Cellular adaptation patho
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Reading File
I now have rich, detailed content from Robbins & Cotran covering all major cellular adaptations. I also have the key flowchart image. Let me now compile a comprehensive answer.
Cellular Adaptations in Pathology
Adaptations are reversible changes in cell size, number, phenotype, metabolic activity, or function in response to altered physiological or pathological stimuli. They represent attempts by the cell to achieve a new steady state while preserving viability. If the stress exceeds adaptive capacity, the cell moves toward injury and death.
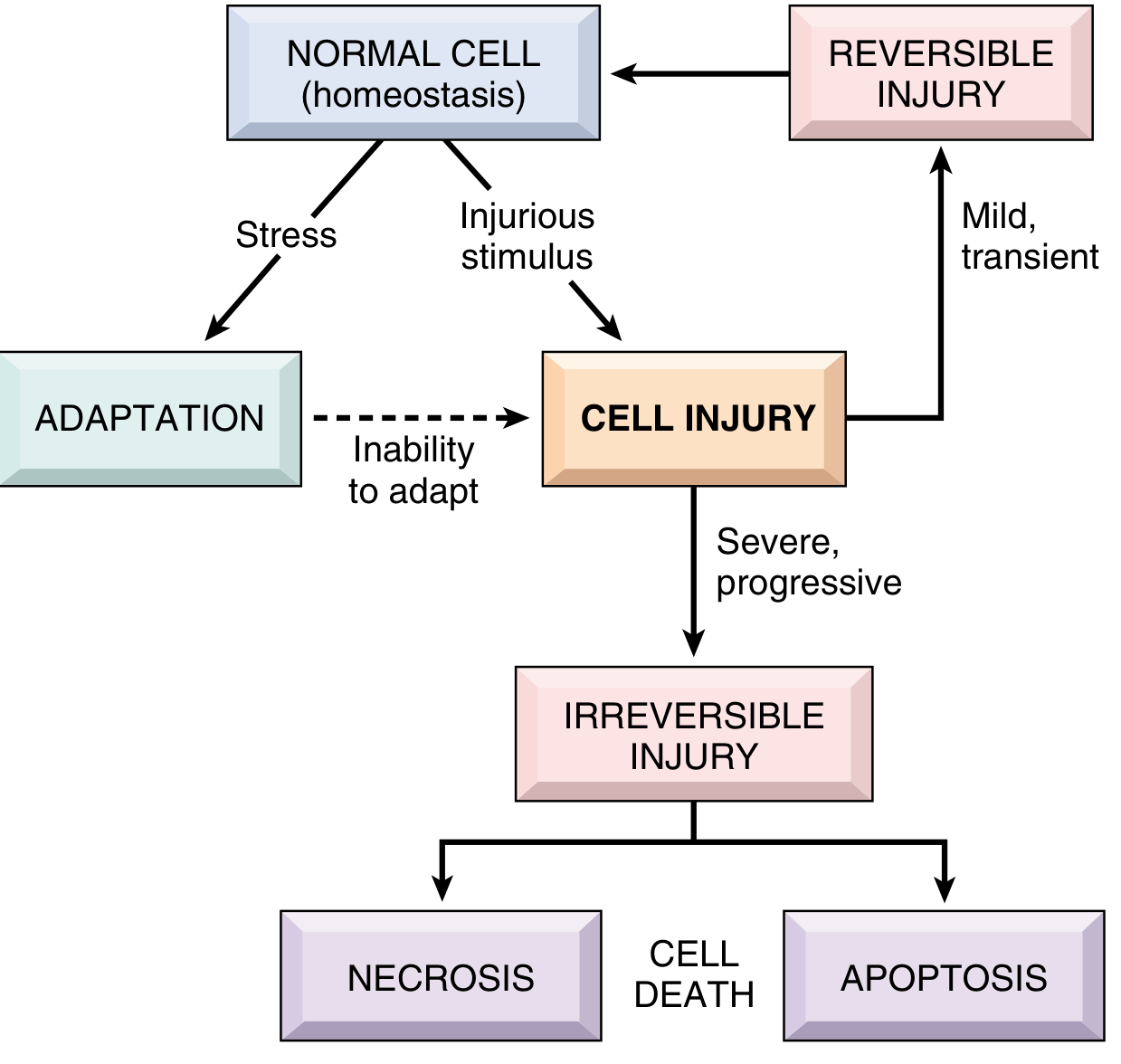
Overview: Spectrum of Cellular Responses
| Stimulus | Cell Response |
|---|---|
| Mild, transient stress | Adaptation (reversible) |
| Severe/persistent stress | Cell injury -> reversible then irreversible |
| Irreversible injury | Necrosis or apoptosis (cell death) |
1. Hypertrophy
Definition: Increase in cell size (not number), resulting in increased organ size. No new cells - just larger cells with more structural components.
Types:
| Type | Example |
|---|---|
| Physiologic | Uterine smooth muscle during pregnancy (estrogen-driven); skeletal muscle with exercise |
| Pathologic | Cardiac hypertrophy from hypertension or valvular disease; bladder hypertrophy from outflow obstruction |
Which tissues?
Occurs in cells with limited capacity for division (e.g., cardiac myocytes, skeletal muscle). Dividing cells may show both hypertrophy AND hyperplasia simultaneously.
Mechanisms of Hypertrophy (cardiac model):
- Mechanical sensors in the cell detect increased load
- Activate downstream signaling via:
- PI3K/AKT pathway - more important in physiologic (exercise-induced) hypertrophy
- G-protein-coupled receptor pathways - more important in pathologic hypertrophy
- Stimulate growth factors: TGF-beta, IGF-1, FGF, and vasoactive agents (alpha-adrenergic agonists, endothelin-1, angiotensin II)
- These activate transcription factors: GATA4, NFAT, MEF2 -> increase expression of contractile protein genes
- Gene switching: alpha-myosin heavy chain --> beta-myosin heavy chain (slower, more energy-efficient contractions - a fetal isoform)
- Atrial natriuretic factor (ANF) expression increases -> compensatory salt excretion + BP reduction
The Limit of Hypertrophy:
When hypertrophy reaches a limit, regressive changes occur: loss of myofibrils, myocyte death -> cardiac failure. This is how a beneficial adaptation becomes maladaptive.
2. Hyperplasia
Definition: Increase in cell number in an organ or tissue. Requires cells capable of division (or stem cells).
Types:
Physiologic Hyperplasia:
- Hormonal: Breast glandular epithelium at puberty/pregnancy; endometrial proliferation after menstruation
- Compensatory: Liver regeneration after partial hepatectomy (experimental liver resection shows near-complete regeneration within 2 weeks)
Pathologic Hyperplasia:
- Endometrial hyperplasia - excess estrogen stimulation (e.g., anovulatory cycles); can progress to endometrial carcinoma
- Benign prostatic hyperplasia (BPH) - DHT-driven stromal + glandular hyperplasia -> urinary obstruction
- Epidermal warts - HPV-induced squamous epithelial hyperplasia
Key point: Pathologic hyperplasia is controlled proliferation (unlike neoplasia); removing the stimulus usually stops it. However, it creates a fertile ground for malignant transformation.
Mechanisms of Hyperplasia:
- Driven by growth factors acting on surviving cells or tissue stem cells
- In liver regeneration: hepatocytes, biliary cells, and vascular cells all proliferate under signals including hepatocyte growth factor (HGF), EGF, TNF, and IL-6
- HPV-associated hyperplasia: viral proteins E6 and E7 inactivate p53 and Rb tumor suppressors
3. Atrophy
Definition: Decrease in cell size AND/OR number, with reduced metabolic activity. The organ shrinks.
Causes:
| Cause | Example |
|---|---|
| Disuse | Skeletal muscle atrophy in a limb cast |
| Denervation | Lower motor neuron lesion -> muscle wasting |
| Loss of blood supply (ischemia) | Brain atrophy in atherosclerosis |
| Inadequate nutrition | Cachexia in cancer/starvation |
| Loss of endocrine stimulation | Post-menopausal uterine/breast atrophy; adrenal atrophy after steroid withdrawal |
| Pressure | Parenchymal atrophy from tumor compression |
| Physiologic aging | Brain, testes |
Types:
- Physiologic atrophy: e.g., thyroglossal duct, notochord, and other embryonic structures involuting after birth
- Pathologic atrophy: any of the causes above
Mechanisms of Atrophy:
- Reduced protein synthesis (decreased anabolic activity)
- Increased protein degradation via the ubiquitin-proteasome pathway - atrophying muscle shows increased ubiquitin ligases (atrogin-1/MAFbx and MuRF1)
- Autophagy - autophagosomes engulf and digest organelles via lysosomal fusion; this is adaptive during nutrient deprivation
- Autophagic vacuoles may leave lipofuscin granules (yellow-brown "wear-and-tear" pigment)
- In some atrophies, apoptosis contributes to cell number reduction
Atrophy is often reversible if the stimulus is corrected early (e.g., re-innervation, restored nutrition).
4. Metaplasia
Definition: Reversible change of one differentiated cell type to another, usually in response to chronic irritation. This is not direct conversion but rather reprogramming of stem cell differentiation.
Common Examples:
| Site | Normal Epithelium | Metaplastic Epithelium | Stimulus |
|---|---|---|---|
| Bronchi | Pseudostratified ciliated columnar | Squamous (stratified) | Cigarette smoking |
| Esophagus (Barrett's) | Stratified squamous | Intestinal columnar with goblet cells | Acid reflux (GERD) |
| Endocervix | Columnar | Squamous | Chronic irritation |
| Bladder | Transitional | Squamous | Chronic calculi/infection |
| Stomach | Gastric mucosa | Intestinal (goblet cells) | H. pylori, chronic gastritis |
Types:
- Squamous metaplasia - most common; squamous replaces columnar/transitional in chronic irritation
- Columnar metaplasia - columnar replaces squamous (Barrett's esophagus is the prime example)
Mechanisms of Metaplasia:
- Reprogramming of tissue stem cells by altered signaling (e.g., retinoids control squamous vs. columnar differentiation)
- In the bronchus: loss of vitamin A signaling -> squamous metaplasia
- Transcription factor switching (e.g., CDX2 in intestinal metaplasia of stomach)
Clinical Significance:
- Metaplastic epithelium is better adapted to the hostile environment
- BUT it loses the original specialized functions (e.g., loss of bronchial cilia impairs mucociliary clearance)
- Most importantly: metaplasia is a pre-malignant state
- Squamous metaplasia in bronchi -> squamous cell carcinoma of lung
- Barrett's esophagus -> esophageal adenocarcinoma
- Intestinal metaplasia of stomach -> gastric adenocarcinoma
5. Dysplasia (Related Concept)
Definition: Disordered cellular growth with loss of uniformity and architectural orientation. Technically a pre-neoplastic change rather than a true adaptation, but closely linked to metaplasia.
- Features: variation in cell size/shape (pleomorphism), increased nuclei with abnormal mitoses, loss of polarity
- Reversible in early stages; severe dysplasia = carcinoma in situ
Summary Comparison Table
| Adaptation | Change | Mechanism | Reversible? | Example |
|---|---|---|---|---|
| Hypertrophy | ↑ cell size | ↑ protein synthesis (PI3K/AKT, GATA4, MEF2) | Yes | Cardiac hypertrophy in HTN |
| Hyperplasia | ↑ cell number | Growth factors on dividing/stem cells | Yes | Endometrial hyperplasia; liver regeneration |
| Atrophy | ↓ cell size ± number | ↓ protein synthesis + ↑ ubiquitin-proteasome + autophagy | Often | Disuse muscle atrophy |
| Metaplasia | Change in cell type | Stem cell reprogramming | Yes (but risk of malignancy) | Barrett's esophagus; squamous metaplasia in smoker |
Source: Robbins, Cotran & Kumar - Pathologic Basis of Disease, 10th ed., pp. 47-76; Robbins & Kumar - Basic Pathology, p. 16-18
This is a shared conversation. Sign in to Orris to start your own chat.