Classification of firearm wounds management of gun shot injury from front of chest
Reading File
Finding Sources
Finding Sources
Searching PubMed
"gunshot wound" AND "chest" AND management
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have very comprehensive information from multiple authoritative textbooks. Let me compile the complete answer.
Classification of Firearm Wounds and Management of Gunshot Injury to the Front of the Chest
I. Classification of Firearm (Gunshot) Wounds
A. By Wound Morphology
1. Entry Wound
- Typically smaller, round/oval with inverted (indrawn) edges
- Surrounded by an abrasion collar (zone of contusion/friction from bullet spin)
- Edges relatively clean and regular
- May have tattooing (stippling) from unburnt gunpowder in close-range shots
- Burn/blackening/singed hair in contact/near-contact wounds
2. Exit Wound
- Usually larger, irregular, stellate or cruciate, with everted (outturned) edges
- No abrasion collar
- More tissue destruction
- Note: Exit wound may be absent if bullet is retained (low-velocity, dissipated energy)
3. Graze/Tangential Wound
- Bullet skims across surface without full penetration
- Elongated, boat-shaped trough
- Beveled edges
B. By Range of Fire
| Range | Features |
|---|---|
| Contact | Muzzle placed against skin; star-shaped laceration; blackening, burning, carbon tattooing inside wound |
| Close range (<60 cm) | Gunpowder tattooing/stippling on skin; singeing |
| Intermediate (60 cm - 1 m) | Some tattooing but no burning |
| Distant (>1 m) | Neat entry wound, abrasion collar only; no tattooing |
C. By Ballistic Type (Weapon/Bullet Velocity)
1. Low-velocity wounds (<600 m/s - handguns, shotguns at distance)
- Bullet causes damage primarily by laceration and crushing along its path
- Relatively limited tissue destruction
- Wound track = caliber of bullet
2. High-velocity wounds (>600 m/s - military rifles, assault weapons)
- Significant cavitation effect: temporary cavity much larger than bullet (up to 30x diameter)
- Massive tissue destruction beyond the wound track
- Yaw and tumbling: bullet becomes unstable inside tissue - greatly increases tissue damage
- Fragmentation possible
- Entry wound often deceptively small compared to internal damage
3. Shotgun wounds
- Contact/close range: devastating single large wound, wad/pellets + powder inside wound
- Intermediate: pellets begin to scatter, multiple puncture wounds
- Distant: diffuse pellet pattern, each wound individually minor
D. By Depth of Penetration
- Perforating - bullet enters AND exits (both entry + exit wound present)
- Penetrating - bullet enters and is retained within body (entry wound only)
- Avulsive/Tangential - bullet grazes surface without full penetration
II. Injuries Caused by Gunshot to the Front of the Chest
The anterior chest is bordered by the sternum, ribs, and chest wall musculature. The key structures at risk include:
| Zone | Structures at Risk |
|---|---|
| Cardiac box (sternal notch to xiphoid, nipple-to-nipple) | Heart, great vessels, trachea, esophagus |
| Right hemithorax | Right lung, right hilum, liver (low), IVC |
| Left hemithorax | Left lung, left hilum, heart, aorta |
| Upper chest | Trachea, subclavian vessels, brachial plexus |
| Thoracoabdominal (below 4th ICS anteriorly) | Diaphragm, liver, spleen, stomach |
Important: The diaphragm may rise as high as the 4th intercostal space anteriorly during expiration - so wounds at or below the nipple line may involve abdominal organs. Coincident thoracic penetration occurs in up to 46% of patients with abdominal injuries.
III. Specific Injury Patterns and Management
1. Simple/Tension Pneumothorax
Pathophysiology: Air enters pleural space from lung or chest wall defect, collapses ipsilateral lung. Tension pneumothorax develops when a one-way valve mechanism traps air - pressure builds, collapses lung, shifts mediastinum, compresses vena cava - causing obstructive shock.
Clinical features (Tension PTX):
- Respiratory distress, hypoxia, tachypnea
- Absent unilateral breath sounds + hyperresonance
- Tracheal deviation away from affected side
- Distended neck veins, hypotension, tachycardia
- Differentiate from tamponade: tamponade has muffled heart sounds, NO tracheal deviation
Management:
- Tension PTX = clinical emergency, do NOT wait for CXR
- Immediate needle decompression: 2nd intercostal space, midclavicular line (or 5th ICS, anterior axillary line in obese)
- Followed by chest tube (intercostal drain) in the 4th-5th ICS, anterior axillary line ("safe triangle")
- Simple PTX: chest tube only; occult PTX (CT only, no CXR finding) may be observed if patient is stable and not on positive pressure ventilation
2. Open Pneumothorax (Sucking Chest Wound)
Occurs when the chest wall defect exceeds the laryngeal cross-sectional area (typically large-caliber gunshot wounds). Air rushes in from outside with each breath - lung collapses, mediastinal shift, decreased venous return.
Signs: Visible wound with sucking/bubbling sound on respiration, hypoxia, respiratory failure.
Management (Current Surgical Therapy, 14e):
- Apply three-sided occlusive dressing (allows air egress but prevents inflow) - Asherman chest seal or petroleum gauze
- Insert a chest tube remote from the wound - BEFORE closing the defect (to prevent converting to tension PTX)
- Wound debridement and formal surgical closure once the patient is stable
3. Hemothorax
Definition: Blood in the pleural space. Most common injury after both penetrating and blunt thoracic trauma.
Classification by volume:
- Small: <300 mL
- Moderate: 300-1500 mL
- Massive: >1500 mL (immediately life-threatening)
Management:
- >85% of cases can be definitively managed with chest tube alone (28-32 Fr intercostal drain, 4th-5th ICS, anterior axillary line) - Schwartz's Principles of Surgery, 11e
- Emergency Department Thoracotomy / Surgical indications:
- Initial chest tube output >1500 mL (20% estimated blood volume in children)
- Ongoing output >150-200 mL/hr for 4 hours (or 2-3 mL/kg/hr in children)
- Hemodynamic instability not responding to resuscitation
- Patient physiology should guide surgical decision over absolute blood volumes
- Retained hemothorax: Video-assisted thoracoscopic surgery (VATS) preferred in stable patients
4. Cardiac Tamponade
Caused by penetrating injury to the heart (especially wounds in the "cardiac box"). As little as 50 mL of blood in the non-distensible pericardial sac compresses the heart and obstructs venous return.
Classic Beck's Triad:
- Elevated CVP / distended neck veins
- Hypotension + tachycardia
- Muffled heart sounds
Note: Neck veins may be flat if concurrent major blood loss has occurred.
Diagnosis: eFAST (most expeditious and reliable - fluid in pericardial sac)
Management (Bailey & Love, 28e):
- Pericardiocentesis has NO role in penetrating cardiac tamponade (clot prevents aspiration)
- Correct treatment is operative:
- Subxiphoid pericardial window (if patient is relatively stable)
- OR left anterolateral thoracotomy / sternotomy for direct cardiac repair
- If in ED with witnessed cardiac arrest from penetrating chest injury: Emergency Department Resuscitative Thoracotomy (EDRT)
5. Emergency Department Resuscitative Thoracotomy (EDRT)
Indicated for patients in extremis from penetrating chest wounds. Decision guided by EAST Practice Management Guidelines:
| Signs of Life in ED | Mechanism | Location | Recommendation |
|---|---|---|---|
| Yes | Penetrating | Thoracic | Strongly yes |
| Yes | Penetrating | Non-thoracic | Yes |
| No (witnessed arrest) | Penetrating | Thoracic | Yes |
| No (unwitnessed) | Blunt | Any | Not recommended |
Best survival (~35%): Single penetrating stab wound to cardiac box + tamponade on FAST + witnessed arrest in ED. Gunshot wounds have lower survival than stab wounds in EDRT. Blunt arrest has near-zero survival.
Technique: Left anterolateral thoracotomy - pericardium opened, clot evacuated, cardiac laceration repaired (digital pressure, Satinsky clamp for atrial wounds; skin staples or Foley catheter balloon for temporary ventricular occlusion; definitive repair with pledgeted non-absorbable sutures).
6. Pulmonary Parenchymal Injury
- Most are managed with tube thoracostomy alone
- Persistent air leak: bronchoscopy-directed fibrin glue or VATS
- Central injuries during thoracotomy: pulmonary tractotomy (GIA stapler inserted into injury track, filleted open, individual vessels and bronchi ligated) - avoids formal lobectomy
- Peripheral lacerations: stapled wedge resection
- Formal lobectomy only for proximal vascular/bronchial injury found on tractotomy
- Pneumonectomy is almost always fatal due to right heart decompensation
7. Tracheobronchial Injury
Signs: air escaping from neck wound, massive air leak post-chest tube, hemoptysis, stridor, subcutaneous emphysema.
Management:
- Pass ETT beyond the injury or into contralateral mainstem bronchus for ventilation
- Primary end-to-end repair (3-0 PDS, single layer interrupted)
- Suture line buttressed with vascularized tissue (pericardium, intercostal muscle, pleura)
- Bronchial injuries <1/3 circumference with no major air leak: expectant management
8. Thoracoabdominal Wounds (Below 4th ICS Anteriorly)
- Must exclude diaphragmatic injury (diaphragm rises to 4th ICS anteriorly in expiration)
- Diaphragmatic wounds may not be apparent initially - diagnose by laparoscopy
- All injuries to the diaphragm require repair (staple/suture)
- Must also assess for injury to liver, spleen, stomach
IV. ATLS Primary Survey Framework for Penetrating Chest GSW
"MARCH" / "ABCDE" priorities:
- A - Airway: Secure; cricothyroidotomy if cannot intubate
- B - Breathing: Identify/treat tension PTX, open PTX, hemothorax, flail chest
- C - Circulation: FAST for tamponade; control hemorrhage; IV access; permissive hypotension (target SBP 80-90 mmHg in penetrating torso trauma) until surgical hemorrhage control - AVOID fluid overload
- D - Disability: GCS, pupils
- E - Exposure: Full exposure, look for exit wound, thoracoabdominal involvement
Key principle in penetrating chest GSW: Avoid extensive pre-hospital interventions - rapid transport to trauma centre takes priority. Hypotensive resuscitation (limited resuscitation before operative hemorrhage control) is now the military-derived standard for civilian penetrating torso trauma.
Sources: Current Surgical Therapy 14e; Bailey & Love's Short Practice of Surgery 28e; Schwartz's Principles of Surgery 11e; Mulholland and Greenfield's Surgery 7e
Classification of firearm wounds management of gun shot injury from front of chest
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I now have all the content and images needed for a comprehensive, well-illustrated answer. Let me compile the full response.
Classification of Firearm Wounds and Management of Gunshot Injury to the Front of the Chest
PART 1: CLASSIFICATION OF FIREARM WOUNDS
A. Classification by Wound Morphology
1. Entry Wound
- Typically smaller, round or oval with inverted (indrawn) edges
- Has an abrasion collar (graze contusion ring) - caused by bullet spin and friction against skin
- Central defect = approximately bullet caliber
- Surrounding skin intact / relatively clean edges
- At contact range: star-shaped laceration from gas blast, blackening, burning, carbon tattooing inside the wound canal
- At close range (<60 cm): gunpowder stippling/tattooing on skin, possible singeing
2. Exit Wound
- Usually larger, irregular, stellate or cruciate shape
- Edges are everted (outturned)
- No abrasion collar
- Greater tissue destruction
- May be absent if bullet is retained (low-velocity, energy dissipated, or bullet fragmented)
3. Tangential / Graze Wound
- Bullet skims the surface without full penetration
- Elongated, boat-shaped trough with beveled edges
- Both ends have features of entry (abrasion collar at entry end)
B. Classification by Range of Fire
| Range | Wound Features |
|---|---|
| Contact (muzzle touches skin) | Star-shaped laceration; burning, blackening, carbon tattooing inside wound; muzzle imprint on skin |
| Close range (<60 cm) | Gunpowder stippling/tattooing on surrounding skin; singeing of hair |
| Intermediate (60 cm - 1 m) | Faint tattooing present; no burning |
| Distant (>1 m) | Clean entry wound with abrasion collar only; no tattooing |
C. Classification by Ballistic Type (Velocity)
1. Low-Velocity Wounds (<600 m/s - handguns, pistols)
- Damage by laceration and crushing along bullet track
- Wound track = approximately bullet caliber
- Relatively limited tissue destruction beyond direct path
- Bullet often retained (penetrating, no exit wound)
2. High-Velocity Wounds (>600 m/s - military rifles, assault weapons)
- Cavitation effect: temporary cavity forms that is up to 30x the bullet diameter - massive tissue destruction well beyond the bullet track
- Yaw and tumbling: bullet becomes unstable inside tissue, dramatically increasing damage
- Entry wound is deceptively small compared to internal destruction
- Fragmentation possible - multiple secondary missiles
- Exit wound is large and irregular
3. Shotgun Wounds
| Distance | Pattern |
|---|---|
| Contact/Close | Single devastating wound; wad + pellets + powder may be inside |
| Intermediate | Pellets scatter - multiple puncture wounds |
| Distant | Diffuse pellet pattern; individual wounds minor; pattern useful for range estimation |
D. Classification by Depth of Penetration
- Perforating wound - bullet enters AND exits (entry + exit wound present)
- Penetrating wound - bullet enters and is retained (entry wound only)
- Avulsive/Tangential wound - bullet grazes the surface without full penetration
PART 2: INJURIES FROM GUNSHOT TO THE FRONT OF THE CHEST
Anatomical Zones at Risk - Anterior Chest
| Zone | Structures at Risk |
|---|---|
| Cardiac box (sternal notch to xiphoid, nipple-to-nipple) | Heart, great vessels, trachea, esophagus, thoracic duct |
| Right hemithorax | Right lung/hilum, liver (if low), IVC |
| Left hemithorax | Left lung/hilum, heart, descending aorta |
| Upper anterior chest | Trachea, subclavian vessels, brachial plexus |
| Thoracoabdominal (below 4th ICS anteriorly) | Diaphragm, liver, spleen, stomach |
Critical point: The diaphragm rises to the 4th intercostal space anteriorly during expiration. Wounds at or below the nipple line may injure abdominal viscera. Coincident thoracic penetration occurs in up to 46% of patients with abdominal injuries.
PART 3: MANAGEMENT OF SPECIFIC INJURY PATTERNS
1. Simple Pneumothorax
Mechanism: Air enters pleural space from lung laceration - lung collapses ipsilaterally.
Features: Decreased breath sounds, hyperresonance, reduced chest expansion on affected side.
Classification by volume:
- Small: <1/3 lung collapse on CXR
- Large: complete lung collapse, no mediastinal shift, no hypotension
Management:
- Intercostal drain (chest tube) in 4th-5th ICS, anterior axillary line
- Occult PTX (CT-only finding, not on CXR): may be observed carefully if hemodynamically stable and not on positive-pressure ventilation. Failure of observation rate = 6% overall (14% if on PPV). Factors predicting failure: PTX >7 mm, PPV, respiratory distress, hemothorax, progression on serial CXR
2. Tension Pneumothorax
Mechanism: One-way valve effect - air continuously enters pleural space and cannot escape. Collapses ipsilateral lung, shifts mediastinum, compresses SVC/IVC - obstructive shock.
Clinical features (Current Surgical Therapy, 14e):
- Air hunger, hypoxia, tachypnea
- Hyperresonance + absent breath sounds - ipsilateral
- Tracheal deviation away from affected side
- Distended neck veins + hypotension + tachycardia
- Note: Tracheal deviation may be absent if patient is intubated. Neck veins may be flat with concurrent hypovolaemia
Differentiating from Cardiac Tamponade (both cause JVD + hypotension):
- Tamponade: muffled heart sounds, NO tracheal deviation, NO asymmetric breath sounds
- Tension PTX: tracheal deviation, hyperresonance, absent breath sounds
Management - clinical emergency, do NOT wait for CXR:
- Immediate needle decompression - 14-16G angiocatheter, 2nd ICS midclavicular line (or 5th ICS anterior axillary line in obese patients). Rush of air = confirms diagnosis, converts to simple PTX
- Followed immediately by chest tube (intercostal drain) in the "safe triangle" (bounded by: lateral border of pectoralis major anteriorly, latissimus dorsi posteriorly, line perpendicular to nipple inferiorly) - Bailey & Love, 28e

Needle decompression technique for tension pneumothorax - Current Surgical Therapy 14e
3. Open Pneumothorax ("Sucking Chest Wound")
Occurs when a large-caliber gunshot creates a chest wall defect exceeding the laryngeal cross-sectional area, allowing atmospheric air to rush in with each respiratory cycle. Lung collapses rapidly; mediastinal shift and decreased venous return follow. (Current Surgical Therapy, 14e)
Signs: Audible sucking/bubbling at wound site, hypoxia, respiratory failure, hypotension.
Management - sequential steps:
- Apply three-sided occlusive dressing (petroleum gauze / Asherman chest seal) - allows air to exit on expiration but prevents entry on inspiration
- Place intercostal drain remote from the wound - BEFORE closing the defect, to prevent conversion to tension PTX
- Once patient is stable: wound debridement and formal surgical closure in the operating theatre
4. Hemothorax
Blood accumulates in the pleural cavity (capacity up to 3 L). Most common injury from both blunt and penetrating thoracic trauma. The pleural space can act as a significant reservoir - supine CXR may miss accumulations <200 mL (shows only diffuse haziness).
Classification by volume:
- Small: <300 mL
- Moderate: 300-1500 mL
- Massive: >1500 mL - may present with tension physiology
Management (Schwartz's Principles of Surgery, 11e):
- >85% of all hemothoraces are definitively managed with chest tube alone (reexpansion of the lung seals the low-pressure pulmonary laceration)
- One caveat: even if initial output is 1.5 L, if bleeding stops and lung is re-expanded in a hemodynamically stable patient, non-operative management may still be pursued
Indications for thoracotomy (Schwartz's, Table 7-10):
| Indication | Threshold |
|---|---|
| Initial chest tube output - penetrating | >1000 mL |
| Initial chest tube output - blunt | >1500 mL |
| Ongoing chest tube output | >200 mL/hr for 3 consecutive hours (non-coagulopathic) |
| Caked/retained hemothorax | Despite 2 chest tubes |
| Great vessel injury | Any |
| Pericardial tamponade | Any |
| Oesophageal perforation | Any |
| Air embolism | Any |
- Retained hemothorax: Video-assisted thoracoscopic surgery (VATS) is the preferred approach in stable patients; reduces empyema risk
5. Cardiac Tamponade
Mechanism: Penetrating injury to the heart - as little as 50 mL of blood in the non-distensible pericardial sac compresses the heart and obstructs venous return. All patients with penetrating injury to the cardiac box plus shock = cardiac injury until proven otherwise.
Classic Beck's Triad:
- Elevated CVP / distended neck veins
- Hypotension + tachycardia
- Muffled heart sounds
Note: Neck veins may be flat if concurrent haemorrhage elsewhere has lowered CVP.
Diagnosis: eFAST is the most expeditious and reliable tool - shows fluid in pericardial sac. Chest X-ray may show enlarged cardiac shadow.
Management (Bailey & Love, 28e):
- Pericardiocentesis has NO role in penetrating cardiac tamponade - clot inside pericardium prevents effective aspiration
- Correct treatment is operative:
- Subxiphoid pericardial window - for relatively stable patients (allows drainage and diagnosis)
- Left anterolateral thoracotomy or median sternotomy - for definitive cardiac repair
- Emergency Department Thoracotomy - if patient arrests in the ED
Cardiac wound repair (Schwartz's, 11e):
- Atrial injuries: Satinsky vascular clamp for hemorrhage control
- Ventricular injuries: digital pressure initially; skin staples for temporary control of LV lacerations; Foley catheter balloon for large stellate lesions (use cautiously - traction enlarges wound)
- Definitive repair: running 3-0 polypropylene or interrupted pledgeted 2-0 polypropylene sutures; pledgets especially important for thin-walled right ventricle
- Injuries adjacent to coronary arteries: horizontal mattress sutures (running sutures would occlude the coronary artery)
- Stellate/friable GSW wounds: surgical adhesive (BioGlue) may be used if edges cannot be fully approximated
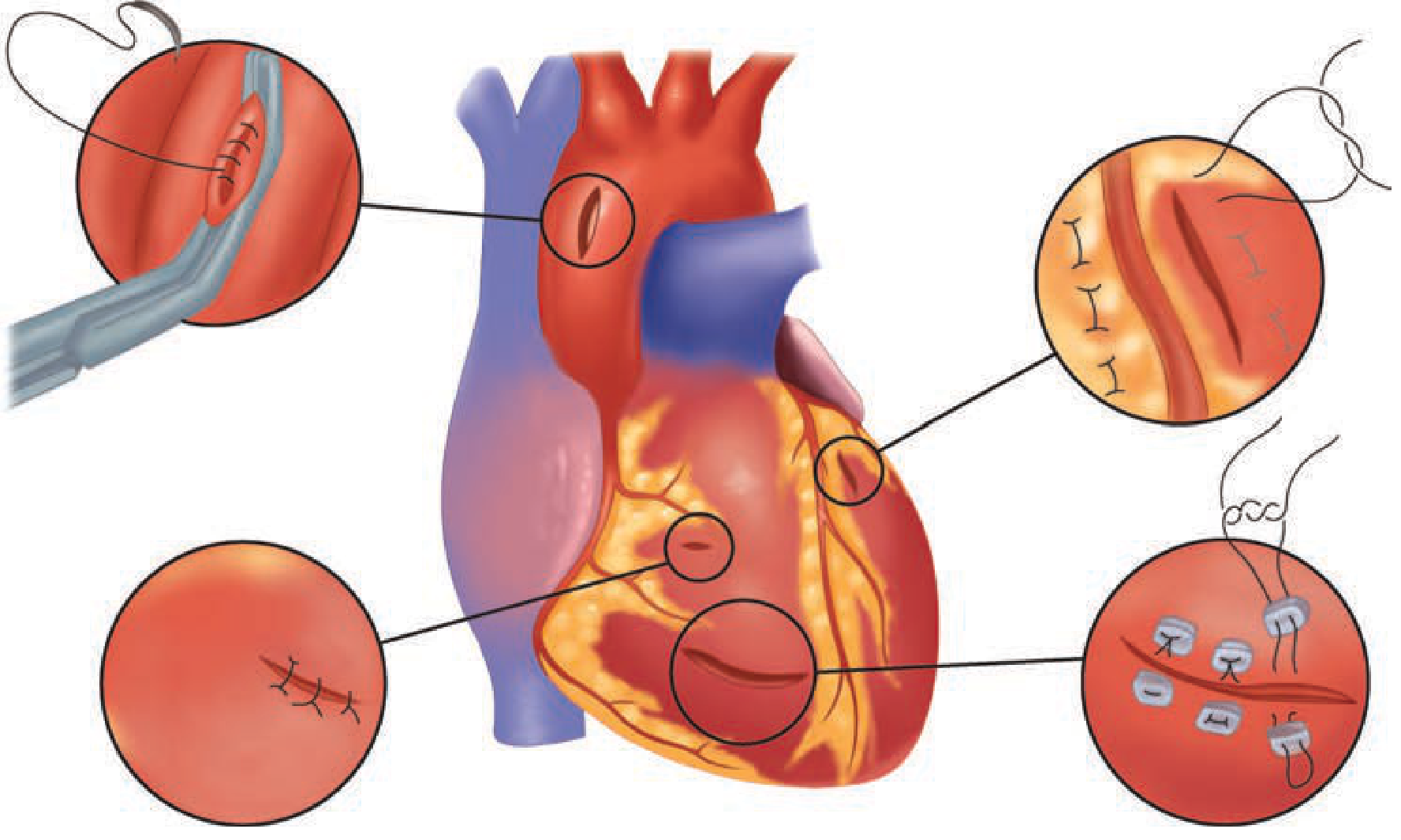
Cardiac wound repair techniques - Schwartz's Principles of Surgery 11e
6. Emergency Department Resuscitative Thoracotomy (EDRT)
Indicated for patients who arrive in extremis or arrest from penetrating thoracic injury. Non-compressible thoracic hemorrhage is the number one cause of death in organized trauma centres. (Current Surgical Therapy, 14e)
Goals of EDRT:
- Release pericardial tamponade
- Direct hemorrhage control
- Open cardiac massage
- Descending aortic cross-clamping (prioritizes cerebral + coronary perfusion; controls sub-diaphragmatic hemorrhage)
- Internal defibrillation
EAST Practice Management Guidelines for EDRT:
| Signs of Life in ED | Mechanism | Location | Recommendation |
|---|---|---|---|
| Yes | Penetrating | Thoracic | Strongly YES |
| No | Penetrating | Thoracic | Conditional yes |
| Yes | Penetrating | Extrathoracic | Conditional yes |
| No | Penetrating | Extrathoracic | Conditional yes |
| Yes | Blunt | Any | Conditional yes |
| No | Blunt | Any | Conditional NO |
Western Trauma Association CPR time limits for EDRT:
- Penetrating torso: <15 min prehospital CPR
- Penetrating neck: <5 min prehospital CPR
- Blunt: <10 min prehospital CPR
Survival rates:
- Best outcome (~35%): Single penetrating stab wound to cardiac box + tamponade on FAST + witnessed arrest in ED
- GSW to chest: lower survival than stab wounds
- Blunt cardiac arrest: near-zero survival if unwitnessed
Technique - Left Anterolateral Thoracotomy:
- Patient supine, left arm raised
- Incision along 4th-5th ICS (males: along nipple line; females: along inframammary fold)
- Enter just above the superior border of the rib (avoids intercostal neurovascular bundle)
- Open pericardium longitudinally, anterior to phrenic nerve, evacuate clot
- Repair cardiac wound, cross-clamp descending aorta if needed
- Extend to "clamshell" (bilateral) if right-sided injury suspected
7. Tracheobronchial Injury
Signs: Air escaping from neck wound, massive air leak after tube thoracostomy, hemoptysis, stridor, subcutaneous emphysema, dysphagia. CXR + chest CT are first-line imaging. (Sabiston, current ed.)
Management:
- Pass ETT beyond the injury or into the contralateral mainstem bronchus to maintain ventilation
- Primary end-to-end repair with 3-0 PDS, single-layer interrupted sutures; buttress suture line with vascularized tissue (pericardium, intercostal muscle, pleura)
- Injuries <1/3 circumference with no major air leak: expectant management
- Peripheral bronchial injuries with persistent leak: bronchoscopically directed fibrin glue
8. Pulmonary Parenchymal Injury
- Majority managed with tube thoracostomy alone
- Pulmonary tractotomy: for central injuries encountered during thoracotomy - GIA-100 stapler inserted into wound track, filleted open, individual vessels and bronchi ligated selectively; avoids formal lobectomy
- Peripheral lacerations: stapled wedge resection
- Formal lobectomy: only when tractotomy reveals proximal injury
- Pneumonectomy: usually fatal (right heart decompensation from acute increase in afterload)
- Bronchovenous fistula (air embolism risk): minimized by prompt control of major air leaks
9. Thoracoabdominal Wounds (Below Nipple Line)
- Must always exclude diaphragmatic injury in anterior wounds below the 4th ICS
- Initial wound may appear thoracic but violate the peritoneum
- Diagnosis: laparoscopy (most sensitive for diaphragmatic lacerations, which can be very small)
- All diaphragmatic injuries require repair
- Must assess for concomitant injury to liver, spleen, stomach
PART 4: ATLS APPROACH - INITIAL RESUSCITATION FRAMEWORK
Primary Survey Priorities (ABCDE)
| Priority | Action |
|---|---|
| A - Airway | Secure airway early; RSI; if cannot intubate - surgical cricothyroidotomy |
| B - Breathing | Identify and treat: tension PTX, open PTX, massive hemothorax, flail chest |
| C - Circulation | eFAST for tamponade; 2x large-bore IV; permissive hypotension (target SBP 80-90 mmHg) until surgical hemorrhage control; massive transfusion protocol if needed (1:1:1 pRBC:FFP:platelets) |
| D - Disability | GCS, pupils |
| E - Exposure | Full undress; find ALL wounds including exit wounds and thoracoabdominal extension |
Key transport principle: In urban settings (trauma centre within 15-25 min), rapid transport takes precedence over extensive field interventions. Hypotensive resuscitation (limited or no resuscitation before operative hemorrhage control) is the current military-derived civilian standard for penetrating torso trauma. Cervical collar and spinal immobilization are unnecessary unless the patient has specific cervical complaints. (Roberts & Hedges; Current Surgical Therapy, 14e)
Sources: Current Surgical Therapy 14e | Schwartz's Principles of Surgery 11e | Bailey and Love's Short Practice of Surgery 28e | Mulholland and Greenfield's Surgery 7e | Sabiston Textbook of Surgery (current ed.)
This is a shared conversation. Sign in to Orris to start your own chat.