Juiandance
Asking for Preferences
The input "Juiandance" is unclear. It could be:
- "Jui and dance" — a name and a topic
- A typo for something like "Zui Quan" (Drunken Fist, a Chinese martial arts/dance style), or "line dance," or another dance form
- A person's name combined with "dance"
Could you rephrase or give more context about what you're looking for? I'm happy to help once I understand what you mean.
Anemia
Reading File
Finding Sources
Searching the Web
anemia classification causes diagnosis treatment overview 2024
Reading File
Finding Sources
Searching Images
anemia classification types red blood cells
Reading File
Finding Sources
Searching PubMed
"anemia" AND "diagnosis"
Reading File
Loading Image
Here is a comprehensive overview of Anemia:
Anemia
Definition
Anemia is a reduction in circulating red blood cell (RBC) mass, resulting in decreased oxygen-carrying capacity of the blood. It is diagnosed when:
- Hemoglobin (Hb) < 12–15 g/dL (varies by sex and age)
- Hematocrit (Hct) < 36–45%
- RBC count < 4–6 × 10⁶/µL
The hematocrit is roughly 3× the Hb value, which is roughly 3× the RBC count — a useful bedside rule.
Classification
Anemia is classified by MCV (cell size), RDW (size variation), and Reticulocyte Production Index (RPI):
By MCV (Morphologic Classification)
| MCV | Category | Common Causes |
|---|---|---|
| < 80 fL | Microcytic | Iron deficiency, thalassemia, anemia of chronic disease (ACD) |
| 80–100 fL | Normocytic | Hemolytic anemia, aplastic anemia, renal failure, acute blood loss |
| > 100 fL | Macrocytic | B12/folate deficiency (megaloblastic), hypothyroidism, liver disease |
By Bone Marrow Response (RPI)
| RPI | Response | Examples |
|---|---|---|
| > 3 | Hyperproliferative | Hemolysis, blood loss |
| < 2 | Hypoproliferative | Iron deficiency, aplastic anemia, renal failure |
Common Types & Key Lab Findings
(From Henry's Clinical Diagnosis and Management by Laboratory Methods)
| Type | Cause | Key Lab Abnormalities |
|---|---|---|
| Microcytic hypoproliferative | Iron deficiency | ↓ Ferritin, ↑ TIBC, ↓ serum iron, ↑ RDW |
| Microcytic hypoproliferative | Anemia of chronic disease | ↑ Ferritin (normal/high), ↓ serum iron, normal RDW |
| Normocytic hyperproliferative | Hemolytic anemia | Schistocytes, ↑ reticulocytes, ↓ haptoglobin, ↑ LDH, ↑ indirect bilirubin, ↑ RDW |
| Normocytic hypoproliferative | Aplastic anemia | Pancytopenia, hypocellular marrow, normal RDW |
| Normocytic hypoproliferative | Renal failure | ↑ BUN/creatinine, ↓ EPO, burr cells |
| Macrocytic megaloblastic | B12/folate deficiency | ↓ B12/folate, hypersegmented neutrophils, macro-ovalocytes, ↑ RDW |
| Macrocytic non-megaloblastic | Hypothyroidism | ↑ TSH, normal RDW |
Peripheral Blood Smear: Normal vs. Iron Deficiency Anemia
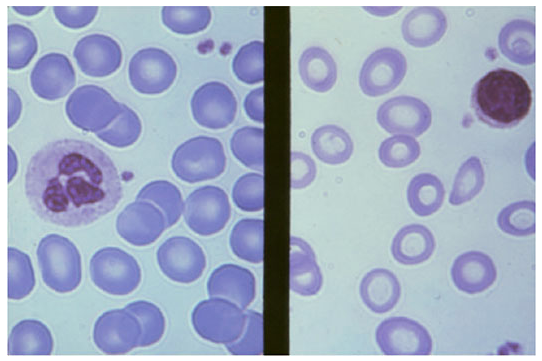
Left: Normal RBCs — uniform size, moderate central pallor. Right: Iron deficiency anemia — smaller cells (microcytic), pale (hypochromic), with markedly increased central pallor. — Harrison's Principles of Internal Medicine, p. 1721
Symptoms
- General: Fatigue, weakness, pallor, dyspnea on exertion
- Cardiovascular: Palpitations, tachycardia, high-output heart failure (severe)
- Neurological (B12 deficiency): Paresthesias, subacute combined degeneration of spinal cord
- Specific: Koilonychia, pica, glossitis (iron deficiency); jaundice, dark urine (hemolysis)
Diagnostic Approach
- CBC — Hb, Hct, MCV, MCH, MCHC, RDW, platelet count
- Peripheral blood smear — morphology (hypochromia, macrocytes, schistocytes, spherocytes)
- Reticulocyte count/RPI — assess marrow response
- Targeted labs based on morphology:
- Microcytic → serum iron, ferritin, TIBC, hemoglobin electrophoresis
- Macrocytic → B12, folate, TSH
- Normocytic → reticulocytes, LDH, haptoglobin, Coombs test, BUN/creatinine
Treatment Principles
| Type | Treatment |
|---|---|
| Iron deficiency | Oral ferrous sulfate 60–120 mg elemental iron/day; IV iron if intolerant or malabsorption |
| B12 deficiency | IM cyanocobalamin or high-dose oral B12 |
| Folate deficiency | Oral folic acid 1 mg/day |
| Anemia of CKD | Erythropoiesis-stimulating agents (ESAs) + iron |
| Hemolytic | Corticosteroids (autoimmune), treat underlying cause |
| Aplastic | Immunosuppression, allogeneic stem cell transplant |
Special Contexts
Pregnancy: Physiologic hemodilution lowers Hb normally (plasma volume ↑47%, RBC mass ↑17%). Hb < 11 g/dL or Hct < 33% is considered non-physiologic. Supplemental iron (30 mg/day) is recommended for all pregnant women; treatment dose is 60–120 mg/day for diagnosed IDA. — Textbook of Family Medicine 9e
Sources: Henry's Clinical Diagnosis and Management by Laboratory Methods; Harrison's Principles of Internal Medicine 21e; Textbook of Family Medicine 9e
This is a shared conversation. Sign in to Orris to start your own chat.