SLAP LESIOMN
Reading File
Finding Sources
Finding Sources
Searching PubMed
SLAP lesion shoulder labrum
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of SLAP (Superior Labrum Anterior to Posterior) Lesions:
SLAP Lesion — Superior Labrum Anterior to Posterior Tear
Definition
A SLAP lesion is a tear of the superior part of the glenoid labrum, occurring anterior and posterior to the attachment of the long head of the biceps tendon. The superior labrum is more loosely adherent to the glenoid than the anteroinferior labrum, attaching more medially off the glenoid face. SLAP tears account for approximately 5% of all shoulder injuries.
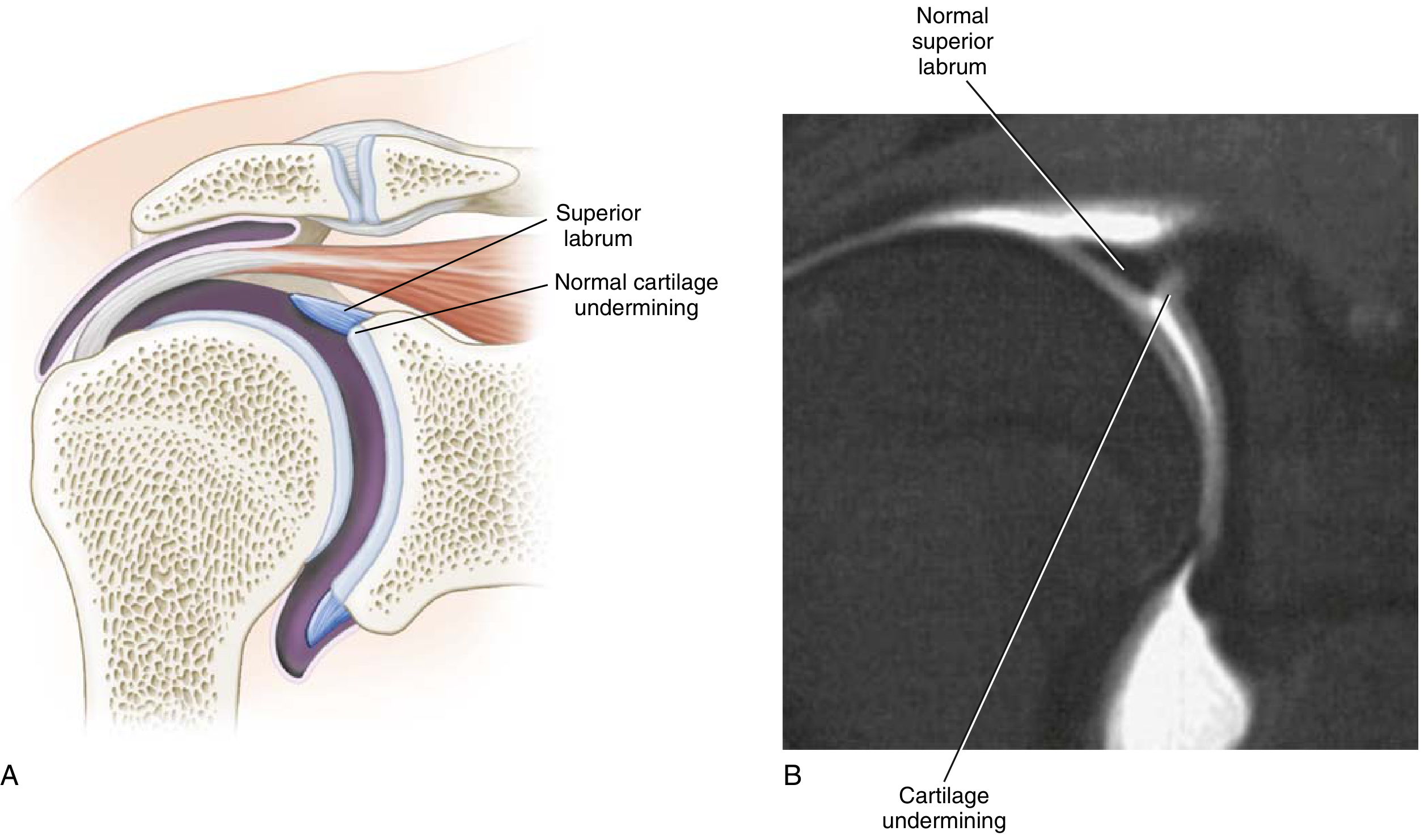
Anatomy Relevant to SLAP
- The biceps tendon has a complex insertion into the superior labrum: ~50% of fibers insert into the superior labrum, ~50% into the supraglenoid tubercle (6.6 mm from the glenoid face at the 12-o'clock position)
- The superior labrum deepens the shoulder socket and anchors the glenohumeral ligaments
Normal anatomic variants that can mimic SLAP pathology:
- Sublabral foramen (recess)
- Sublabral foramen + thickened middle glenohumeral ligament (MGHL) — ~9% of shoulders
- Buford complex — absent anterosuperior labrum + thickened MGHL — ~1.5% of shoulders (attempted repair can cause severe loss of ER)
Mechanism of Injury
- Trauma: fall on outstretched arm (compression), sudden traction/pull, anterior shoulder dislocation
- Repetitive overhead motion: throwing athletes (late cocking phase — "peel-back" phenomenon of the posterosuperior labrum during abduction and external rotation)
- Associated with internal impingement and GIRD (glenohumeral internal rotation deficit)
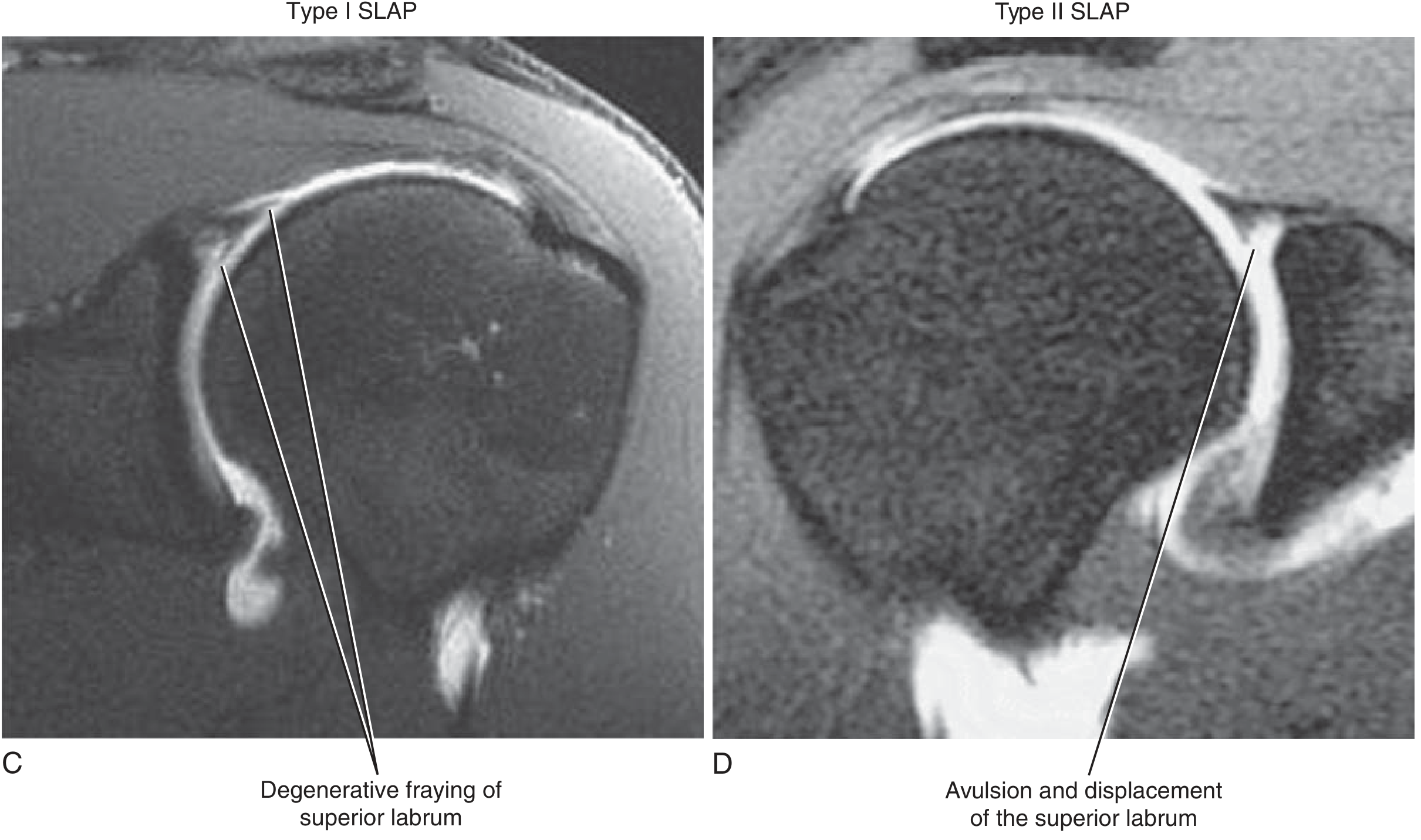
Snyder Classification (Expanded)
| Type | Description | Treatment |
|---|---|---|
| I | Biceps fraying; anchor intact on superior labrum | Arthroscopic débridement |
| II | Detachment of biceps anchor (most common; IIA = anterior, IIB = posterior, IIC = combined) | Repair vs. tenotomy/tenodesis |
| III | Bucket-handle superior labral tear; biceps tendon intact | Arthroscopic débridement |
| IV | Bucket-handle tear extending into biceps tendon | <30% tendon: débridement; >30% tendon: repair or tenodesis |
| V | Bankart labral tear + SLAP lesion | Stabilization of both |
| VI | Superior flap tear | Débridement |
| VII | Capsular injury + SLAP lesion | Repair and stabilization |
Type II is the most common.
MRI Appearance
History & Physical Examination
- Pain may be acute (traumatic) or insidious (repetitive overhead)
- Mechanical symptoms: clicking, catching, locking
- No single test is fully specific for a SLAP tear
Key special tests:
| Test | Technique | Significance |
|---|---|---|
| O'Brien (active compression) | 10° adduction, 90° forward flexion, maximal pronation → resistance | Pain = SLAP or AC joint pathology |
| Compression-rotation test | Axial compression + rotation in abduction | Catching/pain |
| Speed test | Resisted forward flexion with elbow extended, forearm supinated | Biceps tendon involvement |
| Crank test | Axial load + rotation at 160° elevation | Labral tear |
| Kim biceps load test | Seated, arm at 90° abduction, ER; resisted flexion | SLAP |
| Kibler anterior slide test | Hands on hips; axial + forward pressure on elbow | Anterior labrum |
Imaging
- Plain radiographs: evaluate concomitant bony injury or osteoarthritis (generally normal in isolated SLAP)
- MR arthrography (with intra-articular gadolinium) is the modality of choice — adds sensitivity for labral tear detection over standard MRI
- Key MR findings:
- Abnormal morphology or increased signal within or deep to the superior labrum
- Signal irregularity extending lateral to the glenoid or posterior to the biceps tendon = highly suggestive
- Paralabral cyst at the spinoglenoid notch — indicative of SLAP (or posterior labral tear); may compress the suprascapular nerve → infraspinatus wasting
Treatment
Nonoperative (attempt in virtually all patients first)
- Rotator cuff strengthening and scapular stabilization exercises
- Posterior capsule stretching (especially throwers with GIRD — sleeper stretch)
- NSAIDs
- Intraarticular corticosteroid injections
Operative (if conservative management fails)
- Arthroscopic surgery — technique dictated by SLAP type (see table above)
- Intraoperative finding: peel-back phenomenon — posterosuperior labrum detaches with abduction and external rotation
- Type II controversy: Repair vs. tenotomy/tenodesis
- Patients >40 years with biceps pathology + degenerative labral changes → favored: débridement + tenotomy/tenodesis
- Concomitant rotator cuff tears → no proven advantage to repairing SLAP simultaneously; may increase stiffness; newer studies favor biceps tenotomy/tenodesis at time of RCR
Postoperative Rehabilitation
- Sling immobilization ~4 weeks
- Early pendulum exercises to minimize stiffness (high postoperative stiffness rate — one study showed 78%)
- Avoid resistive biceps exercises and ER at 90° abduction early
- Strengthening begins ~4–6 weeks post-op
- Interval throwing program at ~3–4 months post-op
- Persistent stiffness: physical therapy → arthroscopic capsular release if refractory
Complications of SLAP Repair
- Stiffness — most common (up to 78%)
- Persistent pain
- Articular cartilage injury
- Loose or prominent anchor hardware
Sources: Miller's Review of Orthopaedics, 9th Ed.; Schwartz's Principles of Surgery, 11th Ed.
Recent evidence: A 2025 systematic review/meta-analysis (PMID 39914604) confirms high sensitivity and specificity of MR arthrography for labral tears, supporting its role as the primary imaging modality.
This is a shared conversation. Sign in to Orris to start your own chat.