Inflammatory bowel disease
Reading File
Finding Sources
Finding Sources
Searching PubMed
"inflammatory bowel disease"[MeSH Terms] AND "therapy"[MeSH Terms]
Reading File
Reading File
Finding Sources
Searching PubMed
"inflammatory bowel disease" AND treatment
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have rich, comprehensive content across multiple authoritative textbooks. Let me compile the full answer.
Inflammatory Bowel Disease (IBD)
IBD is a chronic, relapsing-remitting inflammatory condition of the gastrointestinal tract with two main subtypes: Crohn disease (CD) and ulcerative colitis (UC). A third category, "indeterminate colitis," applies when features overlap.
1. Epidemiology
- IBD peaks between ages 15-30 (CD) and 20-40 (UC), with a smaller second peak in the 6th-7th decade for both.
- Sex distribution: CD affects females slightly more (F:M = 1.2:1); UC affects both sexes equally.
- Incidence is highest in Western, industrialized nations; it is increasing in newly industrialized countries, implicating environmental factors.
- Smoking is paradoxically protective against UC but worsens CD.
2. Pathogenesis
The pathogenesis involves a complex interplay of genetics, gut microbiome, immune dysregulation, and environmental factors.
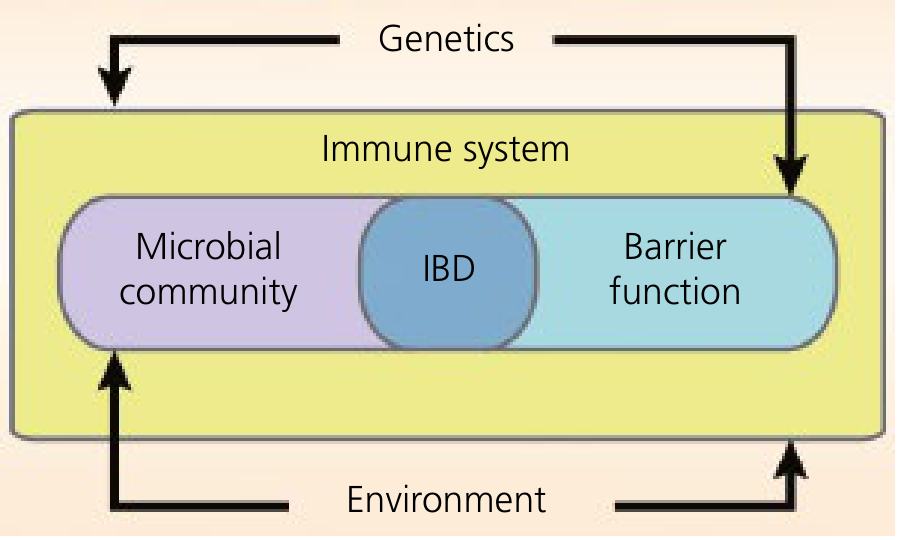
Figure: IBD pathogenesis - breakdown of homeostasis between intestinal epithelium, gut microbiome, and immune response. Genetics and environment exert influence on all components. (Yamada's Textbook of Gastroenterology)
Genetics
- NOD2 (chromosome 16) was the first gene associated with CD - three common polymorphisms (Arg702Trp, Gly908Arg, Leu1007fsX1008). NOD2 senses muramyl dipeptide (MDP) from bacterial cell walls and activates NF-κB signaling.
- ATG16L1 (autophagy-related gene) is another key variant affecting the innate immune response in CD.
- Other relevant SNPs: CARD9, IL18RAP, SLC11A1.
- Over 200 IBD susceptibility loci have been identified by GWAS.
Immune Mechanisms
- CD is characterized by a defective innate immune response to luminal antigens, resulting in exaggerated adaptive Th1/Th17 responses. Key cytokines: TNF-α, IL-12, IL-23, IFN-γ, IL-17.
- UC involves predominantly a Th2-like response with elevated IL-4, IL-5, IL-13.
- Regulatory T cells (Tregs) are impaired in IBD, removing normal brakes on inflammation.
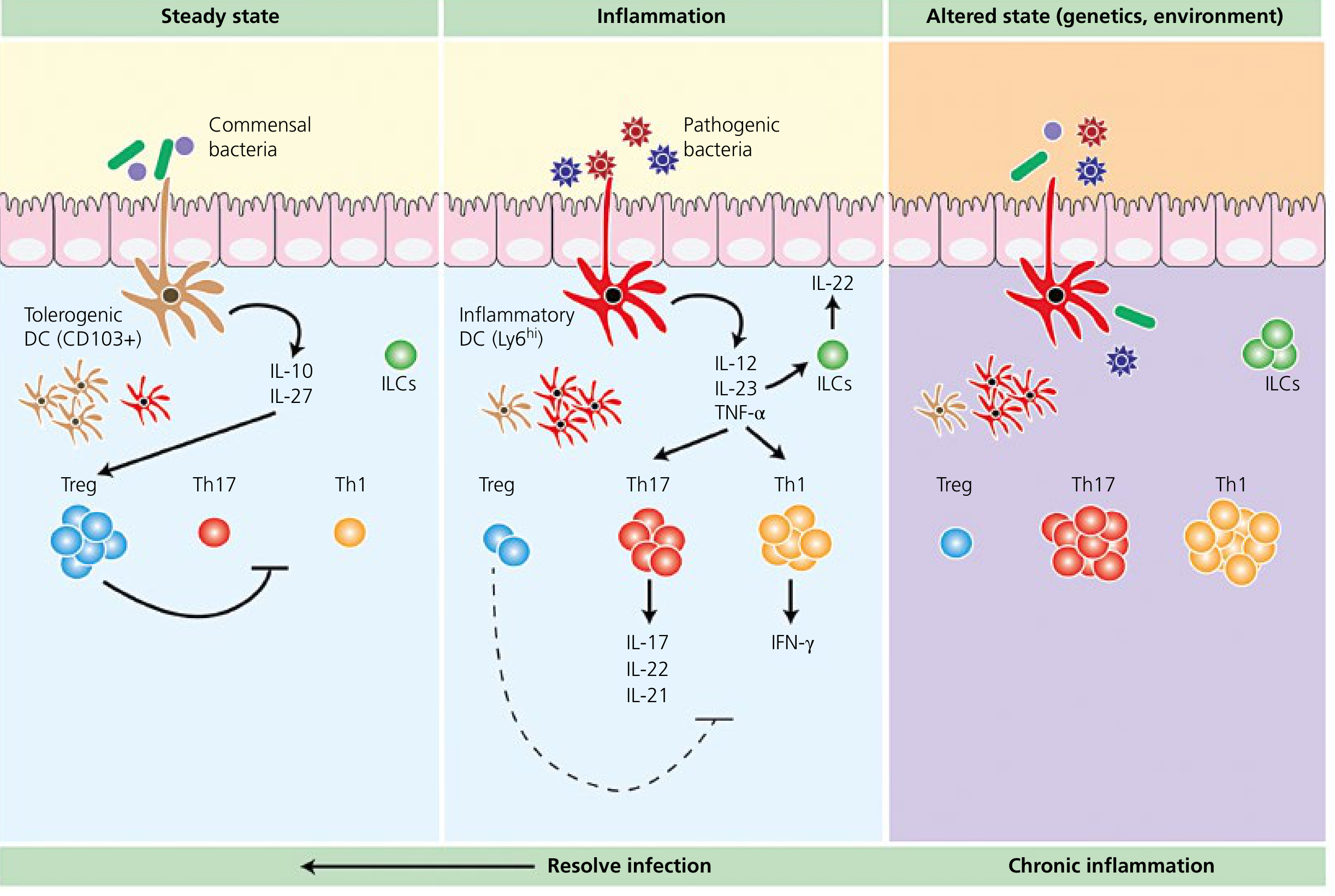
Figure: Host immune perturbations in IBD - alterations in genetics and environment result in chronic mucosal inflammation. (Yamada's Textbook of Gastroenterology)
Microbiome
- Dysbiosis (imbalance of gut microbiota) is central; IBD patients show reduced Firmicutes and Bacteroidetes and increased Proteobacteria.
- Polymorphisms in NOD2 reduce clearance of intracellular bacteria, promoting dysregulated inflammatory responses.
- Antibiotics can modify disease course, supporting a microbial role in pathogenesis.
3. Differentiating CD vs. UC
| Feature | Crohn Disease | Ulcerative Colitis |
|---|---|---|
| Peak onset (years) | 15-30; 2nd peak in 7th decade | 20-40; 2nd smaller peak beyond 7th decade |
| GI involvement | Esophagus to anus ("mouth to anus") | Colon only |
| Skip lesions | Present | Absent (continuous) |
| Transmural inflammation | Yes | No (mucosal/submucosal) |
| Ulceration | Discrete ("cobblestoning") | Continuous |
| Fistulae | Common (20-40%) | Absent |
| Strictures | Common | Rare |
| Perianal disease | Common (up to 30%) | Absent |
| Granulomas | Present (~50%) | Absent |
Source: Goldman-Cecil Medicine, 26th ed.
4. Clinical Features
Crohn Disease
- Terminal ileum is affected in ~70% of cases; pure ileal disease in 30%, ileocolonic in 40%.
- Symptoms: right lower quadrant pain, diarrhea, hematochezia, fatigue, fever, weight loss.
- Obstructive symptoms (distension, nausea) occur with stricturing disease.
- Upper GI involvement (esophageal, gastroduodenal) in <5%; associated with dysphagia, chest pain.
- Fistulae occur in 20-40%: enterocutaneous, rectovaginal, enterovesicular, perianal.
- Perianal disease (fissures, abscesses, skin tags, fistulae) in up to 30%.
Ulcerative Colitis
- Disease starts in the rectum and extends proximally in a continuous pattern.
- At diagnosis: pancolitis in 14-37%, disease beyond the rectum in 36-41%, proctosigmoiditis in 44-49%.
- Symptoms: hematochezia, diarrhea, tenesmus, mucus in stool, urgency, abdominal pain.
- With severe disease: weight loss, fever, hypoalbuminemia, anemia.
- "Backwash ileitis" = spillover inflammation into terminal ileum, not true ileal involvement.
5. Extraintestinal Manifestations
| Complication | CD | UC |
|---|---|---|
| Arthropathy (most common; 10-20%) | + | + |
| Erythema nodosum (10-15%) | + | + |
| Pyoderma gangrenosum (1-2%) | + | + |
| Uveitis / episcleritis (5-15%) | + | + |
| Oral ulcers (aphthous) | + | - |
| Primary sclerosing cholangitis (2-7.5%) | + | + (more with UC) |
| Nephrolithiasis (calcium oxalate; up to 10%) | + | - |
| Ankylosing spondylitis / sacroiliitis | + | + |
Note: 70-80% of patients with primary sclerosing cholangitis have underlying IBD.
6. Diagnosis
Endoscopy
- Colonoscopy (including terminal ileum) is the initial test for lower GI symptoms.
- UC: diffuse mucosal erythema, granular mucosa, loss of vascular pattern, friability, continuous ulceration starting from rectum. Pseudopolyps in chronic disease.
- CD: cobblestone mucosa, discrete ulcers, skip lesions, aphthous ulcers.
- Histology: crypt distortion (both); non-caseating granulomas (CD only).
Radiology
- CT enterography / MRI enterography: gold standard for small bowel CD; identifies strictures, fistulae, abscesses.
- Capsule endoscopy: useful when other tests are non-diagnostic (contraindicated with known strictures; use patency capsule first).
- MRI is preferred over CT for pelvic/perianal disease (less radiation).
Laboratory
- CBC: anemia (iron, B12, folate deficiency), leukocytosis in active/complicated disease.
- ESR, CRP: elevated in active disease (non-specific).
- Fecal calprotectin: elevated in active disease, useful for monitoring.
- Hypoalbuminemia: marker of malnutrition and severe disease.
- Vitamin B12 deficiency: with >100 cm ileal resection or ileal disease.
Serologic Markers
- ASCA (anti-Saccharomyces cerevisiae antibodies): positive in 40-70% of CD, <15% of UC. High ASCA IgA + IgG specificity for CD = 89-100%.
- pANCA: positive in 55% of UC, 20% of CD (colon-predominant).
- ASCA+/pANCA- = high sensitivity for CD; pANCA+/ASCA- = more specific for UC.
7. Treatment
Step 1: 5-Aminosalicylates (5-ASAs)
- Mesalamine (5-ASA): mainstay for mild-moderate UC (induction and maintenance). Topical (suppository/enema) for proctitis/distal disease.
- Sulfasalazine: effective for ileocolonic/colonic CD (response rates 45-55% in mild-moderate disease) but not proven to heal mucosa.
- 5-ASAs are NOT effective for small bowel CD alone.
Step 2: Corticosteroids
- Prednisone (40-60 mg/day): effective for moderate-severe IBD flares; not appropriate for long-term maintenance.
- Budesonide (9 mg/day enteric-coated): preferred for distal ileal/right colonic CD; ~70% response rate at 8 weeks; superior to mesalamine for distal ileal/right colonic disease.
Step 3: Immunomodulators
- Azathioprine (2-3 mg/kg/day) or 6-mercaptopurine (1.5 mg/kg/day): maintenance of remission; slow onset (months).
- Methotrexate (25 mg IM/SC weekly for 16 weeks for active CD; 15-25 mg weekly for maintenance): used for CD, and as combination therapy with biologics to reduce immunogenicity.
- Monitor: CBC, LFTs regularly. Side effects: myelosuppression, hepatotoxicity, pancreatitis, lymphoma risk.
Step 4: Biologics
Anti-TNF-α Agents
- Infliximab (IgG1 chimeric mAb): IV infusion - 5 mg/kg at 0, 2, 6 weeks, then every 8 weeks. Used in moderate-severe CD and UC.
- Adalimumab (fully humanized mAb): SC injection; for moderate-severe CD and UC.
- Certolizumab pegol: pegylated anti-TNF; CD only (US).
- Golimumab: SC injection; UC only.
Anti-integrins (gut-selective)
- Vedolizumab: humanized mAb against α4β7 integrin; blocks lymphocyte recruitment to intestinal mucosa via MAdCAM-1. 300 mg IV at 0, 2, 6 weeks, then every 8 weeks. Approved for moderate-severe CD and UC. Gut-selective = favorable safety profile.
Anti-IL-12/23
- Ustekinumab: fully humanized mAb against the p40 subunit shared by IL-12 and IL-23; prevents Th1 and Th17 activation. IV loading dose (260-520 mg, weight-based), then 90 mg SC every 8 weeks. Approved for moderate-severe CD and UC.
Anti-IL-23 (Selective p19)
- Risankizumab: targets IL-23 p19 subunit selectively; approved for moderate-severe CD and UC.
Antibiotics (CD-specific)
- Metronidazole (10-20 mg/kg/day) and/or ciprofloxacin (500 mg twice daily), 4-8 weeks: primary therapy for perianal fistulae in CD. NOT effective for luminal CD or UC as primary therapy.
Surgery
- UC: colectomy is curative. Indication: medically refractory disease, toxic megacolon, dysplasia, cancer.
- CD: surgery is palliative (not curative). Indications: obstruction, fistulae/abscesses, perforation, refractory disease. Bowel-sparing procedures preferred to avoid short bowel syndrome.
8. Cancer Risk
- UC: CRC risk begins after 7-10 years of disease; rises ~10% per decade; up to 18-34% at 30 years (depends on extent).
- Risk is highest with universal colitis > left-sided colitis > proctitis.
- Surveillance colonoscopy with biopsies every 1-2 years starting after 8-10 years of disease.
- CD: CRC risk is 4-20x the general population, especially with colonic involvement.
- Dysplasia (low-grade to high-grade) is the precursor lesion - characterized by crypt architectural distortion, nuclear enlargement, pseudostratification.
- Aminosalicylate "chemoprevention" is NOT routinely recommended.
9. Recent Evidence (2024-2025)
A 2024 AGA network meta-analysis (Ananthakrishnan et al., Gastroenterology) compared efficacy of advanced therapies for moderate-to-severe UC, providing updated guidance on biologic selection. A 2024 systematic review in Gut (Honap et al.) reviewed acute severe UC trial data. A 2025 Lancet Gastroenterol Hepatol consensus (Hanna et al.) proposed novel diagnostic criteria and management for isolated perianal CD.
Sources:
- Goldman-Cecil Medicine, 26th ed. - Chapter 127
- Yamada's Textbook of Gastroenterology, 7th ed. - Chapter 62
- Goodman & Gilman's Pharmacological Basis of Therapeutics - Chapter 15
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease - Chapter 127
This is a shared conversation. Sign in to Orris to start your own chat.