Congenital heart defects in Adults classification,etiology, pathophysiology,clinical signs and symptoms, diagnosis, differential diagnosis, treatment, complications
Reading File
Finding Sources
Finding Sources
Searching PubMed
"congenital heart disease" AND "adults" AND management
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the material needed for a comprehensive, well-structured answer. Let me compile it.
Congenital Heart Defects in Adults (ACHD)
Epidemiology
Congenital heart defects occur in approximately 1% of births in the United States. An overall adult prevalence of 3 to 4 per 1,000 has been documented. Due to advances in medical and surgical therapy, there are now more adults than children living with congenital heart disease - an estimated 2.4 million people in the US, two thirds of whom are adults. Nearly 300,000 have severe congenital heart disease (a combination of at least two or more abnormalities, typically associated with cyanosis at birth).
- Bicuspid aortic valve: ~2% of the general population; the single most common congenital cardiac anomaly in adults and up to 50% of surgical aortic stenosis cases
- ASD: 30-40% of all ACHD; ostium secundum ASD = 7% of all congenital lesions
- VSD: 15-20% of all congenital lesions (most common in children; high spontaneous closure rates explain lesser adult prevalence)
- PDA: 5-10% of all congenital cardiac lesions in infants
- Pulmonary stenosis / coarctation: 3-10% each
- Tetralogy of Fallot: the most common cyanotic congenital anomaly in adults
Classification
I. By Shunt Direction / Physiology
| Category | Mechanism | Examples |
|---|---|---|
| Left-to-right shunts (Acyanotic) | Volume overload of pulmonary circulation | ASD, VSD, PDA, AVSD |
| Right-to-left shunts (Cyanotic) | Deoxygenated blood enters systemic circulation | Tetralogy of Fallot, Eisenmenger syndrome, Transposition of great arteries, Truncus arteriosus |
| Obstructive lesions | No shunt; outflow tract obstruction | Pulmonary stenosis, Aortic stenosis, Coarctation of the aorta |
| Complex / mixing lesions | Single ventricle or mixing of circulations | Tricuspid atresia, Hypoplastic left heart, Double outlet RV |
II. By Anatomic Complexity (ACC/AHA)
| Complexity | Examples |
|---|---|
| Simple | Native: isolated small ASD, VSD, PDA, mild PS - Repaired: previously ligated PDA, repaired VSD without residua |
| Moderate | AVSD, subvalvular or supravalvular AS, anomalous pulmonary venous return, coarctation, Ebstein anomaly, TOF, Marfan syndrome |
| Great complexity | Eisenmenger syndrome, Fontan circulation, cyanotic lesions (all forms), double-outlet ventricle, congenitally corrected TGA, single ventricle |
III. Anatomic and Physiologic (AP) Classification (Modern)
The modern classification integrates three dimensions, as illustrated below:
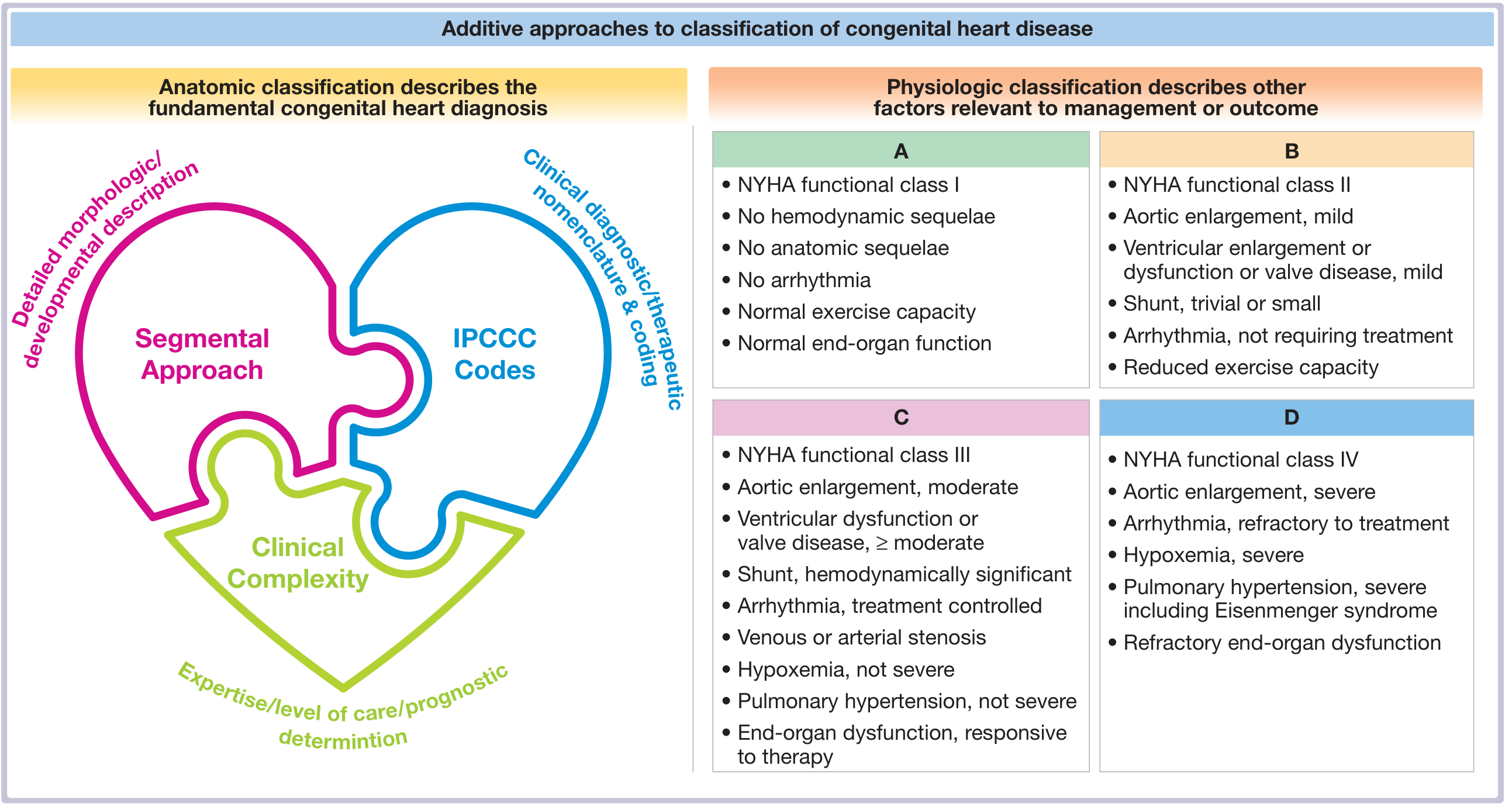
Fuster and Hurst's The Heart, 15th Edition - Anatomic and Physiologic Classification of ACHD
- Anatomic dimension: Segmental approach (situs, connections, ventricular morphology) + IPCCC/ICD-11 coding
- Physiologic dimension (A-D): Grade A (NYHA I, no sequelae) through Grade D (NYHA IV, severe hypoxemia, Eisenmenger, refractory end-organ dysfunction)
Etiology
Genetic Causes (~20% of cases)
- Down syndrome (Trisomy 21): ~50% have endocardial cushion defects and VSD
- Trisomy 13 and 18: VSD in 90%
- Turner syndrome (45,X): Aortic coarctation, aortic stenosis, ASD
- 22q11.2 deletion (DiGeorge / CATCH-22 syndrome): TOF (15%), interrupted aortic arch, truncus arteriosus - shared features: Cardiac defects, Abnormal facies, Thymic hypoplasia, Cleft palate, Hypocalcemia
- Williams syndrome (7q11.23): Supravalvular aortic stenosis
- Noonan syndrome (12q22): Pulmonary stenosis, ASD, hypertrophic cardiomyopathy
- Holt-Oram syndrome (autosomal dominant): ASD + skeletal anomalies
- Marfan syndrome: Aortic root dilation, mitral valve prolapse
Familial / Recurrence Risk
- Mother carrying a sporadic lesion: 2.5-18% recurrence risk (obstructive LVOT lesions highest)
- Father carrying the lesion: 1.5-3%
- Sibling with CHD: 1-3% risk to next sibling
Environmental / Teratogenic Factors
- Maternal rubella infection (PDA, pulmonary stenosis)
- Maternal diabetes (TGA, VSD, coarctation)
- Maternal alcohol use (VSD, ASD)
- Thalidomide, phenytoin, retinoic acid
- Maternal lupus (congenital heart block)
Pathophysiology
1. Left-to-Right Shunts (Acyanotic)
Blood flows from high-pressure left side to lower-pressure right side, creating volume overload of the pulmonary circulation. Chronic left-to-right shunting results in:
- Pulmonary overcirculation → reactive pulmonary vasoconstriction
- Progressive pulmonary arterial hypertension (PAH)
- Eventually, shunt reversal = Eisenmenger syndrome (right-to-left shunt, late cyanosis)
Specific mechanisms:
- ASD: Right atrial and RV volume overload; RV dilates. Large ASD eventually causes RV failure and atrial arrhythmias. Risk of paradoxical embolism (even before Eisenmenger)
- VSD: LV and RV volume overload; pulmonary hypertension develops earlier than in ASD (post-tricuspid shunt). Small VSDs may close spontaneously
- PDA: Aorta-to-pulmonary artery communication; left heart volume overload. Continuous "machinery" murmur
2. Right-to-Left Shunts (Cyanotic)
Deoxygenated blood enters systemic circulation producing central cyanosis, clubbing, and erythrocytosis.
Tetralogy of Fallot: Four components - large VSD + infundibular pulmonary stenosis (RVOTO) + overriding aorta + RVH. Right ventricular outflow obstruction forces deoxygenated blood through the VSD into the aorta. Severity of cyanosis depends on degree of RVOTO.
Eisenmenger Syndrome: End stage of uncorrected large left-to-right shunts (most common: AVSD, VSD, PDA); irreversible PAH raises pulmonary vascular resistance above systemic resistance; shunt reverses to right-to-left. Chronic cyanosis causes:
- Secondary erythrocytosis
- Iron deficiency
- Hyperviscosity
- Paradoxical embolism and cerebrovascular accidents
- Hemoptysis (from pulmonary arteriopathy)
3. Obstructive Lesions
- Pulmonary stenosis: RV pressure overload → RVH → eventual RV failure
- Aortic stenosis: LV pressure overload → LVH → diastolic dysfunction → systolic failure
- Coarctation of the aorta: Proximal hypertension (risk of aortic dissection, rupture, LVH); distal hypoperfusion and collateral formation
4. Complex Lesions
- Transposition of the great arteries (D-TGA): Parallel rather than series circulations; incompatible with life without mixing (ASD/VSD/PDA). Post-atrial switch (Mustard/Senning) operations: systemic RV is at high risk for progressive failure
- Congenitally corrected TGA (CC-TGA): Morphologic RV supports systemic circulation; progressive RV failure + complete heart block are common
- Single ventricle / Fontan circulation: Passive pulmonary blood flow without a subpulmonary ventricle; systemic venous hypertension, protein-losing enteropathy, arrhythmias, liver fibrosis
Clinical Signs and Symptoms
Symptoms (by category)
| Symptom | Common Associations |
|---|---|
| Dyspnea on exertion | ASD, VSD, pulmonary stenosis, TOF post-repair, Eisenmenger |
| Fatigue / reduced exercise tolerance | Any significant ACHD, heart failure |
| Palpitations | Atrial flutter/fibrillation (ASD, Mustard/Senning), VT (TOF) |
| Cyanosis / hypoxemia | Right-to-left shunts, Eisenmenger syndrome |
| Syncope / presyncope | Severe AS, PS, TOF "tet spells," ventricular arrhythmia |
| Chest pain | Coarctation with dissection, anomalous coronary, severe AS |
| Hemoptysis | Eisenmenger syndrome, pulmonary arteriopathy |
| Stroke / TIA | Paradoxical embolism (ASD, PFO, Eisenmenger), erythrocytosis |
| Headache, arthralgia | Erythrocytosis in cyanotic CHD |
Key Physical Signs
General:
- Central cyanosis (lips, tongue, nailbeds) - right-to-left shunts
- Digital clubbing - chronic hypoxemia (TOF, Eisenmenger)
- Differential cyanosis (lower body cyanotic, upper normal) - PDA with Eisenmenger physiology
Cardiovascular Examination:
| Finding | Likely Lesion |
|---|---|
| Widely fixed split S2 | ASD |
| Loud harsh pansystolic murmur at LLSB | VSD |
| Continuous "machinery" murmur | PDA |
| Ejection click + systolic murmur (LUSB) | Pulmonary stenosis or bicuspid AV |
| Harsh systolic murmur at RUSB/carotids | Aortic stenosis |
| Arm-leg BP gradient >20 mmHg | Coarctation of the aorta |
| Holosystolic murmur + displaced apex | Ebstein anomaly (TR) |
| Boot-shaped heart on CXR; RV lift | TOF |
| Loud P2 + right parasternal heave | Pulmonary hypertension / Eisenmenger |
Eisenmenger-specific findings (Braunwald's Heart Disease):
- Central cyanosis and digital clubbing
- Prominent jugular venous a-wave
- Right parasternal heave/lift
- Loud P2
- S3 or S4
- Diastolic murmur of pulmonary regurgitation
- Systolic murmurs may be faint or absent (low-pressure shunt)
Diagnosis
History and Algorithm (Goldman-Cecil Medicine)
The diagnostic evaluation of ACHD should answer three questions:
- What is the native anatomy?
- Has the patient had surgery for the condition?
- What are the residual hemodynamic sequelae?
The key initial branch: cyanotic vs. acyanotic presentation.
Investigations
12-Lead ECG:
- ASD: Right axis deviation, incomplete RBBB, right atrial enlargement; ostium primum → left axis deviation
- VSD: LVH (large VSD), biventricular hypertrophy
- TOF (unrepaired): Right axis deviation, dominant RV forces; post-repair: complete RBBB (80-90%)
- Pulmonary stenosis: Right axis deviation, peaked P waves, R > S in V1 with severe stenosis
- Eisenmenger: Right atrial enlargement, right axis deviation, biventricular hypertrophy, ST-T changes
Chest Radiograph:
- ASD: Cardiomegaly, prominent pulmonary artery, increased pulmonary vascular markings
- VSD: Biventricular enlargement, pulmonary plethora
- TOF: Boot-shaped heart (coeur en sabot) - upturned apex with concave pulmonary artery segment
- Coarctation: Rib notching (collateral vessels), "3-sign" on aortic knob, "E-sign" on barium swallow
- Eisenmenger: Dilated central pulmonary arteries with peripheral "pruning," RV enlargement
Echocardiography (primary imaging modality):
- Transthoracic echo (TTE): Identifies anatomy, shunts (color Doppler), pressure gradients, ventricular function
- Transesophageal echo (TEE): Better definition of ASD morphology, valves, pulmonary veins
- In Eisenmenger: RV enlargement/hypertrophy, pulmonary artery enlargement, low-velocity flow through shunt
Cardiac MRI:
- Gold standard for quantifying RV volumes and function (critical in TOF post-repair)
- Accurately documents distal pulmonary artery stenosis
- Aortic imaging in coarctation and Marfan syndrome
Cardiac Catheterization:
- Reserved for pre-operative/pre-interventional planning
- Measures pulmonary vascular resistance (critical in Eisenmenger)
- Coronary angiography when indicated
Laboratory:
- CBC: Erythrocytosis in cyanotic CHD, thrombocytopenia in Eisenmenger
- Iron studies: Iron deficiency is common in erythrocytosis (impairs RBC function)
- BNP/NT-proBNP: Heart failure marker
- Uric acid: Elevated in Eisenmenger (hyperuricemia)
Differential Diagnosis
| Presentation | ACHD to consider | Non-ACHD differentials |
|---|---|---|
| Young adult cyanosis + clubbing | TOF, Eisenmenger, TGA | Primary pulmonary hypertension, chronic pulmonary disease, methemoglobinemia |
| Dyspnea + wide fixed split S2 | ASD | HFpEF, mitral stenosis, pulmonary embolism |
| Harsh systolic murmur + young adult | Bicuspid AV stenosis, HOCM, PS | Acquired aortic stenosis, HOCM |
| Arm-leg BP gradient + young hypertension | Coarctation of the aorta | Essential hypertension, Takayasu arteritis, renovascular hypertension |
| Cyanosis + erythrocytosis | Cyanotic CHD | Polycythemia vera, secondary polycythemia (COPD, sleep apnea) |
| Palpitations + young adult | ASD (atrial flutter/AF), TOF (VT), Ebstein (WPW) | Idiopathic AF, SVT, accessory pathway |
| Stroke in young adult | PFO/ASD (paradoxical embolism), Eisenmenger | Cardioembolism, thrombophilia, cervical artery dissection |
| Complete heart block | CC-TGA, post-surgical | Acquired AV block, Lyme disease, sarcoidosis |
Treatment
General Principles
All adults with CHD (other than simple, fully repaired lesions without residua) should be followed at specialized ACHD centers. The 2025 ACC/AHA/HRS/ISACHD/SCAI Guidelines (PMID: 41411480) provide the most current recommendations.
Specific Lesion Management
Atrial Septal Defect (ASD)
- Indications for closure: Significant shunt (Qp:Qs ≥1.5:1) with evidence of RV volume overload, or paradoxical embolism. NOT indicated if severe, irreversible pulmonary hypertension (PVR >2/3 systemic)
- Percutaneous device closure: Treatment of choice for ostium secundum ASD with adequate rims; Amplatzer or similar occluder devices
- Surgical closure: For sinus venosus, primum, or coronary sinus ASDs; when device closure not feasible
- Post-procedure: Aspirin for 6 months; endocarditis prophylaxis per guidelines; surveillance for atrial arrhythmias
Ventricular Septal Defect (VSD)
- Small, restrictive VSDs: Annual monitoring; no closure required
- Indications for closure: LV volume overload, prior infective endocarditis, or progressive aortic regurgitation
- Percutaneous or surgical closure depending on location (muscular vs. perimembranous)
Patent Ductus Arteriosus (PDA)
- Closure recommended for any hemodynamically significant PDA
- Percutaneous coil or device occlusion for most
- Surgical ligation for large or complicated PDAs
Pulmonary Stenosis
- Intervention threshold: Mean Doppler gradient ≥30 mmHg + symptoms (or ≥40 mmHg regardless of symptoms) unless moderate/severe pulmonary regurgitation
- Percutaneous balloon valvotomy: Procedure of choice for doming valve; excellent long-term results (>95% 25-year survival)
- Transcatheter pulmonary valve replacement: When valvuloplasty fails or not possible
- Surgical resection: For subvalvular stenosis (double-chambered RV)
Aortic Stenosis (Bicuspid/Congenital)
- Follow guidelines similar to acquired aortic stenosis for intervention thresholds
- TAVR increasingly used; surgical AVR for those unsuitable for transcatheter approach
- Annual surveillance of the aorta is mandatory given bicuspid valve-associated aortopathy
Coarctation of the Aorta
- Intervention: Gradient ≥20 mmHg arm-to-leg at rest, or hypertension with radiological evidence of significant coarctation
- Percutaneous stenting: First-line for most adults (vs. surgical repair in children)
- Balloon angioplasty alone carries risk of re-coarctation and aneurysm
- Lifelong surveillance for hypertension, re-coarctation, and aortic aneurysm
Tetralogy of Fallot
- After childhood repair, ongoing surveillance is mandatory (yearly ACHD specialist review)
- Pulmonary valve replacement (PVR): Indicated when RV pressure >2/3 systemic due to residual RVOTO, or free pulmonary regurgitation with RV dysfunction. ICD should be considered concurrently if arrhythmia burden is high
- Monitor for: Residual PS, pulmonary regurgitation, residual VSD, arrhythmias (atrial flutter, VT), and sudden cardiac death (3-6% over 20-30 years)
- Cardiac MRI is essential for RV volume and function monitoring
Transposition of the Great Arteries (post-Mustard/Senning)
- Systemic right ventricle is at high risk for failure - monitor with MRI and BNP
- Arrhythmia surveillance (sinus node dysfunction, atrial flutter common)
- Heart failure therapy (ACE inhibitors, beta-blockers); transplantation may be needed
Eisenmenger Syndrome
- Contraindicated: Closure of the shunt (irreversible PAH); systemic vasodilators without PAH therapy; inappropriate phlebotomy; pregnancy
- Pulmonary arterial hypertension therapy: Endothelin receptor antagonists (bosentan - most evidence), phosphodiesterase-5 inhibitors (sildenafil), prostacyclin analogs
- Phlebotomy: Only if severe hyperviscosity symptoms AND hematocrit >65%; must replace volume isovolemically; NOT for erythrocytosis without symptoms
- Iron supplementation: Address iron deficiency carefully (may worsen erythrocytosis acutely)
- Anticoagulation: Not routinely recommended due to bleeding risk; consider for specific indications (intracardiac thrombus, atrial arrhythmias)
- Heart-lung transplantation: Definitive option in carefully selected patients
- Avoid: Dehydration, systemic vasodilators, nephrotoxins, air in IV lines (paradoxical embolism)
Infective Endocarditis Prophylaxis
Indicated for:
- Complex cyanotic CHD (unrepaired or residual defects)
- Prosthetic cardiac valves or material
- Repaired CHD with prosthetic material within 6 months (until endothelialized)
- Repaired CHD with residual defects at or adjacent to prosthetic patch/device
Exercise Recommendations
| Condition | Unrestricted | Low-Moderate Intensity | Prohibited |
|---|---|---|---|
| ASD | No PHT, no arrhythmia, normal function | PA pressure >40 mmHg, no arrhythmia | Eisenmenger |
| VSD | Small, no PHT, no arrhythmia | Moderate VSD | Eisenmenger |
| Coarctation | Gradient ≤20 mmHg arm-to-leg, normal BP | Gradient ≥20 mmHg with normal BP/ETT | Gradient ≥50 mmHg or aortic aneurysm |
| Pulmonary stenosis | Gradient <40 mmHg, no arrhythmia | Gradient 40-60 mmHg | Gradient ≥70 mmHg or ventricular arrhythmia |
| Aortic stenosis | Gradient <30 mmHg, normal ECG/ETT | Gradient 30-50 mmHg, asymptomatic | Gradient >50 mmHg or ventricular arrhythmia |
| TOF (repaired) | Normal RV pressure, no shunt, no arrhythmia | Increased RV pressure or moderate PR or SVT | RV pressure ≥65% systemic or VT on ETT |
| Mustard/Senning | - | No cardiomegaly, arrhythmia, or syncope; normal ETT | Cardiomegaly or arrhythmia at rest/exercise |
Complications
Cardiovascular Complications
| Complication | Key Details |
|---|---|
| Arrhythmias | Most common complication overall. Atrial arrhythmias (AF, atrial flutter) - especially ASD, Mustard/Senning, Fontan. VT/VF and sudden cardiac death (3-6% in repaired TOF). Complete AV block in CC-TGA, post-surgical |
| Heart failure | RV failure in Eisenmenger, post-Mustard/Senning (systemic RV), Fontan. LV failure in aortic stenosis, coarctation |
| Pulmonary arterial hypertension | Complication of chronic, uncorrected large left-to-right shunts; Eisenmenger syndrome is the extreme |
| Residual valvular dysfunction | Pulmonary regurgitation post-TOF repair; aortic regurgitation with subaortic stenosis; tricuspid regurgitation in Ebstein |
| Infective endocarditis | High risk in unrepaired defects, prosthetic material, previous endocarditis |
| Aortic complications | Dilation, aneurysm, and dissection in bicuspid aortic valve, coarctation, and Marfan syndrome |
| Coronary artery disease | Superimposed atherosclerosis increases burden; anomalous coronary origins complicate surgical repair |
Hematologic Complications (Cyanotic/Eisenmenger)
| Complication | Mechanism |
|---|---|
| Erythrocytosis | Chronic hypoxemia drives EPO → elevated RBC mass; compensatory, NOT polycythemia vera |
| Iron deficiency | Accelerated erythropoiesis depletes iron; worsens symptoms (headache, fatigue) even without anemia |
| Hyperviscosity syndrome | Elevated hematocrit → headache, blurred vision, fatigue, faintness - distinguish from dehydration |
| Bleeding diathesis | Platelet dysfunction, thrombocytopenia, factor deficiencies; risk of hemoptysis |
| Thromboembolism | Paradoxical embolism (right-to-left shunt), in situ pulmonary thrombosis, cerebrovascular accidents |
| Hyperuricemia / gout | Reduced renal urate excretion due to erythrocytosis and low renal perfusion |
Non-Cardiac Complications
- Renal dysfunction: Chronic reduced renal perfusion in Fontan, cyanotic CHD
- Liver disease / fibrosis: Chronic venous congestion in Fontan circulation; risk of hepatocellular carcinoma
- Protein-losing enteropathy: Fontan circulation (high systemic venous pressure → intestinal protein loss)
- Neurological: Stroke/TIA from paradoxical embolism, brain abscess (right-to-left shunt allows septic emboli to bypass pulmonary filter), cerebral hyperviscosity
- Pregnancy risks: Significantly elevated maternal and fetal mortality in Eisenmenger (maternal mortality 30-50%), Fontan, severe PAH, cyanotic CHD, systemic ventricular dysfunction
- Psychosocial: Depression, anxiety, employment, and insurance barriers are common; transition from pediatric to adult care is a critical vulnerability period
Prognosis
- Simple, repaired ACHD (ASD, small VSD, PS): Near-normal life expectancy
- Repaired TOF: 85% 30-year survival; risk of sudden cardiac death remains
- Eisenmenger syndrome: Death rare in childhood; becomes common after the 4th decade; worse prognosis with pre-tricuspid shunts, lower resting O2 saturations, non-sinus rhythm, and pericardial effusion
- Fontan/single ventricle: Progressive attrition; 5-year transplant-free survival approximately 70-80% at 20 years
- Post-Mustard/Senning (systemic RV): Progressive RV failure is a major long-term concern
Key references:
- Goldman-Cecil Medicine International Edition, Ch. 55 (CONGENITAL HEART DISEASE IN ADULTS)
- Fuster and Hurst's The Heart, 15th Edition, Chs. 65-70 (Adult Congenital Heart Disease section)
- Braunwald's Heart Disease, Ch. 82 (Eisenmenger syndrome)
- 2025 ACC/AHA/HRS/ISACHD/SCAI Guideline for the Management of Adults With Congenital Heart Disease - PMID 41411480 - the most current practice guideline (published February 2026 in JACC and Circulation)
Note: The 2025 ACC/AHA guideline (PMID 41411480) represents a major update to prior recommendations and should be consulted for current class-of-recommendation / level-of-evidence specifics on interventional thresholds and surveillance intervals.
This is a shared conversation. Sign in to Orris to start your own chat.