Demonstrate the procedure of the Polysomnography and interpret the result . For long answer in exam
Reading File
Finding Sources
Finding Sources
Searching the Web
polysomnography procedure interpretation sleep study PSG stages
Reading File
Reading File
Reading File
Reading File
Searching Images
polysomnography PSG sleep study recording EEG EOG EMG channels
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Reading File
Searching Images
sleep hypnogram architecture NREM REM cycles stages diagram
Loading Image
Loading Image
I now have all the material needed to write a comprehensive, exam-quality answer. Here it is:
Polysomnography (PSG): Procedure and Interpretation
Definition
Polysomnography is the continuous, attended, comprehensive recording of multiple biophysiological signals during sleep. It is the gold standard (Level 1) diagnostic test for sleep disorders. A standard overnight PSG is 6–8 hours in duration and is conducted in a sleep laboratory by a trained technologist.
I. INDICATIONS
- Diagnosis of sleep-related breathing disorders (OSA, central sleep apnea, hypoventilation syndromes)
- CPAP/BiPAP titration and treatment efficacy assessment
- Evaluation of violent or potentially injurious sleep behaviors (parasomnias)
- Differentiating narcolepsy from other hypersomnolence disorders
- Differentiating parasomnias from nocturnal seizures
- Assessment of periodic limb movement disorder (PLMD)
- Required the night before a Multiple Sleep Latency Test (MSLT) for narcolepsy workup
- Neuromuscular disorders causing sleep-related hypoventilation
II. PARAMETERS MONITORED (Channels Recorded)
BOX: PSG Monitors (AASM Standard)
| Parameter | Channel | Purpose |
|---|---|---|
| EEG | C3/C4, O1/O2, F3/F4 (10–20 system) | Sleep staging; detect seizures |
| Electrooculogram (EOG) | Left + Right outer canthus | Sleep staging; detect REM |
| Submental EMG | Chin (mentalis) | Sleep staging; detect REM atonia |
| Anterior tibial EMG | Bilateral leg | Periodic limb movements |
| Nasal/oral airflow | Thermistor + nasal pressure transducer | Detect apneas/hypopneas |
| Respiratory effort | Chest + abdominal RIP belts | Distinguish obstructive vs. central |
| ECG | Single-lead | Cardiac arrhythmias |
| Pulse oximetry (SpO₂) | Finger probe | Oxygen desaturation |
| Body position | Sensor | Position-dependent OSA |
| Snoring/tracheal microphone | Neck | Document snoring |
| Optional: End-tidal CO₂ | Transcutaneous/capnography | Hypoventilation |
| Optional: Esophageal pressure (Pes) | Manometer | Upper airway resistance syndrome (UARS) |
(Source: Cummings Otolaryngology, Box 15.5; Murray & Nadel's Respiratory Medicine)
III. PROCEDURE — STEP BY STEP
A. Pre-Study Preparation
- Patient instructions: Avoid caffeine, alcohol, sedatives, and naps on the day of the study. Patients should maintain normal sleep schedule.
- History and questionnaire: Epworth Sleepiness Scale, STOP-BANG questionnaire, Berlin Sleep Questionnaire completed before arrival.
- Arrival: Patient arrives 1–2 hours before habitual bedtime.
B. Electrode and Sensor Application

Patient undergoing PSG setup: Scalp electrodes for EEG are affixed using conductive paste; facial electrodes for EOG; chin and leg EMG electrodes; chest/abdominal belts; pulse oximeter; ECG leads; nasal cannula and/or thermistor.
EEG placement follows the International 10-20 system:
- Central leads (C3, C4) — primary for sleep staging
- Occipital leads (O1, O2) — detect alpha rhythm (wakefulness)
- Frontal leads (F3, F4) — K-complexes and slow waves
EOG electrodes: Placed at outer canthi, 1 cm above right eye and 1 cm below left eye (E1-M2, E2-M2 derivations).
EMG electrodes: Submental (chin) — 2 cm above and 2 cm below chin; bilateral anterior tibialis muscles.
Respiratory sensors: Nasal pressure transducer + oronasal thermistor; chest + abdominal RIP belts.
Impedances: All electrode impedances should be <5 kΩ before recording begins.
C. Recording
- Patient sleeps in a private room while a technologist monitors in an adjacent room via infrared video + audio recording.
- Digital PSG records all channels simultaneously.
- Recording speed: 10 mm/sec (standard for sleep staging).
- Epoch: Each 30-second segment of recording is called an epoch; this is the basic unit of sleep staging.
- If a technical problem (lead fall-off, artifact) occurs, the technologist re-applies the sensor without waking the patient.
D. Post-Recording
- Data is downloaded and either auto-scored or manually scored by a certified PSG technologist.
- Final interpretation is provided by a board-certified sleep medicine physician.
- A summary report includes: total sleep time (TST), sleep latency, REM latency, sleep efficiency, stage distribution, AHI, arousal index, O₂ nadir, and SpO₂ < 90% time.
IV. SLEEP STAGING — THE BASIS OF INTERPRETATION
Sleep is scored in 30-second epochs. The AASM (2007) scoring manual classifies sleep into:
Stage W → N1 → N2 → N3 → R (REM)
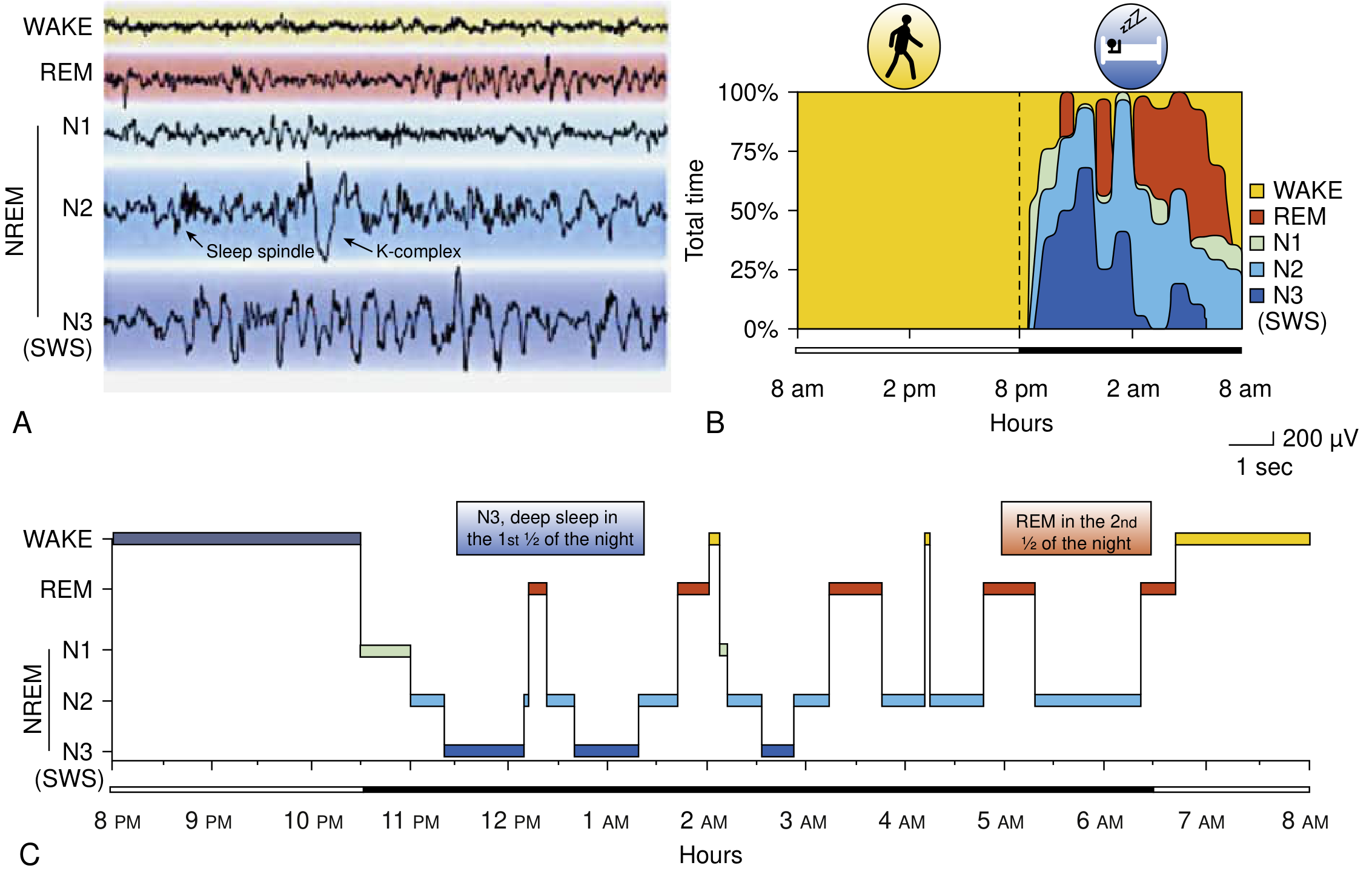
Fig: (A) EEG waveforms for each sleep stage. Note sleep spindles and K-complexes in N2; high-amplitude slow waves in N3 (SWS). (B) Proportion of sleep stages over 24 hours. (C) Sleep hypnogram showing N3-dominant first half of the night and REM-dominant second half. — Bradley and Daroff's Neurology, Fig. 101.1
Stage W (Wakefulness)
- EEG: Alpha rhythm (8–13 Hz) with eyes closed; low amplitude mixed-frequency with eyes open
- EOG: Voluntary/blinking eye movements
- EMG: High chin tone
- Scored when >50% of epoch contains alpha frequency
Stage N1 (Light Sleep) — 3–8% of TST
- EEG: Alpha rhythm drops to <50% of epoch; theta waves (4–7 Hz) predominate; vertex sharp waves appear
- EOG: Slow rolling eye movements
- EMG: Slightly decreased muscle tone
- Transitional stage; patient may not be aware they have fallen asleep
Stage N2 (Light Sleep) — 45–55% of TST
- EEG: Sleep spindles (12–18 Hz bursts, 0.5–2 sec duration) + K-complexes (biphasic sharp wave, ≥0.5 sec); theta activity; slow waves <20%
- EOG: Minimal or no eye movements
- EMG: Further reduced tone
- K-complex = hallmark of N2; thought to suppress arousal and consolidate memory
Stage N3 (Slow-Wave/Deep Sleep) — 15–25% of TST
- EEG: ≥20% of epoch comprised of delta waves (0.5–2 Hz, amplitude >75 μV)
- EOG: No eye movements
- EMG: Variable, often lowest tone
- Most restorative stage; growth hormone secretion; parasomnias (sleepwalking, sleep terrors) arise here
- Predominates in the first third of the night
Stage R (REM Sleep) — 20–25% of TST
- EEG: Low-amplitude, mixed-frequency activity; sawtooth waves (2–6 Hz, notched appearance)
- EOG: Rapid conjugate eye movements in all directions (phasic)
- EMG: Muscle atonia (chin EMG at lowest level — key feature)
- REM latency: normally 60–90 minutes after sleep onset
- Dreaming predominantly occurs here
- REM episodes lengthen across the night; longest REM in last third of night
- Absence of atonia = REM Sleep Behavior Disorder (RBD)
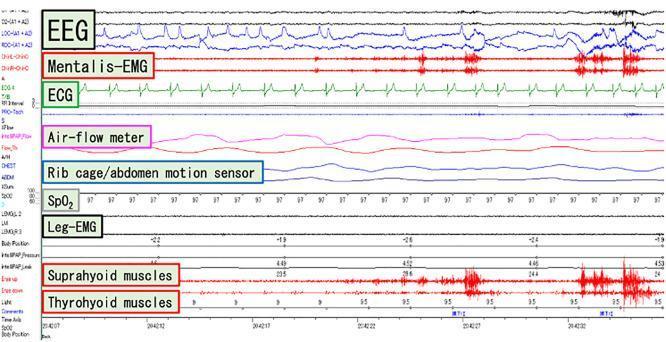
Fig: Multi-channel PSG tracing showing concurrent EEG, Mentalis-EMG (chin), ECG, airflow meter, rib cage/abdomen effort sensors, SpO₂ tracking, and leg-EMG.
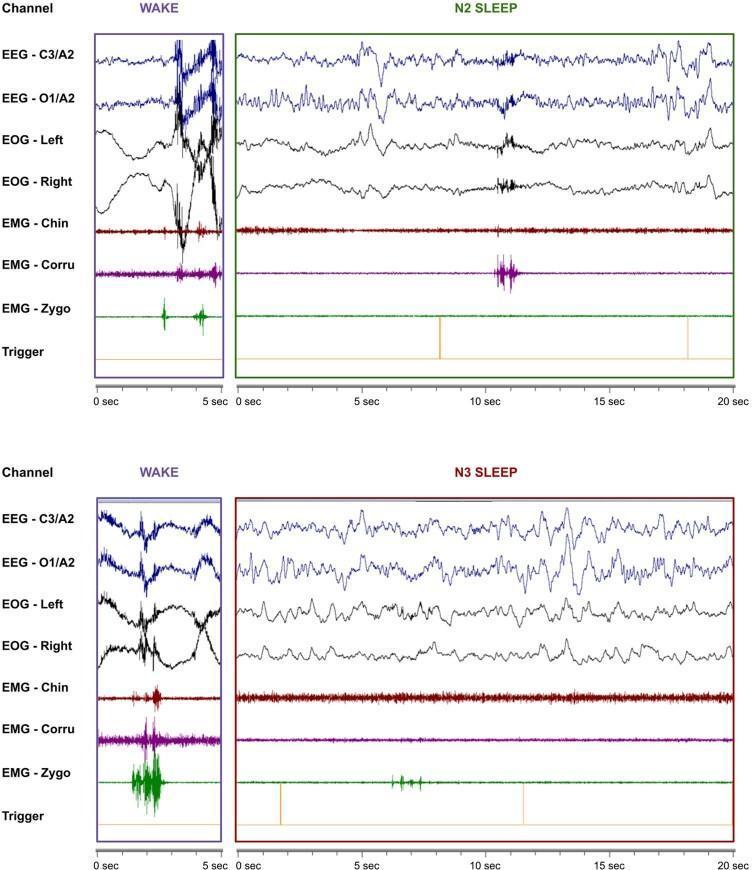
Fig: Comparison PSG tracings across vigilance states — Wakefulness shows high-amplitude EEG; N2 shows sleep spindles and K-complexes; N3 (slow-wave sleep) shows high-amplitude, low-frequency delta waves with reduced chin EMG tone.
V. RESPIRATORY EVENT DEFINITIONS
| Event | Definition |
|---|---|
| Obstructive apnea | Cessation of airflow (≥90% drop) for ≥10 sec with continued respiratory effort |
| Central apnea | Cessation of airflow for ≥10 sec with absent respiratory effort |
| Mixed apnea | Begins as central (no effort), then obstructive effort resumes before airflow returns |
| Hypopnea | ≥30% reduction in airflow for ≥10 sec + ≥3–4% SpO₂ desaturation and/or cortical arousal |
| RERA | Respiratory effort–related arousal: flow limitation causing arousal without meeting apnea/hypopnea criteria |
(Source: Cummings Otolaryngology, Fig. 186.4; Murray & Nadel's, Table 120.1; Miller's Anesthesia)
VI. KEY CALCULATED INDICES
| Index | Formula | Normal |
|---|---|---|
| AHI (Apnea-Hypopnea Index) | (Total apneas + hypopneas) / TST (hr) | <5/hr |
| RDI (Respiratory Disturbance Index) | (Apneas + hypopneas + RERAs) / TST (hr) | <5/hr |
| Arousal Index | Arousals per hour of sleep | <10/hr |
| Sleep Efficiency | (TST / Time in Bed) × 100 | >85% |
| REM Latency | Time from sleep onset to first REM epoch | 60–90 min |
| O₂ Nadir | Lowest SpO₂ recorded | >90% |
VII. INTERPRETATION OF RESULTS
A. Normal PSG
| Parameter | Normal Value |
|---|---|
| Sleep latency | <20 minutes |
| REM latency | 60–90 minutes |
| Sleep efficiency | >85% |
| % N1 | 3–8% |
| % N2 | 45–55% |
| % N3 (SWS) | 15–25% |
| % REM | 20–25% |
| AHI | <5 events/hour |
| O₂ nadir | >90% |
| Arousal index | <10/hr |
Normal sleep cycles last 90–100 minutes; 4–6 cycles occur per night. N3 dominates early, REM dominates late.
B. OSA Severity (AASM/Miller's Anesthesia Classification)
| Severity | AHI |
|---|---|
| Normal | <5/hr |
| Mild OSA | 5–14/hr |
| Moderate OSA | 15–30/hr |
| Severe OSA | >30/hr |
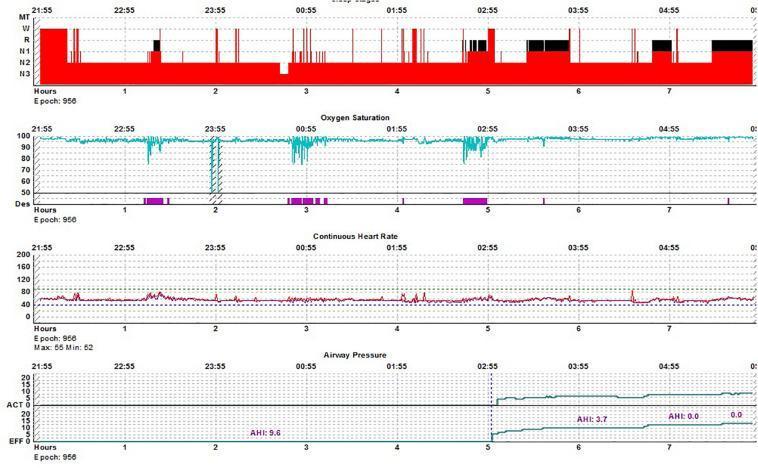
Fig: Split-night PSG. Top panel (hypnogram) shows sleep stage progression. SpO₂ panel shows cyclic desaturations clustering during REM sleep. After CPAP initiation (bottom panel, ~02:55), AHI drops from 9.6 to 0.0 — demonstrating effective treatment.
C. PSG Findings in Specific Disorders
| Disorder | Key PSG Findings |
|---|---|
| Obstructive Sleep Apnea | ↑AHI; obstructive events (effort present); O₂ desaturations; arousals; worse in REM and supine position |
| Central Sleep Apnea | Central apneic events (absent effort and airflow); seen in heart failure, high altitude |
| Narcolepsy | Short REM latency (<20 min); sleep-onset REM periods (SOREMPs) on MSLT; excessive N1 |
| Major Depression | ↓ REM latency; ↑ REM density; ↑ REM% in first half of night; ↓ SWS (N3) |
| PLMD | Periodic limb movements on tibial EMG (≥4 consecutive movements, 0.5–10 sec each, 5–90 sec apart); ≥15 PLMs/hr with arousals |
| REM Sleep Behavior Disorder (RBD) | Loss of REM atonia (REM sleep without atonia — RSWA); tonic/phasic EMG activity during REM |
| Sleepwalking / Night Terrors | Arousals from N3 sleep; abrupt EEG desynchronization during slow-wave sleep |
| Sleep-Related Epilepsy | Paroxysmal EEG discharges, often arising from N1/N2 |
D. Arousal Index Interpretation
- Normal: <10 arousals/hr
- Elevated arousal index without clear respiratory events → suggests UARS (Upper Airway Resistance Syndrome); requires esophageal pressure monitoring for confirmation
- Awake esophageal pressure: normally −10 to −5 cmH₂O
VIII. TYPES OF SLEEP STUDIES
| Level | Type | Channels | Setting |
|---|---|---|---|
| Level 1 | Full attended PSG | ≥7 (EEG, EOG, EMG, ECG, airflow, effort, SpO₂) | In-laboratory |
| Level 2 | Unattended full PSG | ≥7 | Home/unattended |
| Level 3 | Home Sleep Apnea Test (HSAT) | 4–7 (airflow, effort, SpO₂, ± HR) | Home |
| Level 4 | Limited channel | 1–2 (usually SpO₂ ± airflow) | Home |
Important: A negative HSAT (Level 3/4) in a symptomatic patient does not exclude OSA — in-laboratory PSG must be performed due to lower sensitivity of home tests.
IX. LIMITATIONS OF PSG
- First-night effect: Sleep may be disturbed by the unfamiliar environment and electrode placement — sleep efficiency may be artificially reduced
- Expensive and resource-intensive; limited laboratory availability
- Does not replicate the patient's habitual home sleep environment
- Attended in-lab PSG not available in many locations — rationale for home sleep testing
- A single night may not represent every night's sleep pattern
- HSAT (portable monitoring) cannot diagnose the full spectrum of sleep disorders
(Source: Cummings Otolaryngology; Kaplan & Sadock's Comprehensive Textbook of Psychiatry; Murray & Nadel's Respiratory Medicine)
SUMMARY MNEMONIC: "PEAR-RAD"
Parameters: EEG, EOG, EMG, ECG, airflow, effort, SpO₂ Epochs: 30-second segments AHI: Classification (<5 normal; 5–14 mild; 15–30 moderate; >30 severe) REM latency: 60–90 min normally; shortened in narcolepsy and depression Restorative: N3 (slow-wave) sleep most restorative; dominates early night Atonia: REM atonia — loss → RBD Disorders: OSA, narcolepsy, PLMD, parasomnias, seizures
Sources: Bradley and Daroff's Neurology in Clinical Practice; Kaplan & Sadock's Comprehensive Textbook of Psychiatry; Cummings Otolaryngology Head and Neck Surgery; Murray & Nadel's Textbook of Respiratory Medicine; Miller's Anesthesia, 10e; Kaplan and Sadock's Synopsis of Psychiatry
This is a shared conversation. Sign in to Orris to start your own chat.