What are different presentation of tongue on physical exam for pet to the point diagnosis or pathnomonic of different types of diseases like inflammatory condition, autoimmune , deficiencies , lilke loss of papillae, inflamed or coated tongue .. according to medicine and dermatolog9cal textbooks and litreture . Give with pictures of each disease
strawberry tongue scarlet fever Kawasaki disease
geographic tongue benign migratory glossitis
oral hairy leukoplakia HIV lateral tongue
oral candidiasis thrush white plaques tongue
fissured tongue lingua plicata scrotal tongue
macroglossia enlarged tongue amyloidosis hypothyroidism
Tongue Examination: Physical Signs & Their Diagnostic Significance
1. STRAWBERRY TONGUE
White Strawberry Tongue → Scarlet Fever (Strep pyogenes)
Red Strawberry Tongue → Kawasaki Disease

Key distinction: White coating = scarlet fever. Pure red without coating = Kawasaki. Both can cause desquamation of palms/soles. Toxic shock syndrome (TSS) also produces strawberry tongue.
2. GEOGRAPHIC TONGUE (Benign Migratory Glossitis)
- Associated with psoriasis (tongue lesions histologically identical to pustular psoriasis)
- Associated with atopy, Reiter syndrome (reactive arthritis)
- Also seen with fissured tongue in 50% of cases
- Reported in AIDS, lithium therapy

3. SMOOTH / ATROPHIC TONGUE (Atrophic Glossitis)

| Cause | Color / Features | Key Clue |
|---|---|---|
| Iron deficiency / Plummer-Vinson | Pale then red, smooth, painful | + dysphagia (esophageal web), koilonychia |
| Vitamin B12 (pernicious anemia) | Beefy-red, smooth, "Hunter's glossitis" | + megaloblastic anemia, subacute combined degeneration |
| Folate deficiency | Erythematous, smooth, swollen | + megaloblastic anemia; no neurologic signs |
| Riboflavin (B2) deficiency | Magenta tongue — purplish-red + cheilosis | + seborrheic dermatitis, angular stomatitis, corneal vascularization |
| Niacin deficiency (Pellagra) | Bright red "beefy" → smooth glazed; tip/sides first; dental imprints | + 4 Ds: Dermatitis, Diarrhea, Dementia, Death |
| Pyridoxine (B6) deficiency | Redness, burning, ulceration → flattened filiform | + similar to niacin deficiency picture |
| Zinc deficiency | Burning mouth, taste loss | + poor wound healing, acrodermatitis |
| Celiac disease | Smooth, atrophic | + iron/folate malabsorption; DH rash |
| Sjögren syndrome | Smooth, dry (xerostomia) | + dry eyes, anti-Ro/La |
| Candidiasis (atrophic) | Smooth, red, painful (median rhomboid) | Median posterior dorsum; responds to antifungals |
| Diabetes mellitus | Smooth, red + angular cheilitis | Recurrent Candida, taste changes |
Sources: Sleisenger & Fordtran's GI Disease; Andrews' Diseases of the Skin; Harrison's 22e; KJ Lee's Otolaryngology
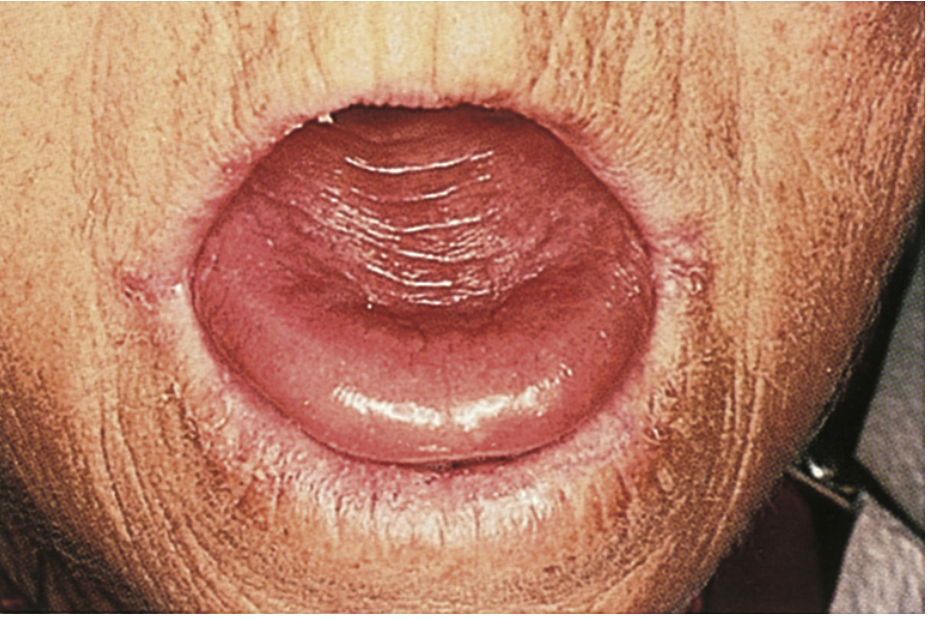
4. FISSURED TONGUE (Lingua Plicata / Scrotal Tongue)
- Melkersson-Rosenthal syndrome (triad: fissured tongue + granulomatous cheilitis + facial nerve palsy) — pathognomonic context
- Associated with Down syndrome, psoriasis, and co-occurs with geographic tongue in 50%

5. BLACK HAIRY TONGUE (Lingua Villosa Nigra)
- Chronic smoking (most common)
- Oral antibiotics (disrupts oral flora → overgrowth of chromogenic bacteria)
- Hydrogen peroxide mouth rinses
- Heavy coffee/tea intake
- Interferon-α therapy (hepatitis C)
- Linezolid, bismuth, psychotropics

Distinguish from oral hairy leukoplakia: OHL is on the lateral tongue, white, adherent, non-scrapable; EBV-driven; marker of HIV/immunosuppression. Black hairy tongue is on the dorsum, scrapes off.
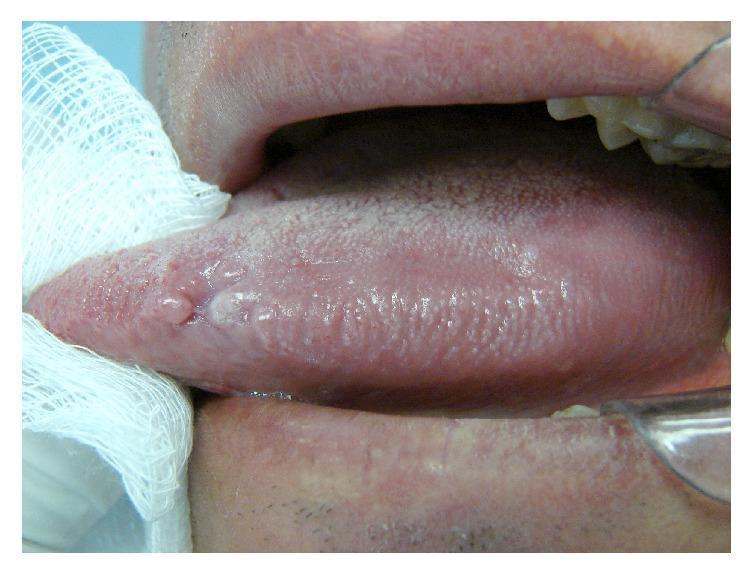
6. ORAL HAIRY LEUKOPLAKIA (OHL)
- Location: lateral tongue borders (bilateral) — key distinguishing feature
- Appearance: shaggy, hairy vertical ridges; adherent — does NOT scrape off (unlike thrush)
- Resolves with HAART
7. ORAL CANDIDIASIS (Pseudomembranous Thrush)

Median rhomboid glossitis = a specific candidal pattern: smooth, oval/rhomboid, erythematous plaque in the midline posterior dorsum — characteristic of chronic atrophic candidiasis.
8. MACROGLOSSIA (Enlarged Tongue)
| Disease | Key Tongue Feature | Associated Findings |
|---|---|---|
| Amyloidosis (AL) | Firm, nodular macroglossia; lateral nodules; ecchymoses | Restrictive cardiomyopathy, periorbital purpura, nephrotic syndrome |
| Hypothyroidism (congenital/adult) | Soft, diffuse macroglossia | Myxedema, hoarseness, bradycardia, delayed reflexes |
| Acromegaly | Macroglossia + teeth spacing | Coarse features, prognathism, large hands/feet |
| Down syndrome | Relative macroglossia + fissuring | Trisomy 21 facies |
| Beckwith-Wiedemann | True macroglossia from birth | Omphalocele, organomegaly, hypoglycemia |
| Angioedema | Acute swelling | Urticaria, allergy, ACE inhibitor use |

9. SUMMARY TABLE: Point-to-Point Diagnosis
| Tongue Finding | Pattern | Diagnose / Consider |
|---|---|---|
| White strawberry tongue | White coat + prominent papillae | Scarlet fever (GAS) |
| Red strawberry tongue | Red + prominent papillae, no coat | Kawasaki disease, TSS |
| Map-like wandering patches | Erythema + white borders, migratory | Geographic tongue (psoriasis, atopy) |
| Smooth, beefy-red, painful | Loss of all papillae | B12/folate/iron deficiency, pernicious anemia |
| Magenta tongue | Purple-red + cheilosis + seborrhea | Riboflavin (B2) deficiency |
| Bright red beefy → smooth glazed | Tip/sides first, dental imprints | Pellagra (niacin deficiency) |
| Smooth + dry tongue | Atrophic ± painful | Sjögren syndrome, xerostomia |
| Smooth triad: anemia + dysphagia | Atrophic + smooth | Plummer-Vinson syndrome |
| Central oval red patch (posterior dorsum) | Median rhomboid | Chronic atrophic candidiasis |
| White curd plaques (scrapable) | Pseudomembrane, red base | Oral candidiasis (thrush) |
| White corrugated lateral tongue (non-scrapable) | Hairy vertical ridges, bilateral lateral | Oral hairy leukoplakia (HIV/EBV) |
| Black/brown elongated papillae (dorsum) | Hairy-looking central dorsum | Black hairy tongue (antibiotics, smoking) |
| Deep fissures + furrowing | Central + branching grooves | Melkersson-Rosenthal (with cheilitis + facial palsy) |
| Firm nodular enlargement | Macroglossia + ecchymoses | AL Amyloidosis |
| Soft enlarged + smooth | Macroglossia + myxedema | Hypothyroidism |
| Enlarged + coarse features | Macroglossia + prognathism | Acromegaly |
Clinical Pearl on Deficiencies
- B2 (riboflavin) → magenta tongue (purple-red) — most specific color sign
- B3 (niacin/pellagra) → beefy-red → smooth glazed + 4 Ds
- B6 (pyridoxine) → overlaps niacin deficiency
- B12 + folate → Hunter's glossitis (smooth, red, painful) with megaloblastic anemia
- Iron → smooth pale-then-red tongue, often with angular cheilitis and koilonychia
Sources: Andrews' Diseases of the Skin (9780323547536); Fitzpatrick's Dermatology; Harrison's Principles of Internal Medicine 22e; Sleisenger & Fordtran's GI Disease; Goldman-Cecil Medicine; KJ Lee's Essential Otolaryngology; Basic Medical Biochemistry 6e
Give the typical features and picture of tongue in each case of specific condition and deficiency.. get from every medical and dermatological litreture and textbook ,