
Screenshot_20260711_210444_WPS Office.jpg
Exam oriented answers super
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Continue
Here are your complete exam-oriented answers for all topics from the image:
⭐⭐⭐⭐⭐ NEONATAL JAUNDICE
A) Define Physiological Jaundice in a Newborn
Definition: Physiological jaundice is a transient, self-limiting unconjugated hyperbilirubinemia occurring in healthy term neonates due to the immaturity of the hepatic bilirubin conjugation system.
Features:
- Appears after 24 hours of birth (never before)
- Peaks at 3rd-4th day in term; 5th-7th day in preterm
- Disappears by 10th day in term; 14th day in preterm
- Total serum bilirubin does not exceed 12 mg/dL in term (15 mg/dL in preterm)
- Direct (conjugated) bilirubin < 2 mg/dL
- Baby is otherwise healthy - feeds well, no signs of illness
Mechanism (causes):
- Increased bilirubin load - fetal Hb breakdown (HbF has shorter RBC lifespan ~70-90 days vs. 120 days in adults)
- Immature hepatic uptake (↓ ligandin/Y protein)
- Decreased UDP-glucuronosyltransferase activity (conjugation enzyme)
- Increased enterohepatic circulation (↑ intestinal beta-glucuronidase)
- Lack of gut flora
B) Causes of Pathological Jaundice
Pathological jaundice = jaundice appearing within FIRST 24 HOURS or any time with features of pathology
| Category | Causes |
|---|---|
| Increased production | Hemolytic disease of newborn (Rh/ABO incompatibility), G6PD deficiency, spherocytosis, sepsis |
| Decreased conjugation | Crigler-Najjar syndrome (type I & II), Gilbert syndrome, hypothyroidism |
| Obstructive / Direct | Biliary atresia, neonatal hepatitis, choledochal cyst, Alagille syndrome |
| Metabolic | Galactosemia, tyrosinemia, alpha-1-antitrypsin deficiency, Wilson disease |
| Infections | TORCH infections, neonatal sepsis, UTI |
| Polycythemia | Twin-to-twin transfusion, maternal-fetal transfusion |
C) Pathological vs Physiological Jaundice
| Feature | Physiological | Pathological |
|---|---|---|
| Onset | After 24 hrs | Within 24 hrs |
| Duration | < 10 days (term) | > 10-14 days |
| Bilirubin rise | < 5 mg/dL/day | > 5 mg/dL/day |
| Peak bilirubin | < 12 mg/dL | > 12 mg/dL |
| Direct bilirubin | < 2 mg/dL | > 2 mg/dL (conjugated) |
| General condition | Well, feeding normally | Sick, lethargic, poor feeding |
| Pallor/hepatosplenomegaly | Absent | May be present |
| Requires treatment | Usually no | Yes |
D) Approach to a Child with Jaundice
History:
- Time of onset, duration, progression
- Family history (hemolytic disease, metabolic disorders)
- Maternal blood group, Rh status
- Dark urine, pale stools (cholestasis?)
- Feeding history, infections (sepsis)
Examination:
- Assess extent: face → trunk → limbs → palms/soles (Kramer's zones - higher zone = higher bilirubin)
- Pallor (hemolysis), hepatosplenomegaly (hemolysis/infection/metabolic)
- Signs of sepsis, dysmorphic features
- Neurological: lethargy, high-pitched cry, opisthotonus (bilirubin encephalopathy)
Investigations:
- Serum bilirubin (total, direct, indirect)
- Blood group - mother and baby (ABO/Rh incompatibility)
- DCT (Direct Coombs Test) - for hemolytic disease
- CBC - anemia, polycythemia
- Peripheral smear - spherocytes, fragmented cells
- Reticulocyte count - elevated in hemolysis
- G6PD assay
- LFTs, TORCH screen, TFTs as indicated
- Urine - reducing substances (galactosemia)
Kramer's Zones (clinical estimate):
| Zone | Area | Approx. Bilirubin |
|---|---|---|
| 1 | Face | 5 mg/dL |
| 2 | Trunk | 9 mg/dL |
| 3 | Below umbilicus | 11 mg/dL |
| 4 | Limbs | 13 mg/dL |
| 5 | Palms/Soles | >15 mg/dL |
E) Treatment of Unconjugated Hyperbilirubinemia
1. Phototherapy (First line)
- Mechanism: Light converts unconjugated bilirubin to water-soluble lumirubin (photoisomers) - excreted in bile/urine without conjugation
- Wavelength: 430-490 nm (blue-green spectrum)
- Indications (AAP guidelines): Based on hour-specific nomogram (bilirubin level + age in hours + risk factors)
- Technique: Naked baby (covered eyes + genitals), turn 2-hourly, monitor temperature, continue feeds
- Intensive phototherapy: Multiple lights, bili-blanket; used when bilirubin rises rapidly
2. Exchange Transfusion (When phototherapy fails or bilirubin critically high)
- Indications:
- Bilirubin approaching exchange level on nomogram
- Signs of acute bilirubin encephalopathy
- Hemolytic disease with rapid rise (> 0.5 mg/dL/hr)
- Procedure: Double-volume exchange (2 × 80 mL/kg = 160 mL/kg) via umbilical vein catheter
- Purpose: Removes antibody-coated RBCs + bilirubin + maternal antibodies
- Complications: Hypocalcemia, hypoglycemia, thrombocytopenia, NEC, air embolism, infection
3. Pharmacological (Adjuncts)
- IV Immunoglobulin (IVIG): 0.5-1 g/kg for isoimmune hemolytic jaundice - reduces hemolysis
- Phenobarbitone: Induces UGT enzyme - used in Crigler-Najjar type II
- Tin-mesoporphyrin: Inhibits heme oxygenase (experimental)
- Adequate hydration + feeding: Reduces enterohepatic circulation
4. Treat Underlying Cause
- Antibiotics for sepsis, thyroid hormone for hypothyroidism, etc.
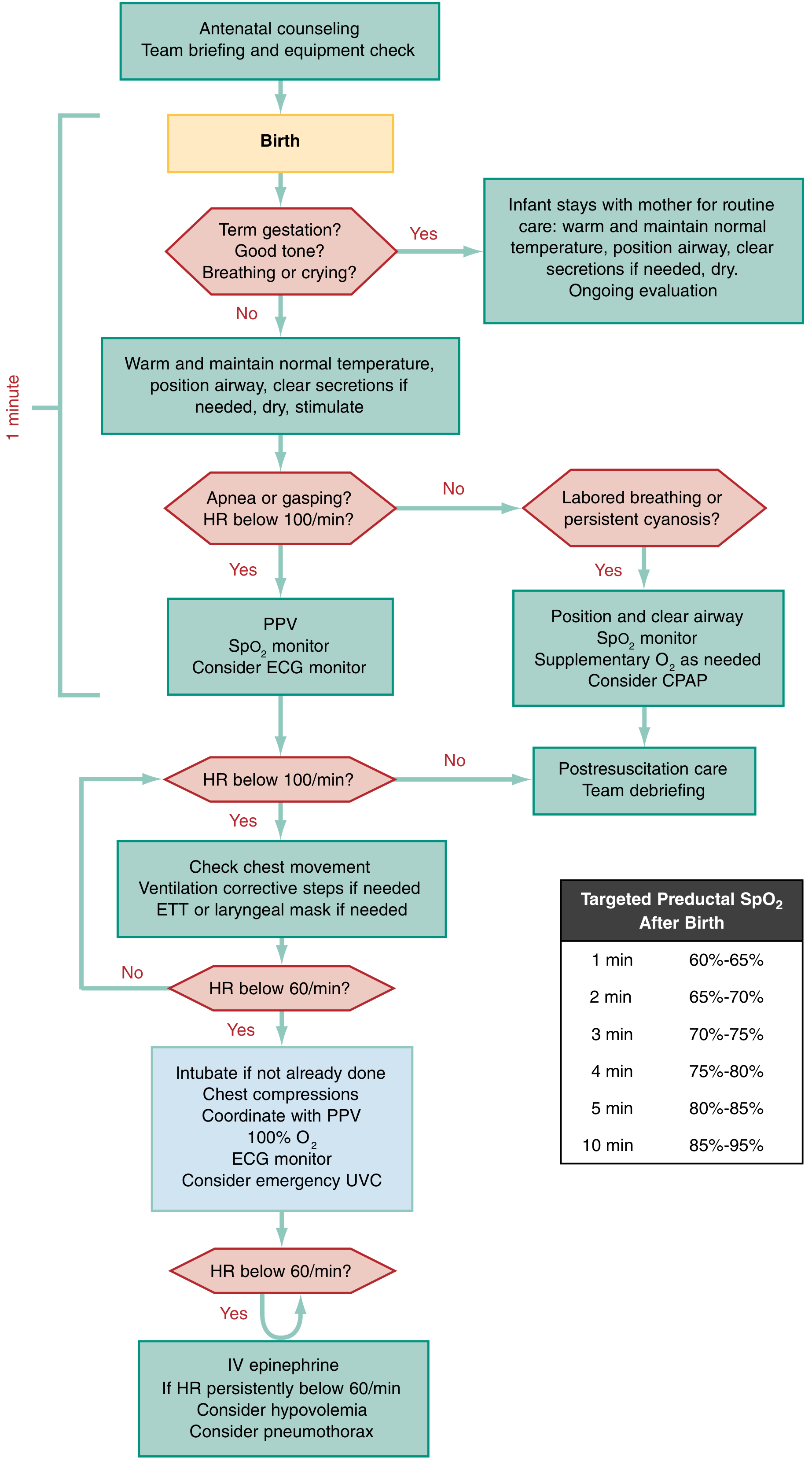
⭐⭐⭐⭐⭐ RESUSCITATION OF NEWBORN AT BIRTH
Steps of Resuscitation (NRP - Neonatal Resuscitation Program)
PRE-BIRTH PREPARATION
- Antenatal counseling, team briefing, equipment check
- Warm radiant warmer, suction, oxygen, bag-mask, ET tubes, medications ready
STEP 1: Initial Assessment (First 30-60 seconds - "Golden Minute")
Ask 3 questions at birth:
- Term gestation?
- Good muscle tone?
- Breathing or crying?
If ALL YES → Baby stays with mother; routine care (warm, dry, position airway)
If ANY NO → Proceed with resuscitation
STEP 2: Initial Steps (0-60 seconds)
- Warm - place under radiant warmer (prevent hypothermia)
- Position - neck slightly extended ("sniffing position")
- Clear airway - suction mouth first, then nose (if secretions or meconium)
- Dry and stimulate - flick soles, rub back
- Reposition - reassess airway
Meconium-stained liquor: Only suction trachea with ETT if baby has poor tone, poor respiratory effort, or HR < 100 after 1 min PPV
STEP 3: Assess - Breathing and Heart Rate
- Breathing: Normal, labored, or apneic?
- Heart Rate (HR): Best assessed by auscultation or 3-lead ECG
- HR ≥ 100 + breathing well → Post-resuscitation care
- Labored breathing / cyanosis → CPAP + SpO₂ monitor
- Apnea or HR < 100 → PPV
STEP 4: Positive Pressure Ventilation (PPV)
- Indications: Apnea, gasping, HR < 100/min
- Rate: 40-60 breaths/min ("breathe-two-three, breathe-two-three")
- Pressure: 20-25 cm H₂O (first breaths may need 30-40 cm H₂O)
- O₂: Start with room air (21%) in term babies; adjust via SpO₂
- Reassess HR after 30 seconds of PPV
Targeted Preductal SpO₂ after birth:
| Time | Target SpO₂ |
|---|---|
| 1 min | 60-65% |
| 2 min | 65-70% |
| 3 min | 70-75% |
| 4 min | 75-80% |
| 5 min | 80-85% |
| 10 min | 85-95% |
STEP 5: If HR Still < 100 after PPV
- Check chest movement - ventilation corrective steps (MR SOPA: Mask adjustment, Reposition, Suction, Open mouth, Pressure increase, Airway - intubate)
- Consider ETT or laryngeal mask insertion
STEP 6: If HR < 60 despite adequate ventilation
- Intubate (if not already done)
- Chest compressions: 3:1 ratio (3 compressions : 1 breath) = 90 compressions + 30 breaths/min
- Technique: Two-thumb encircling method (preferred) OR two-finger method
- Depth: 1/3 of AP chest diameter
- Switch to 100% O₂
- Insert UVC (umbilical vein catheter)
- ECG monitoring
STEP 7: Medications (if HR < 60 despite compressions + ventilation)
- Epinephrine (Adrenaline):
- IV (UVC): 0.01-0.03 mg/kg (1:10,000 solution)
- ET route: 0.05-0.1 mg/kg (higher dose via ET)
- Normal saline 10 mL/kg - if hypovolemia suspected
- Consider pneumothorax (needle decompression)
APGAR Score (assessed at 1, 5, 10 minutes)
| Sign | 0 | 1 | 2 |
|---|---|---|---|
| Heart rate | Absent | < 100 | ≥ 100 |
| Respirations | Absent | Slow, irregular | Good, crying |
| Muscle tone | Limp | Some flexion | Active |
| Reflex irritability | None | Grimace | Cough/sneeze |
| Color | Blue/pale | Pink body, blue extremities | Completely pink |
- Score 7-10: Normal
- Score 4-6: Moderate depression - stimulate, supplemental O₂
- Score 0-3: Severe depression - immediate resuscitation
Neonatal Resuscitation Algorithm:
⭐⭐⭐ PRETERM BABY
Define Preterm Baby
Definition: A baby born before 37 completed weeks of gestation (< 37 weeks), regardless of birth weight.
Classification:
| Type | Gestational Age |
|---|---|
| Extremely preterm | < 28 weeks |
| Very preterm | 28-32 weeks |
| Moderate preterm | 32-34 weeks |
| Late preterm | 34-37 weeks |
Factors Affecting Prematurity (Risk Factors)
Maternal Factors
- Previous preterm birth (strongest predictor)
- Pre-eclampsia / hypertension
- Antepartum hemorrhage (placenta previa, abruption)
- Infections: UTI, bacterial vaginosis, chorioamnionitis
- Uterine anomalies (bicornuate, septate uterus)
- Cervical incompetence
- Multiple gestation (twins, triplets)
- Assisted reproductive technology (ART/IVF)
- Extremes of age (< 18 years, > 35 years)
- Malnutrition, smoking, drug/alcohol use
- Diabetes mellitus, thyroid disease
- Short inter-pregnancy interval (< 18 months)
Fetal Factors
- Multiple gestation
- Fetal anomalies
- Polyhydramnios
- IUGR
Placental / Uterine Factors
- Preterm/prelabor rupture of membranes (PPROM)
- Placental insufficiency
Complications of Preterm Baby
Respiratory
- Respiratory Distress Syndrome (RDS) / Hyaline Membrane Disease - due to surfactant deficiency (most important)
- Bronchopulmonary Dysplasia (BPD) - chronic lung disease
- Apnea of prematurity - due to immature respiratory center
- Pulmonary hypoplasia
Cardiovascular
- Patent Ductus Arteriosus (PDA) - failure of ductus to close
- Hypotension
- Bradycardia
CNS (Most feared long-term complications)
- Intraventricular Hemorrhage (IVH) - germinal matrix bleed
- Periventricular Leukomalacia (PVL) - white matter injury
- Cerebral palsy
- Attention deficit disorders
- Sensorineural hearing loss
Gastrointestinal / Metabolic
- Necrotizing Enterocolitis (NEC) - ischemic bowel necrosis (serious)
- Feeding difficulties / dysmotility / reflux
- Hypoglycemia - poor glycogen stores
- Hypocalcemia, hyponatremia
Eyes
- Retinopathy of Prematurity (ROP) - abnormal retinal vascularization from O₂ exposure
Skin / Temperature
- Hypothermia - thin skin, lack of brown fat, large surface area to body weight ratio
- Excessive insensible water loss
Immune / Hematological
- Increased sepsis/meningitis - immature immune system, no maternal IgG (transferred after 34 wks)
- Anemia of prematurity - short RBC lifespan + insufficient erythropoietin
Metabolic Bone Disease
- Osteopenia of prematurity - inadequate calcium/phosphorus stores
⭐⭐⭐⭐⭐ LOW BIRTH WEIGHT AND SMALL FOR DATE
A) Definitions
| Term | Definition |
|---|---|
| Low Birth Weight (LBW) | Birth weight < 2500 g regardless of gestational age |
| Very Low Birth Weight (VLBW) | Birth weight < 1500 g |
| Extremely Low Birth Weight (ELBW) | Birth weight < 1000 g |
| Small for Gestational Age (SGA) | Birth weight < 10th percentile for gestational age and sex |
| Intrauterine Growth Restriction (IUGR) | Rate of fetal growth less than normal potential; birth weight < 3rd, 5th or 10th percentile, or > 2 SD below mean for gestational age |
| Large for Gestational Age (LGA) | Birth weight > 90th percentile |
| Appropriate for Gestational Age (AGA) | Birth weight between 10th-90th percentile |
Types of IUGR:
| Type | Features |
|---|---|
| Symmetrical IUGR (20-30%) | All parameters reduced - weight, length, HC; early insult (< 20 wks); fewer cells; causes: TORCH, chromosomal, congenital malformations |
| Asymmetrical IUGR (70-80%) | Weight reduced > length > head (brain-sparing); late insult (> 28 wks); fewer fat cells; causes: uteroplacental insufficiency (most common), maternal hypertension, diabetes, smoking |
| Intermediate IUGR (5-10%) | Combined; insult at 20-28 weeks |
B) Known Causes of IUGR
Maternal Causes (Most common)
- Hypertension / Pre-eclampsia - uteroplacental insufficiency
- Malnutrition - maternal undernutrition
- Chronic diseases: Renal disease, SLE, severe diabetes, cardiac disease, thyroid disease
- Smoking (small placentas - high risk)
- Alcohol, drug abuse
- Anemia (severe)
- Multiple gestation
Placental Causes
- Placental insufficiency, infarction, abruption
- Circumvallate placenta
- Single umbilical artery
Fetal Causes
- Chromosomal abnormalities (aneuploidy - 25% of severe early IUGR)
- TORCH infections (Toxoplasma, Rubella, CMV, Herpes, Syphilis)
- Congenital malformations
- Multiple gestation
C) Complications Anticipated in Full-term LBW (IUGR) Neonate
Immediate / Short-term
| System | Complication |
|---|---|
| Metabolic | Hypoglycemia (most common - depleted glycogen), hypocalcemia, hypomagnesemia |
| Temperature | Hypothermia - poor fat stores, large surface area |
| Respiratory | Birth asphyxia, meconium aspiration syndrome (MAS) - chronic fetal hypoxia leads to meconium passage |
| Hematological | Polycythemia (compensatory from chronic hypoxia) → hyperviscosity syndrome |
| Renal | Oliguria, reduced nephron number |
| Immune | Increased susceptibility to infections |
| Feeding | Feeding difficulties, poor suck |
Long-term Complications
- Neurodevelopmental delay - cerebral palsy, learning disabilities
- Growth failure - many remain short
- Barker Hypothesis / DOHaD (Developmental Origins of Health and Disease):
- IUGR babies have increased risk of hypertension, type 2 diabetes, coronary artery disease, obesity, metabolic syndrome in adult life (fetal programming)
D) Steps to Prevent Complications in Full-term LBW Neonate
At Delivery
- Skilled birth attendant; warm delivery room
- Anticipate and prepare for resuscitation
- Delayed cord clamping (1-3 minutes) - reduces anemia
Temperature Management (Prevent Hypothermia)
- Dry immediately, place under radiant warmer
- Kangaroo Mother Care (KMC) - skin-to-skin contact
- Warm clothing, cap, socks
- Target temperature: 36.5-37.5°C (axillary)
Feeding (Prevent Hypoglycemia)
- Early initiation of breastfeeding within 30 minutes of birth
- Exclusive breastfeeding - monitor blood glucose
- Blood glucose monitoring at 30 min, 1hr, 2hr, 6hr, 12hr of life
- Treat hypoglycemia (BG < 45 mg/dL): IV dextrose 10% 2 mL/kg bolus
Infection Prevention
- Hand hygiene, aseptic technique
- Avoid unnecessary invasive procedures
- KMC improves immune function
- Vaccinations as per schedule
Monitoring
- Daily weight, head circumference, length
- Serial blood glucose, hematocrit
- Monitor for polycythemia (hematocrit > 65%): dilutional exchange transfusion if symptomatic
Polycythemia Management
- Adequate hydration
- Symptomatic polycythemia → partial exchange transfusion with normal saline
Sources: Creasy & Resnik's Maternal-Fetal Medicine; Medical Physiology (Boron); ROSEN's Emergency Medicine; Guyton & Hall Textbook of Medical Physiology
This is a shared conversation. Sign in to Orris to start your own chat.