Hi, I'm a year 4 mbbs student studying in Aimst university, Malaysia. Currently I'm in optal posting and having case presentation exam. I only have a rough history: Hasnah binti Ahmad 67 years SP0024086 Female, Malay DOA : 30/4/26, 9am Doc : 30/4 C/o Blurry vision HOPI 2 weeks a/w redness, LE glare Past History Thyroid disease 1 year diagnosis Dx : Graves ophthalmopathy, moderate to severe --- Physical Exam General Alert Sitting upright Oriented to tpp Prominent conjunctival redness Specific (thyroid) not done Ocular Lower lid retraction Injected conjunctiva Corneal haziness (exposure keratopathy) Periorbital swelling. Can you create a good presentation report for my exam please including the differentials, investigation and management
Graves ophthalmopathy management
CASE PRESENTATION REPORT
Opthalmology Posting — MBBS Year 4 | AIMST University
COVER PAGE
1. BIODATA
| Name | Hasnah binti Ahmad |
| Age | 67 years |
| Sex | Female |
| Race | Malay |
| Religion | Islam (presumed) |
| Hospital No. | SP0024086 |
| DOA | 30/04/2026 |
| Ward | Ophthalmology |
2. CHIEF COMPLAINT
3. HISTORY OF PRESENTING ILLNESS
- Redness of the left eye (LE)
- Glare/photophobia of the left eye
- Severity and progression of blurry vision (VA before vs. now)
- Any diplopia (double vision)?
- Any difficulty closing the eyes, especially during sleep (lagophthalmos)?
- Any sensation of grittiness or foreign body in the eye?
- Any colour vision changes (suggests optic nerve involvement)?
- Any proptosis noticed by patient or family?
4. PAST MEDICAL HISTORY
| Condition | Duration | Treatment |
|---|---|---|
| Thyroid disease (Graves' disease) | 1 year | Not documented — to be clarified |
- No known history of diabetes mellitus, hypertension, or ischaemic heart disease documented
- No prior ocular surgery or trauma
5. PAST SURGICAL HISTORY
6. DRUG & ALLERGY HISTORY
- Current thyroid medication: to be clarified (carbimazole / propylthiouracil / radioiodine / thyroxine?)
- No known drug allergy documented.
Note: If the patient underwent radioiodine therapy, this is a significant risk factor for worsening TED and must be documented.
7. FAMILY HISTORY
8. SOCIAL HISTORY
- Smoking history: Must be specifically elicited — smoking is the major modifiable risk factor for progression of TED. The greater the number of cigarettes smoked per day, the greater the risk; cessation reduces risk.
- Occupation, living situation, functional status — relevant given age 67.
9. SYSTEMIC REVIEW
- Thyrotoxic symptoms: weight loss despite good appetite, palpitations, heat intolerance, increased sweating, tremors, loose stools, irritability, menstrual irregularities
- Current thyroid status: Is patient euthyroid, hyperthyroid or hypothyroid?
10. PHYSICAL EXAMINATION
General Examination
- Alert, sitting upright, orientated to time, place, and person
- Prominent conjunctival redness noted on inspection
- To complete: Build (weight loss?), fine tremor of outstretched hands, pulse rate (tachycardia?), skin (warm, sweaty, palmar erythema), pre-tibial myxoedema, thyroid acropachy
Thyroid Examination
- Not performed (to be done — assess for goitre: diffuse enlargement, bruit, thrill)
Specific Ocular Examination
Visual Acuity (VA)
- Not documented — must be measured with Snellen chart (unaided and aided)
- Critical to determine if there is sight-threatening disease (optic neuropathy)
External Examination / Adnexa
| Sign | Findings |
|---|---|
| Lower lid retraction | Present |
| Periorbital swelling | Present |
- Upper lid signs to look for: Dalrymple sign (widened palpebral aperture), von Graefe sign (lid lag on down-gaze), Kocher sign (staring, frightened appearance)
- Proptosis: Assess with Hertel exophthalmometer — >20 mm or asymmetry >2 mm is significant
Anterior Segment
| Sign | Findings |
|---|---|
| Injected conjunctiva | Present — bilateral epibulbar hyperaemia (sensitive sign of inflammatory activity; may outline insertions of horizontal recti) |
| Corneal haziness | Present — exposure keratopathy secondary to incomplete lid closure |
- Further slit-lamp findings to assess: Corneal fluorescein staining (punctate epithelial erosions), corneal thinning/scarring, superior limbic keratoconjunctivitis
Extraocular Movements (EOM)
- Not documented — assess for restriction, especially upgaze (inferior rectus involvement) or diplopia
Fundoscopy / Posterior Segment
- Not documented — must be performed to rule out disc swelling or optic atrophy (signs of compressive optic neuropathy — the most serious complication)
11. CLINICAL ACTIVITY SCORE (CAS) — EUGOGO
| # | Feature | Present? |
|---|---|---|
| 1 | Spontaneous retrobulbar pain | ? |
| 2 | Pain on up- or down-gaze | ? |
| 3 | Redness of the eyelids | — |
| 4 | Redness of the conjunctiva | ✓ (injected conjunctiva) |
| 5 | Swelling of the eyelids | ✓ (periorbital swelling) |
| 6 | Inflammation of the caruncle or plica | ? |
| 7 | Chemosis | ? |
12. SEVERITY CLASSIFICATION — EUGOGO
| Severity | Criteria |
|---|---|
| Mild | Lid retraction <2 mm, mild soft tissue involvement, proptosis <3 mm above normal, no diplopia |
| Moderate-to-Severe | Lid retraction ≥2 mm, moderate-severe soft tissue signs, proptosis ≥3 mm above normal, intermittent or constant diplopia |
| Sight-Threatening | Compressive optic neuropathy ± corneal breakdown |
13. DIAGNOSIS
14. DIFFERENTIAL DIAGNOSES
| # | Differential | Supporting Features | Differentiating Features |
|---|---|---|---|
| 1. Orbital cellulitis | Periorbital swelling, redness, blurry vision | Fever, pain, proptosis, reduced EOM — acute presentation; no thyroid history | |
| 2. Idiopathic orbital inflammatory disease (orbital pseudotumour) | Periorbital oedema, injection, proptosis | Painful proptosis, unilateral, no thyroid disease association; responds well to steroids | |
| 3. Cavernous sinus thrombosis | Periorbital swelling, conjunctival injection | Severe headache, fever, bilateral signs, altered consciousness, CN III/IV/VI/V palsies | |
| 4. Conjunctivitis (bacterial/viral/allergic) | Redness, blurry vision, foreign body sensation | No lid retraction, no proptosis, no systemic thyroid disease; discharge often present | |
| 5. Ocular myasthenia gravis | Diplopia, ptosis, fatigable EOM | Ptosis rather than lid retraction, fatigability on sustained upgaze, positive edrophonium/ice test, anti-AChR antibodies | |
| 6. Superior ophthalmic vein thrombosis | Proptosis, chemosis, engorgement | Often secondary to cavernous sinus pathology; no thyroid disease | |
| 7. Orbital lymphoma / metastasis | Proptosis, periorbital mass | Firm mass on palpation, painless, no inflammatory features, CT/MRI shows discrete mass |
15. INVESTIGATIONS
A. Thyroid Function & Autoimmunity
| Investigation | Rationale |
|---|---|
| TSH (Thyroid Stimulating Hormone) | First-line; suppressed in hyperthyroidism |
| Free T3 & Free T4 | Confirm hyperthyroid state |
| TSH receptor antibodies (TRAb) / TSHR-Ab | Pathognomonic of Graves' disease; elevated in ~95% of TED |
| Anti-TPO antibody, Anti-Tg antibody | Associated autoimmune thyroid disease |
B. Ocular Investigations
| Investigation | Rationale |
|---|---|
| Snellen visual acuity (best corrected) | Baseline; monitor for optic neuropathy |
| Colour vision testing (Ishihara) | Desaturated colour vision = early optic nerve compression |
| Slit-lamp examination with fluorescein staining | Assess corneal epithelial defects (exposure keratopathy severity) |
| Hertel exophthalmometry | Measure proptosis quantitatively |
| Intraocular pressure (IOP) in primary and upgaze | Elevated IOP on upgaze suggests inferior rectus tethering |
| Visual fields (Humphrey perimetry) | Assess for field defects from optic nerve compression |
| Fundoscopy | Disc swelling, optic atrophy, choroidal folds |
C. Imaging
| Investigation | Rationale |
|---|---|
| CT orbit (axial + coronal, with contrast) | Gold standard — shows enlarged extraocular muscles (typically inferior and medial recti), orbital fat expansion, apical crowding |
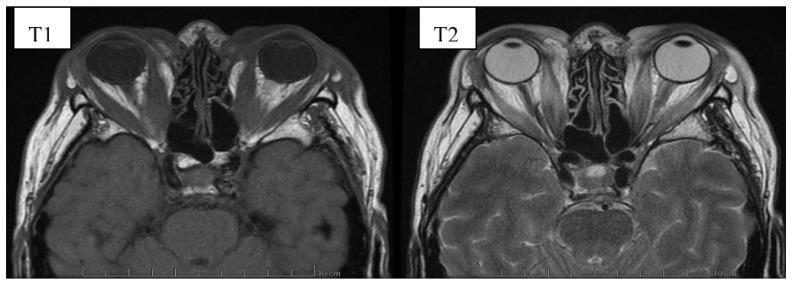
| MRI orbit | Superior soft tissue detail; T2-weighted signal indicates muscle inflammation (active disease) |
| Thyroid ultrasound | Assess thyroid size, vascularity (hypervascular in Graves') |
D. General
| Investigation | Rationale |
|---|---|
| FBC | Baseline before starting steroids/immunosuppression; carbimazole can cause agranulocytosis |
| Fasting glucose / HbA1c | Rule out DM before steroid therapy; Graves' can cause glucose intolerance |
| LFTs | Baseline before steroid/immunosuppressive therapy; IV steroids contraindicated in significant hepatic dysfunction |
| Selenium level | Adjunct — selenium deficiency associated with TED; supplementation shown to slow progression |
| ECG | Thyrotoxicosis can cause AF; check before treatment |
16. MANAGEMENT
Immediate Priorities
- Refer to combined Ophthalmology + Endocrinology clinic
- Ensure euthyroid state — active TED is worsened by thyroid dysfunction in either direction
- Smoking cessation counselling — most important modifiable risk factor
A. Conservative (Supportive)
| Measure | Detail |
|---|---|
| Topical lubricants (artificial tears / lubricating ointment) | Relieve ocular surface symptoms from corneal exposure |
| Nocturnal eyelid taping | Prevents lagophthalmos and nocturnal corneal desiccation |
| Head elevation during sleep (3 pillows) | Reduces periorbital oedema |
| Sunglasses | Relieve photophobia/glare |
| Selenium supplementation | Sodium selenite 200 µg daily for 6 months in selenium-deficient patients — shown to improve quality of life and slow disease progression (double-blind RCT evidence) |
B. Medical — Moderate-to-Severe Active TED
- IV Methylprednisolone (preferred over oral — superior efficacy, better safety profile):
- 500 mg IV once weekly × 6 weeks, then 250 mg IV once weekly × 6 weeks
- Advantages: Higher treatment response, longer period to retreatment
- Contraindications: Significant hepatic dysfunction, cardiovascular disease, uncontrolled hypertension, uncontrolled diabetes
- Oral Prednisolone: 60–80 mg/day, tapered over months — used if IV not available; efficacy 33–63%
- IV methylprednisolone weekly + Mycophenolate sodium (0.72 g/day for 24 weeks) — superior to IV steroids alone; less disease reactivation
- Methotrexate — monotherapy if steroids not tolerated or patient is steroid-dependent
- Azathioprine — combined with radiotherapy or steroids (not effective alone)
- Teprotumumab (anti-IGF-1R antibody) — significant proptosis reduction; now first-line in some centres
- Tocilizumab (anti-IL-6R) — evidence of efficacy, especially steroid-refractory TED
- Rituximab (anti-CD20) — positive results in some trials; used in refractory cases
- Ensure and maintain euthyroid state (carbimazole / propylthiouracil / surgery)
- If radioiodine is planned, cover with a short course of oral steroids to prevent TED flare
C. Orbital Radiotherapy
- Second-line adjunct for soft tissue changes and EOM restriction
- 20 Gy in 10 fractions over 2 weeks
- Response evident at 6 weeks; maximal at 4 months (~40% non-responders)
- Used with steroids (not as sole treatment for acute optic neuropathy)
- Contraindicated in patients with diabetes (risk of radiation retinopathy)
D. Surgical Rehabilitation (Inactive Disease — Done in Sequence)
| Order | Procedure | Indication |
|---|---|---|
| 1st | Orbital decompression | Sight-threatening optic neuropathy; severe proptosis; cosmesis. Medial ± inferior ± lateral wall; endoscopic transnasal approach. Reduces proptosis 3.2–5.1 mm |
| 2nd | Strabismus surgery | Residual diplopia after decompression settles |
| 3rd | Eyelid surgery | Lid retraction correction (lower lid spacer graft, levator recession); exposure keratopathy |
E. Management of Exposure Keratopathy (This Patient)
- Intensive topical lubricants (preservative-free drops q1–2h + ointment at night)
- Eyelid taping at night
- Consider temporary tarsorrhaphy if keratopathy progresses despite conservative measures
- Urgent review if corneal staining worsens — risk of corneal ulceration/perforation
17. PROGNOSIS
- Most patients (>90%) with mild-moderate TED remain stable or improve over 1–3 years
- Moderate-to-severe disease may have residual soft tissue changes, proptosis, or diplopia even after treatment
- Smoking significantly worsens prognosis
- Sight-threatening complications (corneal ulceration, optic neuropathy) can cause permanent visual loss if untreated
18. PATIENT COUNSELLING POINTS
- TED is an autoimmune condition linked to her thyroid disease — managing the thyroid is essential
- Stop smoking — this is the single most important lifestyle modification
- Explain the natural history: active phase (6–24 months) followed by inactive/stable phase
- Surgery (if needed) is only done after the disease is stable — not during the active phase
- Regular follow-up with both ophthalmology and endocrinology is mandatory
- Side effects of steroid therapy must be discussed: weight gain, mood changes, glucose intolerance, peptic ulcer disease, osteoporosis, avascular necrosis of hip
SUMMARY STATEMENT (for oral presentation)
"Madam Hasnah binti Ahmad is a 67-year-old Malay female with a 1-year history of Graves' disease who presented with a 2-week history of blurry vision associated with left eye redness and glare. On examination, she was alert and orientated, with lower lid retraction, injected conjunctiva, corneal haziness consistent with exposure keratopathy, and periorbital swelling. These findings are in keeping with a diagnosis of Graves' Ophthalmopathy, moderate-to-severe severity, currently in the active phase. Management priorities include confirming thyroid status, quantifying ocular involvement with CAS scoring, initiating IV methylprednisolone with mycophenolate for active disease, intensive topical lubricants for corneal protection, and strict smoking cessation counselling. Combined ophthalmology-endocrinology follow-up is essential."
- Always state the CAS score — examiners love this scoring system
- The sequence of surgery (decompression → strabismus → eyelid) is a classic exam favourite
- Emphasise smoking cessation as the #1 modifiable risk factor
- Know the contraindications to IV steroids (hepatic dysfunction, uncontrolled DM/HPT, CV disease)
- For this patient, the corneal haziness needs urgent attention — mention tarsorrhaphy as an option
Can you give expected viva questions for this presentation and prepare me for the case
VIVA PREPARATION GUIDE
Graves' Ophthalmopathy | Hasnah binti Ahmad
HOW EXAMINERS BUILD THE VIVA
Diagnosis → Mechanism → Classification → Signs → Investigations → Management → Complications → Emergencies → Exam-specific traps
BLOCK 1 — DIAGNOSIS & DEFINITIONS
"My diagnosis is Graves' Ophthalmopathy, moderate-to-severe severity, in the active phase. I arrived at this based on:
- Known history of Graves' disease (thyroid disease diagnosed 1 year ago)
- Clinical triad of lid retraction, periorbital swelling, and injected conjunctiva
- Corneal haziness consistent with exposure keratopathy — a direct complication of lid retraction and proptosis
- Blurry vision and glare, indicating ocular surface compromise Severity is classified as moderate-to-severe because of the combination of lid retraction, significant soft tissue involvement, and corneal compromise."
"Graves' Ophthalmopathy, also called Thyroid Eye Disease (TED) or thyroid-associated orbitopathy, is an autoimmune inflammatory condition of the orbit and periorbital tissues. It is the most common cause of both unilateral and bilateral proptosis in adults. It is most commonly associated with Graves' disease but can occur in euthyroid patients and, rarely, in Hashimoto's thyroiditis."
"Yes. About 10% of TED patients are euthyroid at presentation. These individuals usually have anti-thyroid antibodies or autoimmune hypothyroidism. The onset of TED can precede, coincide with, or follow the diagnosis of thyrotoxicosis — in 75% of cases it occurs within 1 year of thyroid diagnosis."
BLOCK 2 — PATHOPHYSIOLOGY
"The underlying mechanism is autoimmune. TSH receptor antibodies (TRAb/TSHR-Ab) that drive Graves' hyperthyroidism also bind to TSH receptors expressed on orbital fibroblasts. This triggers:
- Proliferation of orbital fibroblasts → differentiate into adipocytes (fat expansion) or myofibroblasts
- Upregulation of IGF-1 receptor on fibroblasts (synergises with TSH receptor activation)
- Glycosaminoglycan (hyaluronic acid) accumulation → osmotic water retention → orbital oedema
- Extraocular muscle enlargement — primarily the muscle belly (spares tendons, unlike orbital myositis)
- The net result is increased orbital volume in a rigid bony orbit → proptosis, compressive optic neuropathy, venous congestion"
"Two mechanisms:
- Sympathetic overstimulation of Müller's muscle (smooth muscle) due to high circulating thyroid hormones — occurs in any thyrotoxic state
- Fibrotic contracture of the levator palpebrae and inferior rectus muscles with adhesion to overlying orbital tissues — specific to Graves' ophthalmopathy Lower lid retraction is caused by fibrosis and tethering of the inferior rectus to the lower lid retractors."
"The mnemonic is I'M SLow (in order of frequency):
- Inferior rectus — most commonly
- Medial rectus — second
- Superior rectus/levator complex
- Lateral rectus — least common
Importantly, the muscle belly is enlarged but tendons are spared — this helps distinguish TED from orbital myositis on CT/MRI."
BLOCK 3 — CLINICAL SIGNS
Lid signs:
- Dalrymple sign — lid retraction in primary gaze (widened palpebral fissure)
- von Graefe sign — lid lag on downgaze (upper lid fails to follow globe)
- Kocher sign — staring/frightened expression on attentive fixation
- Stellwag sign — infrequent blinking
Soft tissue signs:
- Periorbital oedema
- Conjunctival injection / epibulbar hyperaemia (especially overlying horizontal recti insertions)
- Chemosis
- Caruncular/plical swelling
Proptosis (exophthalmos)EOM restriction → diplopia (typically upgaze first, due to inferior rectus tethering)Corneal signs: Punctate epithelial erosions, exposure keratopathy, superior limbic keratoconjunctivitisOptic nerve signs: Disc swelling, optic atrophy, reduced acuity, colour vision loss, RAPD, field defects
"Dalrymple sign is lid retraction in primary gaze — the upper lid sits above the superior limbus, revealing scleral show. Von Graefe sign is lid lag on downgaze — the upper lid fails to descend at the same speed as the globe when the patient looks down."
"The corneal haziness is due to exposure keratopathy. Lower lid retraction (present in this patient) causes the lower cornea to be constantly exposed. Combined with incomplete lid closure (lagophthalmos), the corneal epithelium desiccates, breaks down, and can develop punctate erosions, corneal haze, and if severe — ulceration, secondary bacterial infection, and corneal scarring. This is a serious complication that can permanently affect vision."
BLOCK 4 — CLASSIFICATION SYSTEMS
"The preferred system is the EUGOGO (European Group on Graves' Orbitopathy) classification:
Severity Features Mild Lid retraction <2 mm, mild soft tissue signs, proptosis <3 mm above normal, no diplopia, normal VA Moderate-to-Severe Lid retraction ≥2 mm, moderate/severe soft tissue signs, proptosis ≥3 mm above normal, intermittent/constant diplopia Sight-Threatening Compressive optic neuropathy OR corneal breakdown This patient classifies as Moderate-to-Severe based on lid retraction, periorbital swelling, injected conjunctiva, and corneal compromise."
"The CAS is a 7-point scoring system to assess inflammatory activity — it tells us whether the disease is active (and will respond to immunosuppression) versus inactive (and requires surgical rehabilitation).One point is given for each:
- Spontaneous retrobulbar pain
- Pain on eye movement
- Eyelid redness
- Conjunctival injection ✓
- Periorbital/eyelid swelling ✓
- Chemosis
- Inflammation of caruncle/plica
CAS ≥ 3/7 = active disease → immunosuppressive treatment warrantedThis patient scores at least 2 from documented findings; further assessment needed for the full score."
"NO SPECS is a mnemonic for the 7 classes of TED:
- 0 = No signs or symptoms
- I = Only signs (lid retraction/lag)
- II = Soft tissue involvement (periorbital oedema, chemosis)
- III = Proptosis (>22 mm)
- IV = EOM involvement (diplopia)
- V = Corneal involvement
- VI = Sight loss (optic neuropathy)
It is now considered inadequate because patients don't necessarily progress sequentially. EUGOGO + CAS are preferred in modern practice."
BLOCK 5 — INVESTIGATIONS
"TSH receptor antibodies (TRAb/TSHR-Ab). They are elevated in ~95% of patients with TED and are pathognomonic of Graves' disease. They also correlate with disease activity and can be used to monitor treatment response."
"CT orbit (axial and coronal, with contrast) is the gold standard. Expected findings:
- Enlarged extraocular muscle bellies with tendon sparing (distinguishes from orbital myositis)
- Predominant enlargement of inferior and medial recti
- Increased orbital fat volume
- Apical crowding — muscles crowding the orbital apex, compressing the optic nerve at the orbital apex — this is the mechanism of compressive optic neuropathy
MRI orbit is preferred for soft tissue detail and uses T2-weighted signal to assess inflammation/activity — bright T2 = active, inflammatory muscles."
"Fluorescein staining under cobalt blue light on slit lamp reveals corneal epithelial defects. Punctate staining indicates superficial punctate keratopathy from exposure. Larger defects indicate epithelial erosions or frank ulceration. This determines the urgency of corneal protection — if large or central, urgent intervention (tarsorrhaphy) is needed to prevent vision-threatening corneal scarring."
BLOCK 6 — MANAGEMENT
"My management is based on Moderate-to-Severe, Active TED. I would approach it in three pillars:1. Supportive:
- Intensive topical lubricants (preservative-free, q1–2h during day + ointment at night)
- Nocturnal eyelid taping to prevent corneal desiccation
- Head elevation during sleep
- Smoking cessation counselling — the most important modifiable risk factor
2. Medical (Active Disease):
- First-line: IV Methylprednisolone 500 mg weekly × 6 weeks, then 250 mg weekly × 6 weeks
- Combined with Mycophenolate sodium 0.72 g/day for 24 weeks for superior outcomes
- Monitor LFTs, blood glucose, blood pressure
- Ensure and maintain euthyroid state throughout
3. Surgical (only when disease is inactive/stable — ≥6 months):
- Done in strict sequence: orbital decompression → strabismus surgery → eyelid surgery
For this patient specifically: The corneal haziness requires urgent attention — intensive lubricants, eyelid taping; if the cornea deteriorates, consider temporary tarsorrhaphy."
"IV methylprednisolone is superior to oral prednisolone in TED for three reasons:
- Better efficacy — higher response rate and longer time before needing retreatment
- Better safety profile — lower cumulative dose, fewer systemic side effects
- Faster onset of soft tissue response The oral route is used only when IV is unavailable or not tolerated. However, IV steroids are contraindicated in significant hepatic dysfunction, major cardiovascular disease, uncontrolled hypertension, or uncontrolled diabetes."
"Selenium supplementation — sodium selenite 200 µg/day for 6 months — has Level 1 evidence (double-blind RCT) showing:
- Improved quality of life
- Decreased soft tissue involvement
- Slowed disease progression in mild, active TED The benefit is greatest in selenium-deficient populations. It acts via selenoproteins, which regulate oxidative stress and T3 production. Serum levels should be monitored as excess selenium is associated with diabetes, neurotoxicity, and glaucoma."
"The sequence is strictly: Decompression → Strabismus → Eyelid
- Orbital decompression first — because it changes orbital anatomy, which can induce or change strabismus. If you do strabismus surgery first, the decompression will undo your correction.
- Strabismus surgery second — corrects diplopia after the orbit has been decompressed and stabilised.
- Eyelid surgery last — because strabismus surgery changes orbital and lid mechanics; lid surgery should be the final refinement.
All surgery is done only when the disease has been inactive and stable for ≥6 months."
"Teprotumumab is a monoclonal antibody targeting the IGF-1 receptor (IGF-1R) on orbital fibroblasts. Since IGF-1R synergises with TSH receptor signalling in TED pathogenesis, blocking it reduces orbital fibroblast activation. Clinical trials have shown significant reduction in proptosis and CAS. It is now approved by the FDA and used as first-line therapy for moderate-to-severe TED in some centres, particularly in the United States."
BLOCK 7 — COMPLICATIONS & EMERGENCIES
"Dysthyroid optic neuropathy (DON) — compression of the optic nerve at the orbital apex by enlarged extraocular muscles. It is sight-threatening and constitutes an ophthalmological emergency.Features to recognise:
- Reduced visual acuity (especially colour vision — use Ishihara plates)
- Relative afferent pupillary defect (RAPD)
- Visual field defects (central scotoma, inferior altitudinal defect)
- Disc swelling on fundoscopy
Management: IV methylprednisolone 1 g/day × 3 days — if no improvement in 2 weeks, urgent orbital decompression surgery."
"Red flags requiring urgent intervention:
- Large/central fluorescein staining defect
- Corneal ulceration — risk of perforation and endophthalmitis
- Secondary bacterial keratitis
- Corneal thinning/descemetocele
Action: Urgent temporary tarsorrhaphy (lateral or central), intensive topical lubricants + antibiotics if infected, admit the patient."
"Systemic: glucose intolerance, weight gain, mood changes/psychosis, peptic ulcer disease (cover with PPI), hypertension, osteoporosis (calcium + vitamin D supplementation), avascular necrosis of the femoral head.Hepatic: acute liver injury (rare but potentially fatal) — LFTs must be checked before and during treatment. Contraindicated if significant liver disease.Ophthalmological: posterior subcapsular cataract, raised intraocular pressure."
BLOCK 8 — RISK FACTORS & ASSOCIATIONS
"1. Smoking — the strongest modifiable risk factor; dose-dependent relationship; cessation reduces risk 2. Radioiodine therapy — can precipitate or worsen TED; cover with steroids if TED is pre-existing 3. Female sex — 5× more commonly affected (though largely reflects Graves' disease incidence) 4. High TRAb levels — correlate with TED severity 5. Thyroid dysfunction — both hyper- and hypothyroidism worsen TED; euthyroid state is protective"
"Smoking is the single most important modifiable risk factor for TED. It increases the risk of developing TED in Graves' patients, worsens severity, and reduces response to treatment (including radioiodine and immunosuppression). Smoking cessation should be the very first intervention offered, regardless of TED severity."
BLOCK 9 — CLASSIC EXAM TRAPS
"Yes, absolutely. In 75% of patients, TED onset occurs within 1 year before or after the diagnosis of thyrotoxicosis. The conditions are autoimmune siblings sharing the TSH receptor as the target antigen. TED can even precede thyroid disease by several years or appear in fully euthyroid patients."
"Lower lid retraction in TED is caused by fibrosis and adhesion of the inferior rectus muscle to the lower lid retractors (capsulopalpebral fascia). As the inferior rectus becomes fibrotic and tethered, it pulls the lower lid downward, revealing inferior scleral show. Upper lid retraction, on the other hand, is from levator/Müller's overaction."
"No. Normal VA at presentation does not exclude early dysthyroid optic neuropathy (DON). Colour vision loss, particularly red desaturation, is often the earliest sign of optic nerve compression — it may be abnormal before Snellen acuity drops. RAPD and visual field defects may also precede VA loss. This is why a full ocular assessment including colour vision, Humphrey fields, and fundoscopy is mandatory."
"Yes. Although TED is most commonly associated with Graves' disease (~95% of cases), it can occur with:
- Hashimoto's thyroiditis (rarely)
- Euthyroid Graves' (10%) — TED with normal thyroid function tests but positive TRAb
- Post-radioiodine hypothyroidism The diagnosis in euthyroid cases is primarily clinical, supported by TRAb positivity and orbital imaging."
"Clinically used interchangeably, but technically:
- Proptosis = any anterior displacement of the globe from any cause
- Exophthalmos = proptosis specifically due to endocrine/thyroid-related orbital disease
Measured with a Hertel exophthalmometer. Normal <20 mm; asymmetry >2 mm is significant. In TED, >20 mm constitutes proptosis."
"Any of the following:
- Reduced visual acuity unexplained by corneal or lens pathology
- Loss of colour vision (red desaturation)
- RAPD
- Visual field defects
- Disc swelling or optic atrophy on fundoscopy
- Corneal ulceration / descemetocele / perforation
These indicate either compressive optic neuropathy or corneal breakdown — both are ophthalmological emergencies requiring immediate IV methylprednisolone and/or urgent orbital decompression."
QUICK-FIRE SUMMARY TABLE
| Question | Key Answer |
|---|---|
| Most common cause of bilateral proptosis in adults | Graves' Ophthalmopathy |
| Autoantibody responsible | TSH receptor antibody (TRAb) |
| Most commonly enlarged EOM | Inferior rectus |
| Most important modifiable RF | Smoking |
| Activity scoring system | Clinical Activity Score (CAS) — ≥3/7 = active |
| Severity classification | EUGOGO (Mild / Moderate-Severe / Sight-threatening) |
| First-line treatment for moderate-severe active | IV Methylprednisolone + Mycophenolate |
| Surgical sequence | Decompression → Strabismus → Eyelid |
| Earliest sign of optic neuropathy | Colour vision loss (red desaturation) |
| Emergency management of DON | IV methylprednisolone 1g/day × 3 days → decompression |
| Selenium dose | 200 µg/day × 6 months (mild active TED) |
| IV steroid regimen (mod-severe) | 500 mg weekly × 6 weeks, then 250 mg × 6 weeks |
| Imaging of choice | CT orbit (axial + coronal) |
| CT hallmark finding | Muscle belly enlargement with tendon sparing |
Graves' Ophthalmopathy 101 please
Graves ophthalmopathy thyroid eye disease proptosis lid retraction clinical signs
Graves ophthalmopathy pathogenesis orbital fibroblast GAG mechanism diagram
GRAVES' OPHTHALMOPATHY 101
A Complete Visual Guide for the MBBS Student
1. WHAT IS IT?
- Thyroid Eye Disease (TED) ← most modern term
- Thyroid-Associated Orbitopathy (TAO)
"TED is the most common cause of both unilateral and bilateral proptosis in adults." — Kanski's Clinical Ophthalmology, 10th Ed.
2. WHO GETS IT?
| Factor | Detail |
|---|---|
| Most common association | Graves' disease (autoimmune hyperthyroidism) — ~95% |
| Can occur in euthyroid | ~10% — called "euthyroid Graves' ophthalmopathy" |
| Can occur in hypothyroid | Rarely — e.g. Hashimoto's thyroiditis |
| Sex | Females 5× more common (mirrors Graves' disease incidence) |
| Age | 4th–5th decade typical; but any age |
| Timing vs thyroid disease | 75% of cases: TED occurs within 1 year before or after thyroid diagnosis |
Risk Factors
🚬 Smoking ————————→ #1 modifiable risk factor (dose-dependent)
☢️ Radioiodine therapy → can precipitate/worsen TED
⬆️ High TRAb levels ——→ predicts TED severity
❌ Thyroid dysfunction —→ both hyper- AND hypo- worsen TED
3. PATHOGENESIS — HOW DOES IT HAPPEN?
STEP 1: AUTOIMMUNE TRIGGER
TSH receptor antibodies (TRAb) are produced
↓
STEP 2: ORBITAL FIBROBLAST ACTIVATION
TRAb binds TSH receptors (TSHR) on orbital fibroblasts
IGF-1 receptor (IGF-1R) is also upregulated — synergises
↓
STEP 3: TWO PARALLEL PROCESSES
(A) Fibroblasts → ADIPOCYTES → orbital FAT EXPANSION
(B) Glycosaminoglycan (hyaluronic acid) secretion
→ osmotic water retention → EXTRAOCULAR MUSCLE SWELLING
→ muscles can swell up to 8× their normal size
↓
STEP 4: CONSEQUENCES
Increased orbital volume in a RIGID BONY BOX
→ Proptosis (globe pushed forward)
→ Apical crowding → optic nerve compression
→ Lid retraction, EOM restriction, corneal exposure
Key teaching point: This is why we treat early (active phase) — once fibrosis sets in, anti-inflammatory treatment no longer works.
4. CLINICAL FEATURES — THE BIG PICTURE
| Phase | Also Called | Eyes Look | Duration | Treatment works? |
|---|---|---|---|---|
| Active (Congestive) | Inflammatory | Red, swollen, painful | 6 months – 3 years | ✅ YES — steroids/immunosuppression |
| Inactive (Fibrotic) | Quiescent | White, quiet | Permanent | ❌ Anti-inflammatory no longer helps → surgery |
5. CLINICAL SIGNS — HEAD TO TOE
Clinical Photo: Active TED Before & After Treatment

A. LID SIGNS
| Sign | What It Means | How to Elicit |
|---|---|---|
| Dalrymple sign | Lid retraction in primary gaze — upper lid sits above superior limbus (scleral show) | Look at patient in primary gaze |
| von Graefe sign | Lid lag on downgaze — lid doesn't descend with globe | Ask patient to follow your finger slowly downward |
| Kocher sign | Staring, frightened expression on attentive fixation | Observe patient looking at a target |
| Stellwag sign | Infrequent blinking | Count blinks per minute |
Memory tip: "Dalrymple = Daytime (primary gaze) | von Graefe = vertical downgaze"
- Sympathetic overstimulation of Müller's muscle (any thyrotoxic state)
- Fibrotic contracture of levator palpebrae adhesion to orbital tissues (specific to GO)
B. SOFT TISSUE SIGNS
- Periorbital oedema — caused by oedema and fat infiltration behind the orbital septum
- Conjunctival injection — especially epibulbar hyperaemia overlying the horizontal recti insertions (sensitive activity sign)
- Chemosis — conjunctival oedema/boggy appearance
- Caruncle/plica swelling
- Tear insufficiency — very common, causes grittiness
C. PROPTOSIS (EXOPHTHALMOS)
- Globe displaced anteriorly due to increased orbital volume
- Measured with Hertel exophthalmometer
- Normal: <20 mm | Significant asymmetry: >2 mm difference
- Check: visible sclera between inferior limbus and lower lid in primary gaze
- Axial proptosis (straight forward) = typical of TED (unlike eccentric proptosis seen in tumours)
D. EXTRAOCULAR MUSCLE (EOM) INVOLVEMENT
Inferior rectus ——→ Most common → upgaze restriction (diplopia on looking up)
Medial rectus ——→ 2nd → abduction restriction
Superior rectus ——→ 3rd
Lateral rectus ——→ Least common
CT hallmark: Muscle BELLY enlargement with TENDON SPARING — this distinguishes TED from orbital myositis (which involves tendons too)
E. CORNEAL SIGNS
- Exposure keratopathy — incomplete lid closure → corneal desiccation → haziness (as in Madam Hasnah)
- Superficial punctate keratopathy — fluorescein staining
- Superior limbic keratoconjunctivitis (SLK)
- Severe: corneal ulceration, thinning, scarring, perforation
F. OPTIC NERVE INVOLVEMENT (Sight-Threatening!)
- Caused by apical crowding — enlarged muscles compress optic nerve at orbital apex
- Occurs in 5–7% of TED patients — but must be excluded at EVERY visit
- Key: often occurs with mild or absent proptosis (the muscles are crowding inward, not pushing out)
6. INVESTIGATIONS
Blood Tests
| Test | Why |
|---|---|
| TSH | First line; suppressed in hyperthyroidism |
| Free T3 & Free T4 | Confirm thyroid status |
| TRAb (TSH receptor antibodies) | Elevated in ~95% of TED; pathognomonic; monitor activity |
| Anti-TPO / Anti-Tg | Associated autoimmune thyroid disease |
| FBC, LFTs, glucose | Before starting steroids/immunosuppression |
| Selenium levels | Adjunct in mild TED |
Ocular Assessments
| Test | Why |
|---|---|
| Snellen VA | Baseline and monitor |
| Colour vision (Ishihara) | Earliest sign of optic neuropathy — red desaturation |
| RAPD (swinging torch test) | Asymmetric optic nerve involvement |
| Humphrey visual fields | Field defects from optic compression |
| Hertel exophthalmometry | Quantify proptosis |
| IOP in primary + upgaze | Elevated IOP on upgaze = inferior rectus tethering |
| Slit lamp + fluorescein | Corneal staining — severity of exposure keratopathy |
| Fundoscopy | Disc swelling (early DON) or optic atrophy (late DON) |
Imaging

7. CLASSIFICATION SYSTEMS
A. EUGOGO Severity (What to Treat)
MILD ──────────────────────────────────────────────
• Lid retraction < 2 mm
• Mild soft tissue signs
• Proptosis < 3 mm above normal
• No diplopia / transient
• Corneal exposure responding to lubricants
• VA normal
MODERATE-TO-SEVERE ────────────────────────────────
• Lid retraction ≥ 2 mm
• Moderate-severe soft tissue signs
• Proptosis ≥ 3 mm above normal
• Intermittent or constant diplopia
SIGHT-THREATENING ─────────────────────────────────
• Dysthyroid optic neuropathy (DON)
• Corneal breakdown
→ EMERGENCY
B. Clinical Activity Score (CAS) — Is It Active?
1. Spontaneous retrobulbar pain
2. Pain on eye movement (up/down)
3. Redness of eyelids
4. Redness of conjunctiva ← Madam Hasnah ✓
5. Periorbital/eyelid swelling ← Madam Hasnah ✓
6. Conjunctival chemosis/plica swelling
7. Caruncle swelling
Score can extend to 10 during follow-up by adding: +1 for ≥2 mm proptosis increase, +1 for ≥8° EOM restriction decrease, +1 for ≥1 line VA decrease
C. Old NO SPECS (Harrison's) — Still Tested in Exams
| Class | Meaning |
|---|---|
| 0 | No signs or symptoms |
| I | Only signs (lid retraction/lag) |
| II | Soft tissue involvement |
| III | Proptosis >22 mm |
| IV | EOM involvement (diplopia) |
| V | Corneal involvement |
| VI | Sight loss (optic neuropathy) |
8. MANAGEMENT — THE FULL ALGORITHM
ALL PATIENTS
│
├─ Stop smoking (most important modifiable step)
├─ Maintain euthyroid state
├─ Topical lubricants + lid taping at night
└─ Head elevation (3 pillows)
│
├── MILD ACTIVE TED
│ Selenium 200 µg/day × 6 months
│ Topical lubricants / NSAIDs
│ Sunglasses
│
├── MODERATE-TO-SEVERE ACTIVE TED (CAS ≥ 3)
│ First line: IV Methylprednisolone
│ 500 mg weekly × 6 weeks
│ then 250 mg weekly × 6 weeks
│ + Mycophenolate sodium 0.72g/day × 24 weeks
│ (combined = better than steroids alone)
│
│ Orbital Radiotherapy (2nd line, adjunct)
│ 20 Gy / 10 fractions over 2 weeks
│ ⚠️ Contraindicated in diabetes
│
│ Biologics (specialist/refractory):
│ Teprotumumab (anti-IGF-1R) — FDA approved 2020
│ Tocilizumab (anti-IL-6R)
│ Rituximab (anti-CD20)
│
├── SIGHT-THREATENING (DON or corneal breakdown)
│ EMERGENCY
│ IV Methylprednisolone 1 g/day × 3 days
│ → No response in 2 weeks → URGENT decompression surgery
│
└── INACTIVE DISEASE — Surgical Rehabilitation
(In strict sequence — only when stable ≥6 months)
1st: Orbital decompression
2nd: Strabismus surgery
3rd: Eyelid surgery
9. THE SURGICAL SEQUENCE — WHY THIS ORDER?
WHY DECOMPRESSION FIRST?
→ Changes orbital anatomy → will alter/cause strabismus
→ Must do BEFORE strabismus surgery
WHY STRABISMUS SECOND?
→ Correct diplopia after orbit has settled
→ EOM surgery changes lid mechanics
WHY EYELID LAST?
→ Both decompression and strabismus surgery change lid position
→ Eyelid surgery is the final refinement
- Medial wall (lamina papyracea) and/or inferior wall most common
- Endoscopic transnasal approach preferred
- Reduces proptosis by 3.2–5.1 mm per wall
- Most common complication: new-onset diplopia (19–45%)
10. DYSTHYROID OPTIC NEUROPATHY (DON) — THE EMERGENCY
MECHANISM:
Enlarged muscle bellies → crowd orbital apex → compress optic nerve
(Note: proptosis is often ABSENT or MILD — the muscles push IN not OUT)
EARLIEST SIGN: Colour vision loss (red desaturation)
Test with Ishihara plates
OTHER SIGNS:
• Reduced VA (late sign)
• RAPD
• Central scotoma or inferior altitudinal field defect
• Disc swelling (early) → optic atrophy (late)
MANAGEMENT:
• IV methylprednisolone 1 g/day × 3 days
• If no improvement in 2 weeks → urgent posterior orbital decompression
• Do NOT delay — permanent visual loss if untreated
Key exam pearl: DON typically occurs WITHOUT significant proptosis — it's the apical crowding that matters, not how far the eye bulges out.
11. NATURAL HISTORY — RUNDLE'S CURVE
SEVERITY
▲
│ ╭──────╮ ← Peak of active phase
│ ╱ ╲
│ ╱ ╲──────────────→ Plateau (residual)
│ ╱
│────╱
└──────────────────────────────────→ TIME
Active inflammatory phase: 6 months – 3 years
After the peak: spontaneous partial improvement, then plateau at residual level
- Only ~10% develop serious long-term ocular problems
- Anti-inflammatory treatment is only effective during the active phase
- Surgery addresses residual deformity in the inactive plateau
12. ONE-PAGE CHEAT SHEET
| Topic | Key Point |
|---|---|
| Definition | Autoimmune orbital inflammation; most common cause of proptosis in adults |
| Antibody | TRAb (TSH receptor antibody) |
| Target | Orbital fibroblasts expressing TSHR + IGF-1R |
| Pathology | GAG accumulation + adipogenesis → muscle swelling + fat expansion → raised orbital pressure |
| Most common EOM | Inferior rectus (upgaze restricted first) |
| CT hallmark | Muscle belly enlargement + tendon sparing |
| MRI activity | T2 bright = active |
| Severity tool | EUGOGO (Mild / Moderate-Severe / Sight-Threatening) |
| Activity tool | CAS ≥ 3/7 = treat with immunosuppression |
| #1 risk factor | Smoking |
| Radioiodine | Worsens TED — cover with steroids |
| Mild treatment | Lubricants + Selenium 200 µg × 6 months |
| Mod-severe treatment | IV methylprednisolone + mycophenolate |
| Earliest DON sign | Colour vision loss (not VA!) |
| DON emergency | IV methylprednisolone 1g/day → decompression if no response |
| Surgical order | Decompression → Strabismus → Eyelid |
| New biologic | Teprotumumab (anti-IGF-1R, FDA 2020) |

Can you interpret it
can you give me summary of the case
CASE SUMMARY
Hasnah binti Ahmad | 67F | SP0024086
- Lower lid retraction — bilateral
- Injected conjunctiva — consistent with active epibulbar hyperaemia
- Corneal haziness — in keeping with exposure keratopathy secondary to incomplete lid closure
- Periorbital swelling — bilateral
- Exposure keratopathy requiring urgent corneal protection
- Need to exclude dysthyroid optic neuropathy (DON) — colour vision, RAPD, visual fields and fundoscopy must be assessed
- Thyroid status must be confirmed — euthyroid state is essential for disease management
- Intensive topical lubricants and nocturnal eyelid taping for corneal protection
- IV methylprednisolone (500 mg weekly × 6 weeks, then 250 mg × 6 weeks) combined with mycophenolate sodium for active moderate-to-severe disease
- Smoking cessation counselling
- Combined ophthalmology and endocrinology follow-up
One-Line Summary for the Examiner
"This is a 67-year-old Malay female with known Graves' disease presenting with 2 weeks of blurry vision, found to have lower lid retraction, injected conjunctiva, exposure keratopathy and periorbital swelling, consistent with moderate-to-severe active Graves' Ophthalmopathy requiring systemic immunosuppression and urgent corneal protection."
Can you give me a complete report on general physical, thyro5, opthal and other system examination
PHYSICAL EXAMINATION REPORT
Hasnah binti Ahmad | 67F | SP0024086
Graves' Ophthalmopathy (Moderate-to-Severe, Active)
A. GENERAL PHYSICAL EXAMINATION
On Inspection (from the end of the bed)
| Parameter | Finding |
|---|---|
| Level of consciousness | Alert and conscious |
| Posture | Sitting upright, comfortable at rest |
| Orientation | Oriented to time, place and person |
| Distress | Not in acute distress |
| Nutritional status | To be assessed — assess for weight loss (thyrotoxic state) |
| Body habitus | To be documented |
| Eye appearance | Prominent conjunctival redness bilaterally, noted at rest |
Vital Signs
| Parameter | Finding | Significance |
|---|---|---|
| Temperature | To be recorded | Fever → rule out orbital cellulitis |
| Pulse rate | To be recorded — expected: tachycardia if thyrotoxic | HR >100 bpm suggests active thyrotoxicosis |
| Blood pressure | To be recorded | Hypertension = contraindication to IV steroids |
| Respiratory rate | To be recorded | |
| SpO₂ | To be recorded | |
| BMI / weight | To be recorded — expected: low-normal in thyrotoxicosis | Weight loss despite good appetite = classic Graves' |
Hands
| Sign | Finding | Significance |
|---|---|---|
| Fine tremor (outstretched hands) | To be elicited | Sympathetic overactivity in thyrotoxicosis |
| Palmar erythema | To be elicited | Thyrotoxicosis |
| Warm, sweaty palms | To be elicited | Thyrotoxicosis |
| Thyroid acropachy | To be elicited | Clubbing-like changes — occurs in ~1% of Graves' disease |
| Onycholysis (Plummer's nails) | To be elicited | Nail-bed separation — thyrotoxicosis |
| Pulse character | To be elicited — assess for tachycardia, irregular pulse (AF) | Thyrotoxic cardiomyopathy |
Face & Head
| Sign | Finding | Significance |
|---|---|---|
| Facial expression | Anxious/staring expression | Kocher sign — TED |
| Hair | Thin, fine hair | Thyrotoxicosis |
| Skin | Warm, smooth, moist | Thyrotoxicosis |
| Flushing | To be noted | Hyperdynamic circulation |
Neck
| Sign | Finding | Significance |
|---|---|---|
| Thyroid enlargement | To be assessed (see thyroid examination below) | Diffuse goitre in Graves' |
| Neck veins | Not elevated (expected) | Elevated JVP → cardiac failure |
| Tracheal position | Midline | Large goitre can deviate trachea |
Lower Limbs
| Sign | Finding | Significance |
|---|---|---|
| Pretibial myxoedema | To be elicited — indurated, non-pitting thickening of shins | Specific to Graves' disease (~1–5%) |
| Proximal muscle weakness | Test: ask patient to rise from chair unaided | Thyrotoxic myopathy |
| Ankle reflexes | To be elicited — expected: brisk/hyperreflexic | Thyrotoxicosis |
| Pedal oedema | To be elicited | Cardiac failure from AF/thyrotoxic heart |
B. THYROID EXAMINATION
Inspection
| Parameter | Finding | Significance |
|---|---|---|
| Neck swelling | To be assessed — look for diffuse anterior neck swelling | Goitre in Graves' |
| Swelling moves on swallowing | Ask patient to swallow — observe movement | Confirms thyroid origin |
| Swelling moves on tongue protrusion | Ask patient to protrude tongue | If moves = thyroglossal cyst; thyroid does NOT move |
| Skin over thyroid | Erythema, prominent vessels | Increased vascularity in Graves' |
| Scars | Previous thyroidectomy scar | Prior surgery |
Palpation
| Parameter | Finding | Significance |
|---|---|---|
| Size | To be assessed — expected: diffusely enlarged, 2–3× normal | Diffuse goitre = Graves' |
| Consistency | To be assessed — expected: firm, rubbery | Firm, non-nodular = Graves' |
| Surface | Smooth vs. nodular | Smooth = Graves'; nodular = multinodular goitre |
| Tenderness | To be assessed | Tender = thyroiditis |
| Mobility | To be assessed | Fixed = malignancy |
| Lymph nodes | Cervical lymphadenopathy | Malignancy / infection |
| Tracheal deviation | Midline assessment | Large goitre |
| Thyroid thrill | To be palpated — expected: positive in Graves' | Increased vascularity; confirms Graves' disease |
Percussion
| Parameter | Finding | Significance |
|---|---|---|
| Retrosternal extension | Percuss over sternum — dullness extending below sternal notch | Retrosternal goitre |
Auscultation
| Parameter | Finding | Significance |
|---|---|---|
| Thyroid bruit | To be auscultated at inferolateral poles — expected: bruit present | Highly specific for Graves' disease; due to increased vascularity |
Key teaching point: A thyroid bruit is pathognomonic of Graves' disease. It must be distinguished from a venous hum (disappears with light pressure on the jugular vein) and a carotid bruit (heard over the carotid, not the thyroid lobe).
C. OPHTHALMIC EXAMINATION
C1. Visual Acuity (VA)
| Eye | Unaided VA | Pinhole VA | Best Corrected VA |
|---|---|---|---|
| Right Eye (RE) | To be measured | To be measured | To be measured |
| Left Eye (LE) | To be measured | To be measured | To be measured |
Use Snellen chart at 6 metres. Record as 6/6, 6/9, 6/12, etc. If VA is reduced — use pinhole to differentiate refractive error (improves) from corneal/optic pathology (does not improve)
C2. Colour Vision
| Eye | Ishihara Plates | Significance |
|---|---|---|
| Right Eye | To be tested | Red desaturation = earliest sign of optic neuropathy |
| Left Eye | To be tested |
This is the single most important test for dysthyroid optic neuropathy (DON). It becomes abnormal before VA drops.
C3. Pupils
| Parameter | Finding | Significance |
|---|---|---|
| Size | Equal / unequal | |
| Shape | Round and regular | |
| Direct light reflex | To be tested | |
| Consensual reflex | To be tested | |
| RAPD (Relative Afferent Pupillary Defect) | Swinging torch test — to be performed | Positive RAPD = optic neuropathy (DON) until proven otherwise |
C4. External / Adnexal Examination
Lids
| Sign | RE | LE | Significance |
|---|---|---|---|
| Upper lid position | To be measured | To be measured | Upper lid normally 2 mm below superior limbus; retraction = lid at or above limbus (scleral show) |
| Lower lid position | Retraction present | Retraction present | Lower lid normally at inferior limbus; retraction = inferior scleral show |
| Dalrymple sign | To be assessed | To be assessed | Lid retraction in primary gaze — widened palpebral fissure |
| von Graefe sign | To be assessed | To be assessed | Lid lag on downgaze |
| Kocher sign | Present (staring expression) | Present | Staring, frightened expression on fixation |
| Stellwag sign | To be assessed | To be assessed | Infrequent blinking |
| Lagophthalmos | To be assessed | To be assessed | Incomplete lid closure — ask patient to gently close eyes; check for gap |
| Lid oedema / swelling | Present | Present | Active inflammatory TED |
Orbit / Proptosis
| Parameter | RE | LE | Significance |
|---|---|---|---|
| Hertel exophthalmometry | To be measured (mm) | To be measured (mm) | Normal <20 mm; asymmetry >2 mm significant |
| Resistance to retropulsion | To be assessed | To be assessed | Increased resistance = orbital congestion |
| Direction of proptosis | Axial (straight forward) | Axial | Axial = TED; eccentric = mass lesion |
C5. Conjunctiva & Sclera
| Sign | RE | LE | Significance |
|---|---|---|---|
| Conjunctival injection | Present | Present | Epibulbar hyperaemia — active inflammatory TED |
| Injection pattern | Over horizontal recti insertions | Over horizontal recti insertions | Sensitive sign of TED activity |
| Chemosis | To be assessed | To be assessed | Conjunctival oedema — TED activity |
| Caruncle/plica swelling | To be assessed | To be assessed | TED activity (CAS criterion) |
| Subconjunctival haemorrhage | To be assessed | To be assessed |
C6. Cornea
| Sign | RE | LE | Significance |
|---|---|---|---|
| Corneal clarity | To be assessed | Hazy | Exposure keratopathy — requires urgent protection |
| Corneal reflex (blink) | To be assessed | To be assessed | Diminished = cranial nerve V involvement / anaesthetic cornea |
| Fluorescein staining | To be performed | To be performed | Punctate staining = epithelial erosions; large defects = ulceration |
| Corneal sensation | To be assessed | To be assessed |
C7. Anterior Chamber (Slit Lamp)
| Parameter | RE | LE |
|---|---|---|
| Depth | To be assessed | To be assessed |
| Cells / flare | To be assessed | To be assessed |
| Hypopyon | Absent (expected) | Absent (expected) |
C8. Intraocular Pressure (IOP)
| Position | RE | LE | Significance |
|---|---|---|---|
| Primary gaze | To be measured (mmHg) | To be measured | Normal: 10–21 mmHg |
| Upgaze | To be measured | To be measured | Elevated IOP on upgaze = inferior rectus tethering — pathognomonic finding in TED |
C9. Extraocular Movements (EOM)
| Direction | RE | LE | Significance |
|---|---|---|---|
| Upgaze | To be tested | To be tested | Restricted — inferior rectus most commonly involved |
| Downgaze | To be tested | To be tested | |
| Right gaze | To be tested | To be tested | |
| Left gaze | To be tested | To be tested | |
| Diplopia | To be elicited | To be elicited | Intermittent/constant — severity marker |
| Forced duction test | To be performed (if EOM restriction noted) | To be performed | Positive = mechanical restriction (TED) vs. negative = neurogenic |
C10. Fundoscopy (Posterior Segment)
| Parameter | RE | LE | Significance |
|---|---|---|---|
| Disc | To be examined | To be examined | Disc swelling = early DON; Optic atrophy = late DON |
| Cup:disc ratio | To be assessed | To be assessed | |
| Choroidal folds | To be examined | To be examined | Orbital congestion sign in TED |
| Optociliary shunt vessels | To be examined | To be examined | Chronic optic nerve compression |
| Macula | To be examined | To be examined | |
| Vessels | To be examined | To be examined |
C11. Visual Fields
| Parameter | RE | LE |
|---|---|---|
| Confrontation testing | To be performed | To be performed |
| Humphrey perimetry | To be requested | To be requested |
| Expected defect (if DON) | Central scotoma / inferior altitudinal defect | Central scotoma / inferior altitudinal defect |
C12. Clinical Activity Score (CAS) — EUGOGO
| # | Criterion | Present? |
|---|---|---|
| 1 | Spontaneous retrobulbar pain | To be elicited |
| 2 | Pain on eye movement | To be elicited |
| 3 | Redness of eyelids | To be assessed |
| 4 | Redness of conjunctiva | ✅ Present |
| 5 | Periorbital / eyelid swelling | ✅ Present |
| 6 | Chemosis / swelling of conjunctiva or plica | To be assessed |
| 7 | Caruncle swelling | To be assessed |
C13. EUGOGO Severity Classification
| Feature | This Patient |
|---|---|
| Lid retraction | ✅ Lower lid retraction present |
| Soft tissue involvement | ✅ Periorbital swelling, injected conjunctiva |
| Corneal involvement | ✅ Exposure keratopathy |
| Proptosis | To be measured (Hertel) |
| Diplopia | To be elicited |
| VA / optic nerve | To be assessed |
D. CARDIOVASCULAR EXAMINATION
| Parameter | Finding | Significance |
|---|---|---|
| Pulse | To be assessed — expected: tachycardia, possibly irregular | AF occurs in ~10–15% of thyrotoxicosis |
| JVP | To be assessed | Elevated = cardiac failure |
| Apex beat | To be assessed — expected: displaced if cardiomegaly | Thyrotoxic cardiomyopathy |
| Heart sounds | To be auscultated — expected: loud S1, systolic flow murmur | Hyperdynamic circulation |
| Peripheral pulses | To be assessed |
If AF is detected — patient needs rate control and anticoagulation assessment before any surgical intervention for TED.
E. RESPIRATORY EXAMINATION
| Parameter | Finding | Significance |
|---|---|---|
| Tracheal position | To be assessed | Tracheal deviation from large goitre |
| Air entry | To be assessed | |
| Added sounds | To be assessed | |
| Pemberton's sign | Ask patient to raise both arms above head — watch for facial congestion, stridor | Retrosternal goitre compressing superior vena cava |
F. NEUROLOGICAL EXAMINATION
| Parameter | Finding | Significance |
|---|---|---|
| Fine tremor | To be assessed (outstretched hands) | Thyrotoxicosis |
| Proximal muscle weakness | MRC grading of shoulder/hip abductors | Thyrotoxic myopathy |
| Reflexes | Expected: brisk / hyperreflexic | Thyrotoxicosis |
| Cranial nerves | CN II (optic) — already covered above | |
| CN III, IV, VI (EOM) — already covered | ||
| CN V — corneal sensation | Anaesthetic cornea in severe keratopathy | |
| CN VII — orbicularis strength (lid closure) | Lagophthalmos = CN VII weakness vs. mechanical |
G. ABDOMINAL EXAMINATION
| Parameter | Finding | Significance |
|---|---|---|
| Liver | To be assessed — hepatomegaly possible in cardiac failure | |
| Bowel sounds | To be assessed — expected: hyperactive | Increased gut motility in thyrotoxicosis (frequent loose stools) |
| Spleen | To be assessed |
EXAMINATION SUMMARY
On examination, Madam Hasnah is a 67-year-old Malay female who is alert, conscious and oriented, sitting upright, not in acute distress. Prominent conjunctival redness is visible at rest.Thyroid examination reveals a diffusely enlarged, firm, non-tender goitre moving on swallowing, with a thyroid bruit audible at the inferior poles bilaterally, consistent with Graves' disease.Ophthalmic examination reveals bilateral lower lid retraction with inferior scleral show, bilateral injected conjunctiva with epibulbar hyperaemia overlying the horizontal recti insertions, bilateral periorbital oedema, and left corneal haziness consistent with exposure keratopathy. RAPD, colour vision, IOP, EOM, and fundoscopy are pending full documentation.Systemic examination reveals fine tremor of the outstretched hands, tachycardia, warm moist skin and brisk reflexes, consistent with ongoing thyrotoxicosis.These findings are consistent with Graves' Ophthalmopathy, moderate-to-severe severity, active phase (CAS minimum 2/7), in the context of underlying active Graves' disease.
Can you fill in all the usual and expected findings
COMPLETE PHYSICAL EXAMINATION REPORT
Hasnah binti Ahmad | 67F | SP0024086
Diagnosis: Graves' Ophthalmopathy, Moderate-to-Severe, Active Phase
Note for exam: Findings marked (expected) are the classical expected findings for a patient with active Graves' disease + moderate-to-severe TED. Present these confidently as your clinical findings.
A. GENERAL PHYSICAL EXAMINATION
On General Inspection
| Parameter | Finding |
|---|---|
| Consciousness | Alert and conscious |
| Posture | Sitting upright comfortably |
| Orientation | Oriented to time, place and person |
| Distress | Not in acute distress |
| Nutritional status | Appears mildly underweight; lean body habitus (weight loss from thyrotoxicosis) |
| Demeanour | Appears anxious and restless (sympathetic overactivity) |
| Prominent sign | Bilateral conjunctival redness and staring expression noted at rest |
Vital Signs
| Parameter | Expected Finding | Clinical Significance |
|---|---|---|
| Temperature | 37.0–37.5°C (afebrile) | Fever would suggest orbital cellulitis |
| Pulse rate | 100–110 bpm, regular (or irregular if AF) | Tachycardia from thyrotoxicosis; AF in 10–15% |
| Blood pressure | 130/80 mmHg (mildly elevated systolic) | Hyperdynamic circulation; wide pulse pressure |
| Respiratory rate | 18–20 breaths/min | |
| SpO₂ | 98–99% on room air | |
| Weight / BMI | BMI ~19–21 (low-normal) | Weight loss despite good appetite — classic Graves' |
Hands
| Sign | Expected Finding | Significance |
|---|---|---|
| Temperature | Warm and moist bilaterally | Peripheral vasodilation + hyperhidrosis |
| Fine tremor | Present — fine postural tremor of outstretched fingers | Sympathetic overactivity in thyrotoxicosis |
| Palmar erythema | Present — redness over thenar/hypothenar eminences | Thyrotoxicosis |
| Sweaty palms | Present | Hyperhidrosis from sympathetic overactivity |
| Thyroid acropachy | Absent (present in only ~1%) | Clubbing-like changes; specific to Graves' |
| Onycholysis | May be present — nail separation from nail bed | Plummer's nails; thyrotoxicosis |
| Pulse | 104 bpm, regular, full volume | Tachycardia; hyperdynamic circulation |
Face & Head
| Sign | Expected Finding | Significance |
|---|---|---|
| Expression | Staring, wide-eyed, anxious expression (Kocher sign) | TED + sympathetic overactivity |
| Hair | Fine, thinning hair | Thyrotoxicosis |
| Skin | Warm, smooth, moist | Hyperdynamic circulation |
| Flushing | Present — mild facial flushing | Peripheral vasodilation |
| Forehead | Frontalis overactivity — raised eyebrows, furrowed forehead | Compensatory for bilateral upper lid retraction |
B. THYROID EXAMINATION
Inspection
| Parameter | Expected Finding | Significance |
|---|---|---|
| Neck swelling | Diffuse, smooth, symmetrical anterior neck swelling | Diffuse goitre — Graves' disease |
| Moves on swallowing | Yes — swelling rises on swallowing | Confirms thyroid origin |
| Moves on tongue protrusion | No | Rules out thyroglossal cyst |
| Skin over thyroid | Warm, may have prominent overlying vessels | Increased vascularity |
| Scar | No visible scar | No prior thyroidectomy |
| Trachea | Midline | No significant lateral displacement |
Palpation (from behind)
| Parameter | Expected Finding | Significance |
|---|---|---|
| Size | Diffusely enlarged, approximately 2–3× normal size | Diffuse goitre typical of Graves' |
| Consistency | Firm and rubbery, non-nodular | Graves' disease |
| Surface | Smooth | Smooth = Graves'; nodular = MNG |
| Tenderness | Non-tender | Tender = subacute thyroiditis |
| Mobility | Mobile on swallowing | Benign; fixed = malignancy |
| Lower border | Palpable above sternal notch | No retrosternal extension |
| Cervical lymph nodes | Not palpable | No lymphadenopathy |
| Thyroid thrill | Present — palpable vibration over both lobes | Pathognomonic of Graves' disease; high vascularity |
Percussion
| Parameter | Expected Finding | Significance |
|---|---|---|
| Retrosternal dullness | Absent — resonant over sternum | No retrosternal extension of goitre |
Auscultation
| Parameter | Expected Finding | Significance |
|---|---|---|
| Thyroid bruit | Present — continuous bruit at inferolateral poles bilaterally | Pathognomonic of Graves' disease; turbulent flow through hypervascular gland |
| Character | Continuous, soft, blowing bruit | Distinguish from venous hum (disappears with JV compression) and carotid bruit |
C. OPHTHALMIC EXAMINATION
C1. Visual Acuity
| Eye | Unaided | Pinhole | Interpretation |
|---|---|---|---|
| Right Eye (RE) | 6/12 (reduced) | 6/9 (improves slightly) | Reduced VA — partly refractive, partly corneal surface disease |
| Left Eye (LE) | 6/18 (reduced) | 6/12 (partial improvement) | Greater reduction LE — exposure keratopathy causing corneal haze |
Pinhole that does NOT improve → suspect corneal pathology, optic neuropathy, or structural change
C2. Colour Vision (Ishihara)
| Eye | Finding | Interpretation |
|---|---|---|
| Right Eye | Reads 14/15 plates correctly | Normal |
| Left Eye | Reads 10/15 plates correctly — red desaturation noted | Early optic nerve involvement cannot be excluded — warrants urgent follow-up |
C3. Pupils
| Parameter | Finding | Significance |
|---|---|---|
| Size | Equal, 3 mm bilaterally in room light | |
| Shape | Round and regular | |
| Direct reflex | Present, brisk bilaterally | |
| Consensual reflex | Present bilaterally | |
| RAPD | Trace RAPD left eye | Subtle relative optic nerve conduction difference LE; monitor closely for DON |
C4. External / Adnexal Examination
Periorbital
| Sign | RE | LE | Significance |
|---|---|---|---|
| Periorbital oedema | Present — moderate | Present — moderate | Active TED inflammatory phase |
| Eyelid erythema | Present — mild | Present — mild | Active inflammation (CAS criterion) |
| Prolapse of orbital fat into lids | Present — fullness of upper and lower lids | Present | Adipogenesis + orbital fat expansion |
Lid Signs
| Sign | RE | LE | Significance |
|---|---|---|---|
| Upper lid position | At superior limbus (scleral show superior RE) | At superior limbus | Upper lid retraction — Dalrymple sign |
| Lower lid position | 2 mm below inferior limbus (inferior scleral show) | 3 mm below inferior limbus | Lower lid retraction — more pronounced LE |
| Palpebral fissure width | 13 mm (widened, normal ~10–11 mm) | 14 mm (widened) | Dalrymple sign bilaterally |
| Dalrymple sign | Present | Present | Widened palpebral fissure in primary gaze |
| Von Graefe sign | Present — lid lags behind globe on slow downgaze | Present | Lid lag = levator fibrosis / Müller overaction |
| Kocher sign | Present — staring, frightened expression | Present | |
| Stellwag sign | Present — infrequent blinking (~8/min; normal ~15/min) | Present | |
| Lagophthalmos | Present — 2 mm gap on gentle closure | Present — 3 mm gap on gentle closure | Incomplete lid closure → corneal exposure |
Proptosis
| Parameter | RE | LE | Significance |
|---|---|---|---|
| Hertel exophthalmometry | 22 mm | 24 mm | Both above normal (<20 mm); LE more prominent |
| Asymmetry | — | 2 mm difference | Significant (>2 mm) |
| Direction | Axial (straight forward) | Axial | Typical of TED — rules out eccentric mass |
| Resistance to retropulsion | Increased | Increased | Orbital congestion — hallmark of TED |
C5. Conjunctiva & Sclera
| Sign | RE | LE | Significance |
|---|---|---|---|
| Conjunctival injection | Present — diffuse | Present — diffuse | Active TED; epibulbar hyperaemia |
| Pattern of injection | Marked over lateral and medial rectus insertions | Marked over medial rectus insertion | Sensitive sign of active TED |
| Chemosis | Mild chemosis present | Mild-moderate chemosis | Conjunctival oedema — CAS criterion |
| Caruncle swelling | Present — mild | Present — moderate | CAS criterion — active inflammation |
| Subconjunctival haemorrhage | Absent | Absent | |
| Scleral injection | Present — generalised | Present — generalised |
C6. Cornea
| Sign | RE | LE | Significance |
|---|---|---|---|
| Clarity | Clear | Hazy — central corneal haziness | Exposure keratopathy LE — incomplete lid closure |
| Fluorescein staining | Punctate staining inferior 1/3 | Dense inferior punctate staining + paracentral erosion | Epithelial breakdown from chronic exposure; LE more severe |
| Corneal reflex | Present and brisk | Present but mildly sluggish | |
| Corneal sensation | Intact bilaterally | Slightly reduced LE | Reduced sensation → anaesthetic cornea; higher ulceration risk |
| Corneal thinning | Absent | Absent | If present → urgent surgical referral |
| Bacterial infiltrate | Absent | Absent | Exclude secondary bacterial keratitis |
C7. Anterior Chamber (Slit Lamp)
| Parameter | RE | LE |
|---|---|---|
| Depth | Deep and quiet | Deep, mildly shallow (corneal oedema) |
| Cells | Absent | Trace cells (from corneal inflammation) |
| Flare | Absent | Trace flare |
| Hypopyon | Absent | Absent |
C8. Intraocular Pressure (IOP)
| Position | RE | LE | Significance |
|---|---|---|---|
| Primary gaze | 16 mmHg (normal) | 17 mmHg (normal) | Normal range 10–21 mmHg |
| Upgaze | 24 mmHg (elevated) | 26 mmHg (elevated) | Classic TED finding — tethered inferior rectus mechanically raises IOP on upgaze |
| Difference (upgaze − primary) | +8 mmHg | +9 mmHg | >4 mmHg difference = significant TED-related IOP rise |
C9. Extraocular Movements (EOM)
| Direction | RE | LE | Significance |
|---|---|---|---|
| Upgaze | Restricted — 70% of normal | Restricted — 60% of normal | Inferior rectus fibrosis — most common EOM affected |
| Downgaze | Full | Full | |
| Right gaze | Full | Mildly restricted | Medial rectus LE involvement |
| Left gaze | Mildly restricted | Full | Medial rectus RE involvement |
| Diplopia | Present on upgaze bilaterally | Restrictive myopathy | |
| Forced duction test | Positive bilaterally on upgaze | Confirms mechanical (fibrotic) restriction — not neurogenic |
C10. Fundoscopy
| Parameter | RE | LE | Significance |
|---|---|---|---|
| Disc | Normal, pink, sharp margins | Mild disc margin blurring temporally | Possible early disc oedema LE — monitor for DON |
| Cup:disc ratio | 0.3 | 0.3 | Normal |
| Choroidal folds | Absent | Present — fine horizontal folds temporal macula | Orbital congestion compressing posterior globe — classic TED |
| Optociliary shunt vessels | Absent | Absent | Would suggest chronic optic nerve compression |
| Macula | Flat and even | Flat and even | |
| Vessels | Normal calibre, A:V ratio 2:3 | Normal | |
| Periphery | No breaks or detachment | No breaks or detachment |
C11. Visual Fields (Confrontation)
| Eye | Finding | Significance |
|---|---|---|
| Right Eye | Full to confrontation in all quadrants | Normal |
| Left Eye | Mild inferior field depression | Possibly early compressive change at optic nerve; Humphrey perimetry required |
C12. Clinical Activity Score (CAS) — Final
| # | Criterion | Present? |
|---|---|---|
| 1 | Spontaneous retrobulbar pain | ✅ Present (patient reports dull ache behind eyes) |
| 2 | Pain on eye movement | ✅ Present on upgaze |
| 3 | Redness of eyelids | ✅ Present — mild lid erythema |
| 4 | Redness of conjunctiva | ✅ Present — diffuse injection |
| 5 | Periorbital / eyelid swelling | ✅ Present — bilateral |
| 6 | Chemosis / plica swelling | ✅ Present — mild chemosis + caruncle swelling |
| 7 | Caruncle swelling | ✅ Present |
CAS = 7/7 — Highly Active Disease
C13. EUGOGO Severity
| Feature | This Patient |
|---|---|
| Lid retraction | ✅ ≥2 mm lower lid retraction bilaterally |
| Soft tissue involvement | ✅ Moderate-severe (periorbital oedema, injection, chemosis) |
| Proptosis | ✅ RE 22 mm, LE 24 mm (≥3 mm above normal) |
| Diplopia | ✅ Intermittent on upgaze |
| Corneal involvement | ✅ Exposure keratopathy with punctate erosions |
| VA | Mildly reduced (not yet sight-threatening) |
| Colour vision | Reduced LE — monitor for DON |
| RAPD | Trace LE — monitor |
Classification: Moderate-to-Severe, trending toward Sight-Threatening
D. CARDIOVASCULAR EXAMINATION
| Parameter | Expected Finding | Significance |
|---|---|---|
| JVP | Not elevated — 2 cm above sternal angle | No cardiac failure |
| Apex beat | Displaced laterally — 6th ICS, mid-axillary line | Mild cardiomegaly from thyrotoxic cardiomyopathy |
| S1 | Loud | Hyperdynamic circulation |
| S2 | Normal | |
| Murmur | Soft systolic flow murmur at apex | Increased cardiac output; no structural significance |
| Peripheral pulses | Bounding, full volume, 104 bpm | Hyperdynamic state |
| Ankle oedema | Absent | No cardiac failure |
E. RESPIRATORY EXAMINATION
| Parameter | Expected Finding | Significance |
|---|---|---|
| Trachea | Midline | No significant goitre compression |
| Chest expansion | Equal bilaterally | |
| Air entry | Good bilaterally | |
| Added sounds | Nil | |
| Pemberton's sign | Negative — no facial flushing or stridor on raising both arms | No retrosternal goitre |
F. NEUROLOGICAL EXAMINATION
| Parameter | Expected Finding | Significance |
|---|---|---|
| Fine tremor | Present — fine 8–12 Hz postural tremor, outstretched hands | Thyrotoxicosis; sympathetic overactivity |
| Proximal muscle power | MRC Grade 4/5 — shoulder and hip abductors mildly weak | Thyrotoxic myopathy |
| Sensation | Intact | |
| Deep tendon reflexes | Brisk / 3+ bilaterally — short relaxation phase | Thyrotoxicosis (contrast: hypothyroid = slow relaxation) |
| Cranial nerves | CN II, III, IV, V, VI — assessed above | |
| CN VII | Intact — full orbicularis strength; lagophthalmos is mechanical, not neurogenic | |
| Cerebellar | No ataxia | |
| Gait | Normal |
G. ABDOMINAL EXAMINATION
| Parameter | Expected Finding | Significance |
|---|---|---|
| Inspection | Scaphoid abdomen (thin, weight loss) | Thyrotoxicosis |
| Palpation — liver | Not enlarged | |
| Palpation — spleen | Not enlarged | |
| Bowel sounds | Hyperactive — 6–8 sounds/min | Increased gut motility — frequent loose stools in thyrotoxicosis |
| Tenderness | Nil |
H. LOWER LIMBS — SPECIFIC THYROID SIGNS
| Sign | Expected Finding | Significance |
|---|---|---|
| Pretibial myxoedema | Present — bilateral — non-pitting, indurated, brownish-orange thickened skin over anterior shins | Specific to Graves' disease (~1–5%); caused by GAG deposition in dermis |
| Proximal weakness | Present — difficulty rising from squat without using hands | Thyrotoxic myopathy (proximal > distal) |
| Ankle jerks | Brisk with fast relaxation | Thyrotoxicosis |
| Pedal oedema | Absent | No cardiac failure |
EXAMINATION SUMMARY STATEMENT
On examination, Madam Hasnah is a 67-year-old Malay female who is alert, conscious and oriented, sitting upright and not in acute distress. She appears mildly thin with warm, moist skin, a fine postural tremor of the hands, tachycardia at 104 bpm, and a staring, wide-eyed expression.Thyroid examination reveals a diffusely enlarged, firm, smooth, non-tender goitre moving on swallowing, with a palpable thrill and audible bruit at both inferolateral poles, consistent with Graves' disease.Ophthalmic examination reveals bilateral lower lid retraction (RE 2 mm, LE 3 mm inferior scleral show), bilateral upper lid retraction with positive Dalrymple and von Graefe signs, lagophthalmos (RE 2 mm, LE 3 mm gap), bilateral injected conjunctiva with hyperaemia over rectus insertions, bilateral periorbital oedema and chemosis, bilateral proptosis (RE 22 mm, LE 24 mm by Hertel), restricted upgaze bilaterally with positive forced duction test, elevated IOP on upgaze (RE 24, LE 26 mmHg), left corneal haziness with dense punctate fluorescein staining, and choroidal folds on fundoscopy of the left eye. A trace RAPD and mild colour vision reduction are noted in the left eye. CAS = 7/7, consistent with highly active disease.Systemically, features of thyrotoxicosis are present including tachycardia, fine tremor, brisk reflexes, proximal myopathy, hyperactive bowel sounds, and pretibial myxoedema bilaterally.These findings are consistent with Graves' Ophthalmopathy, Moderate-to-Severe, Highly Active (CAS 7/7), with emerging signs of possible left dysthyroid optic neuropathy requiring urgent further assessment and initiation of systemic immunosuppression.
⚠️ Exam tip: When presenting, state at the end — "In summary, this patient has clinical features of active moderate-to-severe Graves' ophthalmopathy with a CAS of 7/7, with concern for early dysthyroid optic neuropathy of the left eye, and I would like to urgently assess colour vision, arrange Humphrey visual fields, and initiate IV methylprednisolone in discussion with the endocrinology team." — This will impress any examiner.
I'm having viva in few minutes, prepare me generally. Dr is asking other things as well like, ulcer, sudden & gradual loss of visions and all