Tretment of sle pllt admitted in derma ward
Reading File
Finding Sources
Searching PubMed
"systemic lupus erythematosus"[MeSH Terms] AND "therapy"[MeSH Terms]
Finding Sources
Searching PubMed
"systemic lupus erythematosus" AND treatment
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
I have comprehensive data. Let me now compile the full, structured answer for an SLE patient admitted to the dermatology ward.
Treatment of SLE - Patient Admitted to Dermatology Ward
Here is a comprehensive, organ-by-organ treatment guide for SLE based on current textbook guidelines (Harrison's 22E 2025, Washington Manual, Firestein & Kelley's Rheumatology, Fitzpatrick's Dermatology).
Severity-Based Treatment Framework
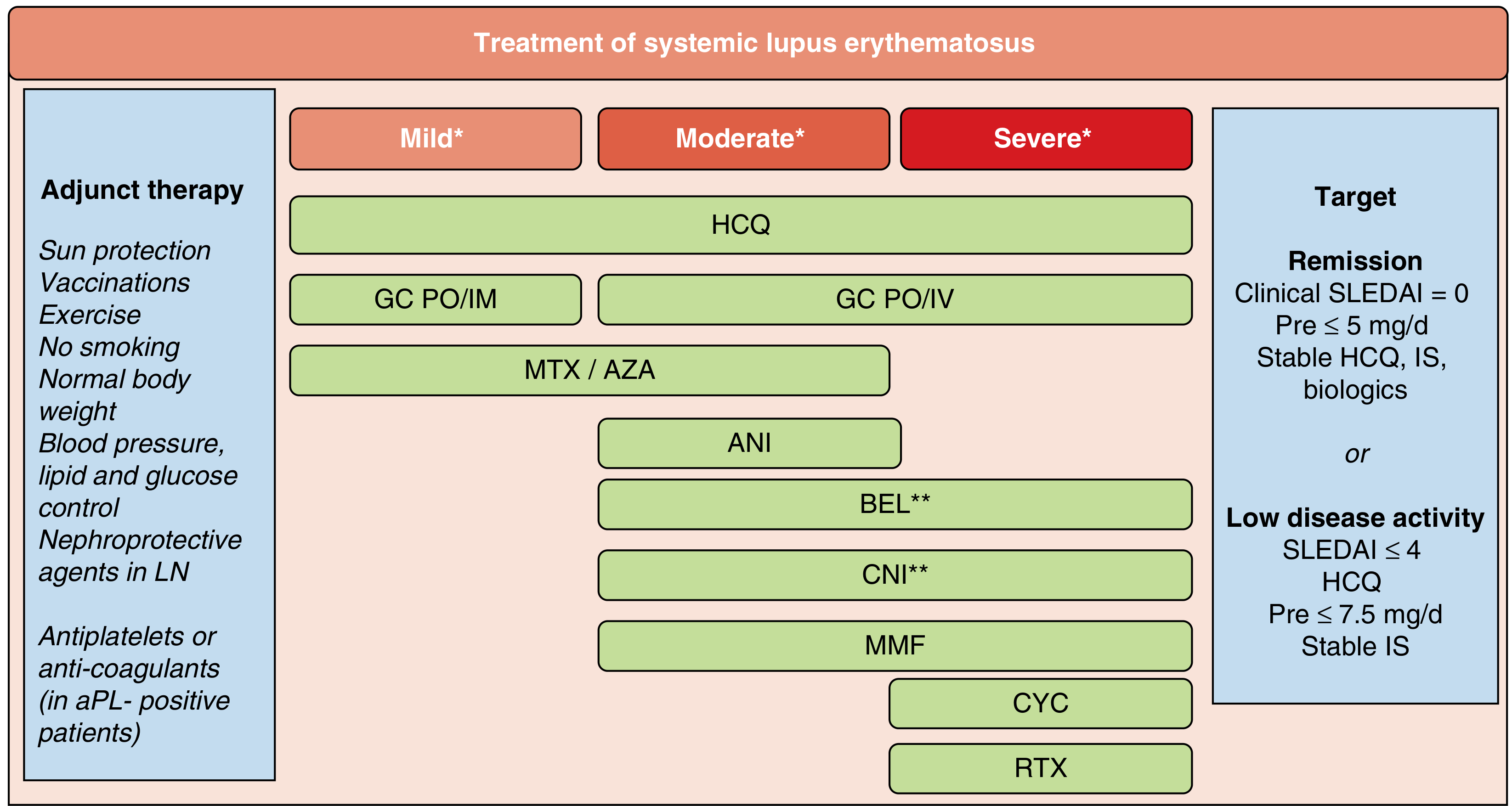
Fig. 82.1 - Firestein & Kelley's Textbook of Rheumatology, 2-Volume Set
Classify Disease Severity First
| Severity | Features |
|---|---|
| Mild | Mucocutaneous disease, arthralgia/arthritis, leukopenia, mild thrombocytopenia, mild serositis |
| Moderate | Unresponsive to standard therapy, low C3/C4 + high anti-dsDNA, significant cutaneous/joint/hematologic disease |
| Severe | Lupus nephritis, CNS involvement, pneumonitis, vasculitis, severe cytopenias, hemolytic anemia |
1. Universal Therapy (ALL Patients, All Severities)
Hydroxychloroquine (HCQ) - BACKBONE OF SLE TREATMENT
-
Dose: 5 mg/kg/day of real body weight PO (max 400 mg/day)
-
Indications: Every SLE patient unless contraindicated
-
Benefits: Reduces flares, rash, photosensitivity, arthritis, alopecia, malaise; reduces thrombosis in APS; reduces disease progression and long-term damage; improves survival
-
Side effects: Retinopathy (annual ophthalmology screening after 5 years), bone marrow suppression, myocardial toxicity
-
Note: Quinacrine can be added for inadequate response or used as alternative if toxic retinopathy develops
-
Washington Manual of Medical Therapeutics, p. 957
-
Harrison's Principles of Internal Medicine 22E, p. 2875
2. NSAIDs
- Used for: SLE-associated arthritis, arthralgias, fever, mild serositis
- Caution in SLE: Increased risk of aseptic meningitis, hypertension, renal dysfunction, elevated transaminases, increased MI risk with COX-2 inhibitors
- Do NOT rely on for major organ involvement or fatigue/malaise
3. Glucocorticoids
| Situation | Dose |
|---|---|
| Mild-moderate flare (skin/joints/serositis) | Prednisone 0.5 mg/kg/day PO; taper as fast as possible |
| Severe/life-threatening (nephritis, CNS, hemolytic anemia, severe thrombocytopenia) | Prednisone 1-2 mg/kg/day PO or pulse IV methylprednisolone 500-1000 mg IV daily x 3-5 days |
| Maintenance goal | Prednisone ≤5 mg/day (or withdraw completely) |
| Taper rate | Reduce by 10% every 7-10 days once controlled; rapid taper risks relapse |
Key principle: Glucocorticoids are for short-term control. Chronic use should be minimized due to cushingoid effects, hyperglycemia, hypertension, osteoporosis, and avascular necrosis.
- Washington Manual of Medical Therapeutics, p. 957
- Harrison's Principles of Internal Medicine 22E, p. 2876
4. Immunomodulators - Skin & Musculoskeletal Disease
These are used when disease is refractory to HCQ + topical therapies:
| Drug | Dose | Best For |
|---|---|---|
| Methotrexate (MTX) | 10-25 mg/week PO or SC | Skin + musculoskeletal manifestations |
| Azathioprine (AZA) | Standard dosing | Skin, joints; steroid-sparing; safe in pregnancy |
| Mycophenolate mofetil (MMF) | Standard dosing | Moderate-severe skin, arthritis, nephritis |
| Leflunomide | 10-20 mg/day PO | Arthritis, skin |
For cutaneous lupus specifically (Fitzpatrick's/Andrews'):
- Topical/intralesional corticosteroids
- Antimalarials (HCQ)
- Dapsone, thalidomide, sulfasalazine, retinoids, MMF, MTX
- Topical calcineurin inhibitors (generally disappointing for cutaneous LE)
5. Immunosuppressive Therapy - Severe/Life-Threatening Disease
Indications: Glomerulonephritis, CNS involvement, thrombocytopenia, hemolytic anemia, inability to taper steroids.
| Drug | Role |
|---|---|
| Cyclophosphamide (CYC) | Reserved for life-threatening manifestations (severe nephritis, CNS lupus, vasculitis); IV pulse regimen preferred |
| Mycophenolate mofetil (MMF) | At least as effective as CYC for many classes of lupus nephritis with fewer side effects; preferred in young women (preserves fertility) |
| Azathioprine (AZA) | Maintenance therapy after induction; steroid-sparing |
| Rituximab (RTX) | Severe SLE not responding to conventional treatment; refractory cases |
6. Biologics
| Drug | Mechanism | Indication |
|---|---|---|
| Belimumab (BEL) | Anti-BLyS (B lymphocyte stimulator inhibitor) | FDA-approved for autoantibody-positive SLE (2012) and lupus nephritis (2020); added to standard therapy; use for moderate-severe disease unresponsive to HCQ + IS |
| Anifrolumab (ANI) | Anti-interferon-alpha receptor-1 | Moderate-severe SLE with skin/musculoskeletal/hematologic manifestations |
| Voclosporin (CNI) | Calcineurin inhibitor (no drug level monitoring required) | FDA-approved 2021 for lupus nephritis in combination with standard therapy |
7. Lupus Nephritis - Specific Protocol
- Induction: IV methylprednisolone pulses + MMF (preferred) OR cyclophosphamide; Belimumab can be added to MMF as induction
- Maintenance: MMF or AZA
- Add-ons: Voclosporin (CNI) + MMF combination for proteinuria reduction; SGLT2 inhibitors for nephroprotection; ACEi/ARB
- Always continue HCQ throughout
8. Adjunct Therapy (Always Address)
| Measure | Details |
|---|---|
| Sun protection | Broad-spectrum SPF sunscreen; UV-protective clothing; avoid peak sun hours |
| Vaccinations | Influenza (annual), pneumococcal, hepatitis B (before immunosuppression) |
| Smoking cessation | Smoking worsens disease activity and cardiovascular risk |
| Blood pressure control | Target BP <130/80 mmHg especially with nephritis |
| Lipid + glucose control | Accelerated atherosclerosis risk |
| Antiplatelet/anticoagulation | Mandatory if antiphospholipid antibody positive |
| Bone protection | Calcium + Vitamin D if on long-term steroids; bisphosphonates if needed |
| Nephroprotection in LN | ACEi/ARB + SGLT2 inhibitors |
9. Treatment Goals
- Remission: Clinical SLEDAI = 0, prednisone ≤5 mg/day, stable HCQ + IS + biologics
- Low disease activity: SLEDAI ≤4, on HCQ, prednisone ≤7.5 mg/day, stable IS
Quick Reference - Drug Dosing Summary
| Drug | Dose |
|---|---|
| Hydroxychloroquine | 5 mg/kg/day (max 400 mg/d) |
| Prednisone (moderate) | 0.5 mg/kg/day, taper |
| Prednisone (severe) | 1-2 mg/kg/day |
| Methylprednisolone IV pulse | 500-1000 mg/day x 3-5 days |
| Methotrexate | 10-25 mg/week |
| Azathioprine | 1-3 mg/kg/day |
| Mycophenolate mofetil | 2-3 g/day (induction), 1-2 g/day (maintenance) |
| Cyclophosphamide IV | 500-750 mg/m² monthly x 6 cycles (Euro-Lupus: 500 mg x 6 fortnightly) |
Sources:
- Harrison's Principles of Internal Medicine 22E (2025, McGraw Hill), Chapter 368/385
- Washington Manual of Medical Therapeutics, Chapter 25, pp. 957-958
- Firestein & Kelley's Textbook of Rheumatology, Chapter 82 (Fig. 82.1)
- Fitzpatrick's Dermatology, Vol 1-2, Chapter 61
- Andrews' Diseases of the Skin, 13e, Chapter 33
This is a shared conversation. Sign in to Orris to start your own chat.