics and portal venous system, seeding the liver and systemic circulation.
Key drivers include:
- Bowel obstruction - even simple small or large bowel obstruction causes bacterial translocation (Deitch EA, 1989)
- Severe acute pancreatitis - intestinal permeability is markedly increased, with endotoxemia suggesting gut translocation as the mechanism of infectious necrosis
- Enteral starvation - reduces IgA, promotes bacterial adhesion, and promotes translocation (this is why early enteral feeding is preferred over parenteral nutrition in the ICU)
- Hepatic cirrhosis - translocation of gram-negative bacteria from the colon is central to the pathophysiology of spontaneous bacterial peritonitis (SBP); prophylaxis targets selective intestinal decontamination of gram-negative flora
B. Transmural Perforation - The Hinchey Spectrum
The most dramatic form of trans-colonic sepsis spread follows breach of the full thickness of the bowel wall. The Hinchey classification (and its modified Wasvary version) describes the progressive stages of sepsis spread from colonic perforation, most commonly in diverticular disease:
| Stage | Description | Sepsis Pattern |
|---|---|---|
| 0 | Mild clinical diverticulitis, no perforation | Contained |
| Ia | Colonic wall thickening / confined pericolic inflammation | Phlegmon, no free pus |
| Ib | Confined pericolic or mesocolic abscess (<5 cm) | Localized spread |
| II | Pelvic, distant intra-abdominal, or retroperitoneal abscess | Regional spread |
| III | Generalized purulent peritonitis | Free pus in peritoneum - systemic sepsis |
| IV | Generalized fecal peritonitis | Free fecal contamination - severe sepsis/shock |
Hinchey III results when an occult diverticular perforation with pericolic abscess ruptures into the peritoneum, releasing purulent material. Hinchey IV denotes a free perforation of a diverticulum with direct fecal contamination of the peritoneal cavity. Clinically, Hinchey III and IV cannot be reliably distinguished without surgical exploration.
- Current Surgical Therapy, 14th ed. and Schwartz's Principles of Surgery, 11th ed.
2. Pathophysiology - How Spread Occurs
The process from localized colonic infection to systemic sepsis:
- Mucosal inflammation / microperforation - bacteria leak into pericolic fat (peridiverticulitis)
- Pericolic phlegmon / abscess formation - contained by mesentery and omentum (Hinchey I-II)
- Abscess rupture or free perforation - pus or feces enter the peritoneal cavity (Hinchey III-IV)
- Peritonitis - the peritoneum becomes a massive absorptive surface for endotoxin and bacteria
- Systemic bacteremia and endotoxemia - triggers SIRS/sepsis cascade (cytokines, complement, coagulation)
- Multi-organ dysfunction - if not controlled
In colonic cancer obstruction, a closed-loop obstruction causes massive bowel distension leading to ischemia of the wall, then perforation and peritonitis with the same consequence.
3. Microbiology
The colonic flora responsible for trans-colonic sepsis are predominantly:
- Gram-negatives: E. coli, Klebsiella, Proteus, Enterobacteriaceae
- Anaerobes: Bacteroides fragilis (major contributor to abscess formation)
- Antibiotic coverage must include gram-negative AND anaerobic organisms
4. Clinical Presentations
| Condition | Mechanism | Result |
|---|---|---|
| Acute diverticulitis (perforated) | Direct transmural perforation | Pericolic abscess → peritonitis |
| Colorectal cancer obstruction | Ischemia → perforation | Fecal peritonitis |
| Ischemic colitis | Mucosal necrosis → transmural spread | Peritonitis, systemic sepsis |
| Colonic volvulus (sigmoid/cecal) | Closed-loop → strangulation | Perforation, peritonitis |
| Cirrhosis / SBP | Bacterial translocation through intact wall | Ascitic fluid infection |
| Critical illness / ICU | Barrier dysfunction + translocation | Bacteremia, sepsis without perforation |
| Severe acute pancreatitis | Increased permeability + translocation | Infected pancreatic necrosis |
5. Management Algorithm (Perforated Diverticulitis)
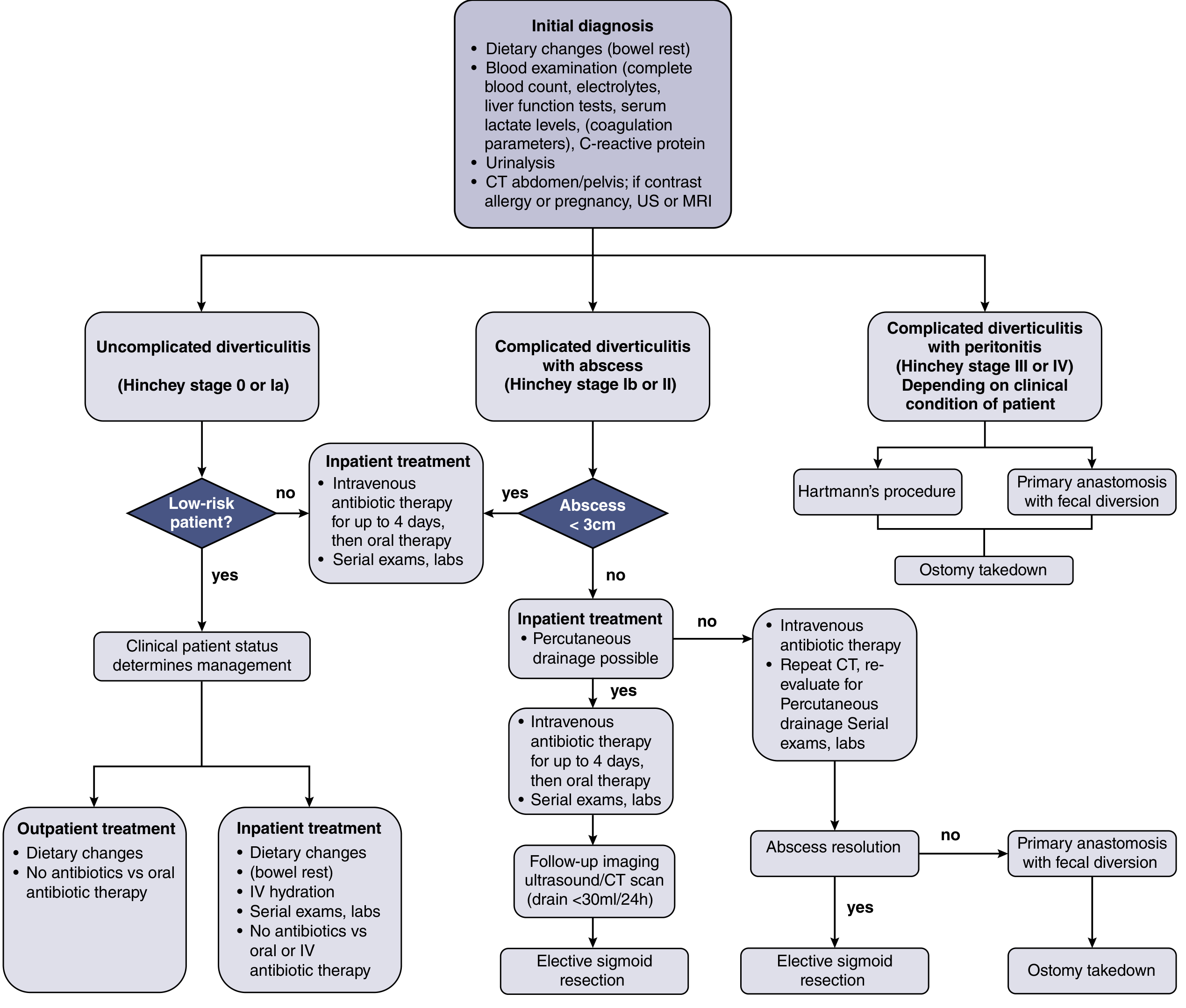
Current Surgical Therapy, 14th ed. - Evidence-based management algorithm
Key surgical principles for Hinchey III/IV:
- Emergency laparotomy with abdominal exploration
- Resection of the perforated colonic segment + thorough peritoneal lavage
- Two options: (1) Resection + primary anastomosis ± proximal loop-ileostomy, or (2) Hartmann's procedure (end colostomy + rectal stump)
- The DIVA arm of the LADIES trial showed primary anastomosis yields significantly higher 12-month stoma-free survival (95% vs. 72%) compared to Hartmann's procedure in perforated diverticulitis, with no difference in morbidity/mortality
- Laparoscopic lavage alone is not recommended for Hinchey III/IV (LOLA trial showed higher morbidity in the lavage arm)
- 30-day mortality after emergency colectomy is ~5.1% overall, rising to up to 53% with 2+ risk factors (age >80, ASA 4-5, creatinine >1.2, albumin <2.5)
Prevention of translocation-mediated sepsis:
- Early enteral nutrition - maintains intestinal barrier, stimulates IgA, prevents bacterial adhesion
- Prophylactic antibiotics (e.g., norfloxacin/rifaximin) in cirrhosis for SBP prophylaxis - targeting gram-negative decontamination
- Timely relief of bowel obstruction before mucosal ischemia progresses to full-thickness necrosis
Sources:
- Current Surgical Therapy, 14th ed. (Diverticular Disease with Perforation/Peritonitis)
- Schwartz's Principles of Surgery, 11th ed. (Inflammatory Complications - Diverticulitis)
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease (SBP Prophylaxis; Diverticulitis)
- Mulholland & Greenfield's Surgery, 7th ed. (Bacterial Translocation in Gut Obstruction)
- Fischer's Mastery of Surgery, 8th ed. (Colorectal Cancer Obstruction; Nutrition/Translocation)
This is a shared conversation. Sign in to Orris to start your own chat.