Serous otitis media
Reading File
Finding Sources
Searching PubMed
"otitis media with effusion" management
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I have everything needed for a comprehensive answer. Here is the full review:
Serous Otitis Media (Otitis Media With Effusion)
Definition
Serous otitis media - also called otitis media with effusion (OME) or "glue ear" - is defined as a serous or mucoid (non-purulent) collection of fluid within the middle ear space without clinical signs of acute inflammation (no otalgia, fever, or bulging tympanic membrane). It differs fundamentally from acute otitis media (AOM) in the absence of acute symptoms. The effusion can persist for hours or last for decades, making duration-based classification unhelpful.
- Shambaugh Surgery of the Ear, p. 451
- Tintinalli's Emergency Medicine, p. 144
Epidemiology
-
Point prevalence in children: up to 20% on screening tests
-
More than 2 million episodes are diagnosed annually in the United States, with an estimated annual cost of $4 billion
-
Peak incidence: 6 months to 4 years of age
-
By age 3 years, nearly all children have experienced at least one OME episode
-
90% of children will be affected before school age
-
Cummings Otolaryngology, p. 3767
-
Tintinalli's Emergency Medicine, p. 144
Risk Factors
Host-related:
- Onset of first AOM before 12 months of age
- Male sex
- Genetic predisposition
- Craniofacial abnormalities (cleft palate)
- Immunodeficiency
- Adenoid hypertrophy
- Down syndrome and other craniofacial syndromes
Environmental:
- Low socioeconomic status
- Recurrent upper respiratory tract infections
- Daycare attendance
- Tobacco smoke exposure
- Pacifier use
- Fall/winter season
Protective factor: Breastfeeding
- Cummings Otolaryngology, p. 3767
Pathophysiology
Eustachian Tube Dysfunction
The Eustachian tube (ET) is central to OME pathogenesis. Its functions are to protect the middle ear from nasopharyngeal pathogens, drain middle ear secretions, and equalize pressure. In children, the ET is:
- Shorter and more horizontal than in adults
- More flexible and more easily obstructed
ET dysfunction causes inadequate gas exchange, leading to progressively negative middle ear pressure, which drives transudation of fluid that fails to clear. Dysfunction arises from:
- Inflammatory causes - mucosal edema from allergic disease, laryngopharyngeal/gastroesophageal reflux, ciliary dysmotility
- Anatomic obstruction - prominent adenoid tissue, synechiae, nasopharyngeal masses
- Congenital anomalies - cleft palate, palatal myopathies
Biofilm Hypothesis
Modern research has shifted understanding away from a purely mechanical model. Evidence now supports OME as a chronic inflammatory state driven by bacterial biofilms:
- Biofilm-aggregated bacteria (primarily H. influenzae) are sequestered on the mucosal surface rather than free-floating in the fluid, explaining why standard cultures are negative
- Hall-Stoodley (2006) found biofilms in 92% of pediatric OME patients by confocal laser-scanning microscopy
- Bacterial toxins initiate a cascade of pro-inflammatory cytokines: TNF-α, IL-1β, IL-6, IL-8 and immunoregulatory cytokines IL-2, IL-4, IL-5, IL-10, IFN-γ
- TNF-α and IL-1β are the primary drivers of middle ear and mastoid inflammation
Effusion Formation
The inflammatory response causes:
- Proliferation of mucosal lining
- Secretion of mucus by goblet cells
- Differentiation of basal cells into goblet and ciliated cells
- Production of mucins (glycoproteins that determine viscosity) - the primary determinant of effusion type (serous vs. glue-like/mucoid)
Children tend to have more mucoid effusions; adults tend toward more serous effusions.
- Shambaugh Surgery of the Ear, pp. 450-452
Pathology / Otoscopic Appearance
On otoscopy, OME shows:
- An amber-colored or yellowish effusion visible behind an intact tympanic membrane
- Air-fluid levels or bubbles may be seen
- Reduced tympanic membrane mobility on pneumatic otoscopy
- Retracted or dull TM; loss of the light reflex in some cases
- No erythema, no bulging (distinguishing from AOM)
With long-standing OME:
- Atrophy of the tympanic membrane
- Ossicular fixation and erosion may occur
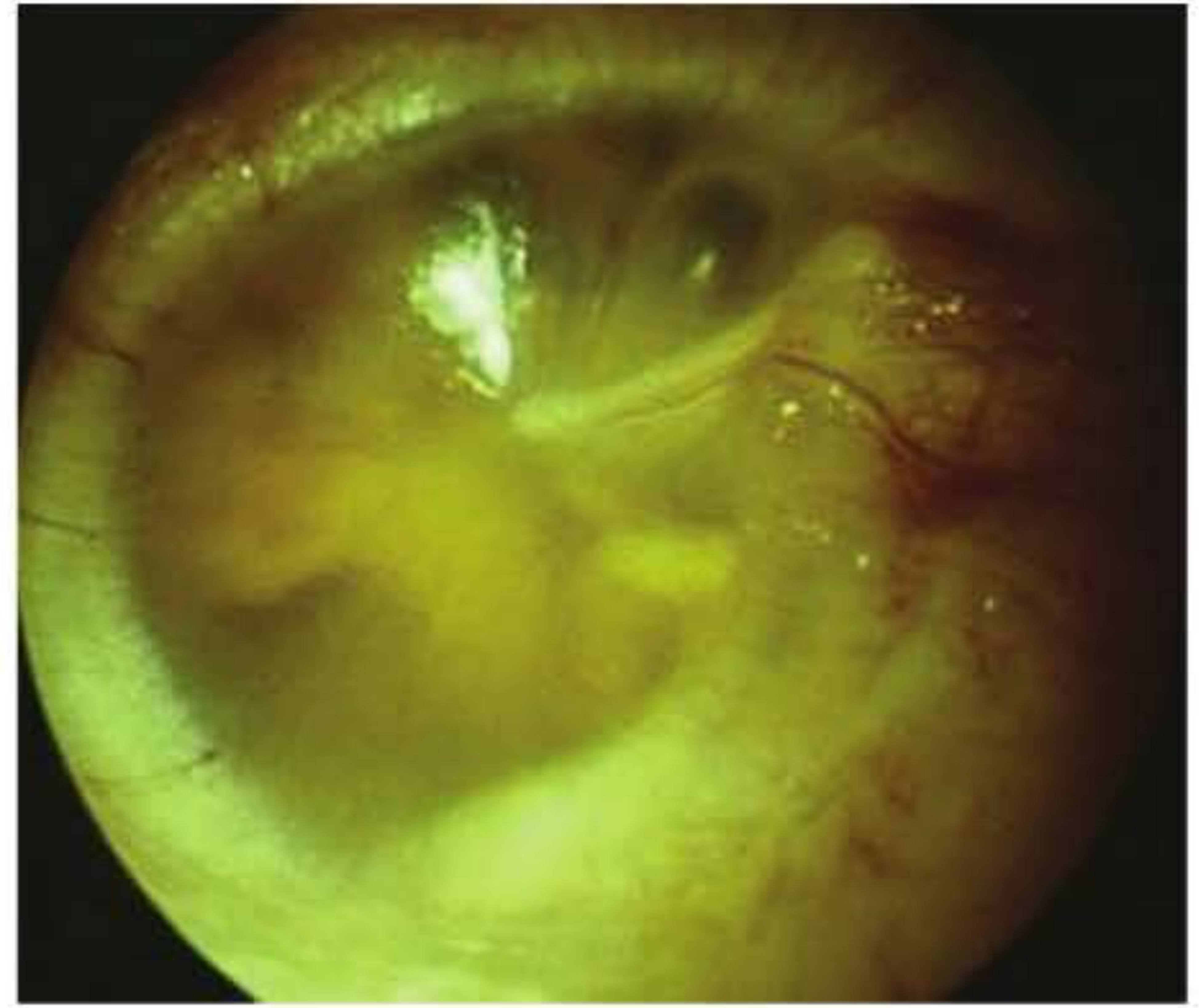
Otitis media with effusion: amber-colored effusion behind an intact tympanic membrane. A small bubble can be seen near the light reflex. (Shambaugh Surgery of the Ear)
Clinical Features
Many children are asymptomatic. When symptoms occur:
- Conductive hearing loss - mild to moderate, typically 10-20 dB (can reach 25 dB HL)
- Aural fullness, popping sensation
- Mild intermittent ear pain
- Balance problems and vestibular dysfunction
- Speech, language, and learning difficulties in children with persistent bilateral disease
- Behavioral problems
Adults additionally present with: aural fullness, intermittent conductive hearing loss, tinnitus.
Diagnosis
Tympanometry is the key diagnostic tool:
- Type B (flat) tympanogram - no compliance peak - indicates middle ear effusion
- Type C - negative pressure with reduced compliance
Audiometry: Conductive hearing loss (air-bone gap); referral recommended if OME persists ≥3 months, or at any time when language delay or significant hearing loss is suspected.
Otoscopy: Amber/yellow effusion, reduced TM mobility on pneumatic otoscopy, possible air-fluid levels or bubbles.
In children where standard audiometry is not possible (e.g., Down syndrome with narrow canals), ABR under general anaesthetic may be required.
High-Risk Groups for Developmental Complications
Children at higher risk of adverse developmental outcomes from OME (Box 199.1, Cummings):
- Permanent hearing loss independent of OME
- Suspected or confirmed speech and language delays
- Autism spectrum disorder
- Down syndrome or craniofacial disorders with cognitive delay
- Cleft palate
- Blindness or uncorrectable visual impairment
- Developmental delay
These children warrant earlier and more aggressive intervention.
Management
1. Watchful Waiting (First-Line for Most)
- Most children resolve spontaneously within several months
- For children not at risk for speech/language/learning disabilities: 3 months of observation with monitoring is recommended
- Review at 3-6 month intervals until MEE resolves
- Proceed to intervention if: OME persists >3 months with hearing loss, language/learning delay identified, or structural TM abnormalities develop
2. Medical Treatments
| Treatment | Evidence | Recommendation |
|---|---|---|
| Antibiotics | Short-term resolution benefit; no long-term benefit; no prevention of tube insertion; ~10% adverse events (diarrhea, rash) | Not recommended for routine OME |
| Decongestants ± antihistamines | No benefit; associated with harm | Not recommended |
| Oral corticosteroids | Short-term MEE resolution (especially with antibiotics); no long-term benefit; no hearing improvement | Not recommended |
| Topical (intranasal) corticosteroids | No benefit shown in meta-analysis | Not recommended |
| Auto-inflation (Otovent device) | Large RCT (n=320) showed benefit in school-aged children with recent-onset OME | May be considered for mild/recent onset |
Recent evidence note: A 2025 Cochrane review (PMID 41307300) on decongestants/antihistamines for acute OM in children reinforces that these drugs lack benefit and may cause harm - consistent with current guidelines.
3. Surgical Treatment
Myringotomy alone: Ineffective long-term (perforation closes in 2-3 weeks); not recommended.
Tympanostomy tubes (grommets):
- Standard surgical treatment for persistent OME
- Alleviate conductive hearing loss by draining fluid as a proxy for the dysfunctional ET
- Effect on hearing is modest and diminishes after 6-9 months (median tube function duration)
- Indications:
- Persistent MEE with documented hearing difficulties after 3 months
- Children at risk for, or already with, speech/language/learning disabilities (Box 199.1)
- Hearing level ≥25 dB HL in both ears persisting ≥3 months
- Largest benefit in young children in high-infection environments (e.g., daycare) and older children with bilateral significant hearing loss
Adenoidectomy:
- Most beneficial in children aged ≥4 years
- As adjunct to tympanostomy tube insertion: reduces need for reinsertion by ~10%
- Improves ET and middle ear function
- The TARGET study supports adjuvant adenoidectomy in children >3 years undergoing grommet insertion
Balloon Eustachian tube dilation: Proposed as a novel option but currently no evidence to support use in OME.
Hearing aids: In the UK, recommended for children with persistent bilateral OME when surgery is contraindicated or in Down syndrome. In the US, tympanostomy tubes are the standard even in Down syndrome.
- Cummings Otolaryngology, pp. 3773-3775
- Tintinalli's Emergency Medicine, p. 144
Complications of Untreated/Persistent OME
- Conductive hearing loss with speech/language delay
- Tympanic membrane atrophy
- Ossicular fixation and erosion
- Balance and vestibular dysfunction
- Retraction pockets - may progress to cholesteatoma
- Adhesive otitis media
Key Differentials
| Feature | AOM | OME (Serous OM) |
|---|---|---|
| Otalgia | Marked | Absent or mild |
| Fever | Common | Absent |
| TM appearance | Bulging, erythematous | Amber/retracted, intact |
| Effusion type | Purulent | Serous/mucoid |
| TM mobility | Reduced | Reduced (no bulge) |
| Tympanogram | Type B or C | Type B |
| Treatment | Antibiotics | Watchful wait / tubes |
Sources:
- Cummings Otolaryngology Head and Neck Surgery (Schilder section, pp. 3767-3775)
- Shambaugh Surgery of the Ear (pp. 450-452)
- Tintinalli's Emergency Medicine (pp. 144-148)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 2
Recent evidence: Adenoidectomy vs. tympanostomy for OME (PMID 39254052, 2024 meta-analysis); adenoidectomy + tympanostomy vs. myringotomy alone (PMID 41544403, 2026 systematic review) - both support surgical options consistent with the textbook guidance above.
Tympanostomy tubes
Finding Sources
Searching PubMed
"tympanostomy tubes" OR "ventilation tubes" otitis media
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have comprehensive information from multiple textbooks. Here is the full structured response:
Tympanostomy Tubes (Ventilation Tubes / Grommets)
Overview
Tympanostomy tubes - also called ventilation tubes, pressure-equalizing (PE) tubes, or grommets - are small hollow cylinders surgically placed through the tympanic membrane (TM). They act as a mechanical proxy for a dysfunctional Eustachian tube by ventilating the middle ear, draining effusions, and equalizing pressure. Myringotomy alone without tube insertion is ineffective - the incision closes within days and the effusion recurs.
- Scott-Brown's Otorhinolaryngology, Vol. 2, p. 169
- Cummings Otolaryngology, p. 3774
Indications
Primary Indications
- Otitis media with effusion (OME) / Serous otitis media - persistent MEE with hearing difficulties after 3 months of watchful waiting
- Recurrent acute otitis media (rAOM) - typically ≥3 episodes in 6 months or ≥4 episodes in 12 months
- Eustachian tube dysfunction - with chronic negative middle ear pressure, TM retraction, or atelectasis
High-risk children warrant earlier/lower threshold insertion:
- Permanent hearing loss independent of OME
- Speech and language delays
- Autism spectrum disorder
- Down syndrome or craniofacial disorders (e.g., cleft palate)
- Blindness or uncorrectable visual impairment
- Developmental delay
Specific thresholds for OME (per guidelines):
-
Hearing level ≥25 dB HL in both ears persisting ≥3 months
-
Documented hearing difficulties after 3 months with risk factors for developmental delay
-
Cummings Otolaryngology, pp. 3773-3774
Types of Tympanostomy Tubes
Most tubes are variations of two fundamental designs:
1. Short-term / Grommet-type (e.g., Shepard, Shah, Armstrong, Donaldson)
- Standard first-line tube for most children
- Flanged design with short barrel
- Extrusion timeline: Up to 55% of Shepard tubes extrude within 6 months; Armstrong tubes ~50% by 12 months, 75% by 18 months
- Lower complication rates compared to long-term tubes
2. Long-term / T-tubes (e.g., Goode T-tube)
- T-shaped flanges on both ends anchor the tube in the TM for longer duration
- ~10% extruded by 6 months (vs. 55% for Shepard)
- Indications for T-tube: atrophic TM, multiple previous sets of grommets, or comorbidities such as cleft palate causing rapid re-accumulation
- Drawbacks: higher rates of persistent perforation (16.6% vs. 2.2% for short-term), plugging, infection, and TM thinning
Tube Materials
-
Available in Teflon (PTFE), silicone, titanium, gold- or silver oxide-coated versions
-
Titanium/gold/silver oxide coatings aim to reduce biofilm formation; in vitro evidence suggests benefit only if antibiotic-coated
-
Ionized processed silicone appears more resistant to biofilm, reducing tube plugging and post-operative otorrhoea
-
A recent trial (n=400) comparing tube materials/shapes found silicone tubes were associated with the longest time to first infection; Long Armstrong tubes were least prone to extrude
-
Cummings Otolaryngology, pp. 3774-3775
-
Scott-Brown's Otorhinolaryngology, Vol. 2, pp. 169-170
Surgical Procedure

Anaesthesia
- Most children: general anaesthesia
- Selected young children: office setting with local anaesthesia (laser-assisted myringotomy is an alternative)
Steps
- Binocular operating microscope - mandatory
- Cerumen and debris removal; full TM inspection for abnormalities
- Myringotomy incision in the anteroinferior quadrant of the pars tensa
- Radial or circumferential incision (no difference in extrusion rate)
- Anteroinferior placement lengthens tube survival (80% vs. 45% at 6 months compared to posteroinferior) and reduces perforation risk
- Never posterosuperior - risk of ossicular chain damage
- Aspiration of MEE (if present) through the incision
- If fluid too viscous: counter-incision inferiorly, or saline irrigation to assist aspiration
- Note: evidence is mixed on whether aspiration actually affects outcomes (some data shows no hearing benefit and possible increased tympanosclerosis from trauma)
- Tube inserted with alligator forceps
- Optional: topical antibiotic-steroid drops at time of insertion to reduce early infection (reduces rate from ~9% to ~1%)
- Cummings Otolaryngology, p. 3774
- Scott-Brown's Otorhinolaryngology, Vol. 2, pp. 169-170
Outcomes (Evidence)
Hearing
The UK MRC TARGET trial is the landmark RCT:
- At 3 months: +12 dB improvement in the ventilation tube group vs. non-surgical group
- At 12 months: difference becomes almost negligible as tubes extrude and OME naturally resolves in many
- Average hearing benefit over year 1: 5.7 dB
- Average benefit over 2 years: reduced to 3.1 dB
- Note: Even with a functioning tube, an air-bone gap of ~13 dB persists due to effusion and oedema around the ossicular chain
A Cochrane systematic review concluded:
- Grommets beneficial at 6 months (mean 12 dB better at 3 months, ~4 dB better at 6-9 months)
- Effects on hearing diminish in the first year; not maintained at 12 months
Long-term (25-year follow-up): Hearing no different from age- and gender-matched controls. Myringosclerosis was associated with a small 4-5 dB high-frequency loss; pars tensa atrophy with 3-4 dB overall loss.
Speech, Language, Development, Quality of Life
-
Trial evidence is limited but supports beneficial effects on speech, language, behaviour, cognitive function, and quality of life
-
Impact is largest in:
- Young children in high-infection environments (daycare)
- Older children with bilateral HL ≥25 dB HL persisting ≥3 months
- Children with developmental risk factors
-
Scott-Brown's Otorhinolaryngology, Vol. 2, pp. 170-172
Post-operative Follow-up
- First review: 2-3 months post-surgery (otoscopy, hearing assessment)
- Subsequent: every 6-12 months until tubes extrude and TM is confirmed intact
- Water precautions: swimming/bathing restrictions are traditionally advised, though evidence for their strict necessity is limited
Complications
Early Complications
| Complication | Incidence | Management |
|---|---|---|
| Tube otorrhoea (acute) | 10-50% | Topical fluoroquinolone drops (ciprofloxacin preferred; 1st line) |
| Early post-op infection around tube | 9% (→1% with prophylactic drops) | Topical antibiotic-steroid drops |
| Early tube extrusion | ~3.9% of ears | Re-insertion if indicated |
| Tube blockage/occlusion | Variable | Topical drops, suction clearance |
Otorrhoea - Key Points
- Most common complication: 10-50% incidence
- Causative organisms: Nontypeable H. influenzae, S. aureus, P. aeruginosa (often polymicrobial)
- Risk factors: young age, rAOM as indication, recurrent URTIs, older siblings
- First-line treatment: topical fluoroquinolone (ciprofloxacin/ofloxacin) ear drops
- Superior to oral antibiotics (failure rate 23% vs. 70% for oral amoxicillin in RCT)
- Ofloxacin preferred over ciprofloxacin to minimise resistance to a systemically used antibiotic
- Avoid aminoglycoside drops - risk of ototoxicity and vestibulotoxicity
- If no resolution after 2 weeks: culture from tube opening to guide therapy
- If yeast: topical antifungal (clotrimazole)
- Chronic/persistent otorrhoea refractory to treatment: consider tube removal (~4% of cases)
Late Complications
| Complication | Incidence | Notes |
|---|---|---|
| Tympanosclerosis / myringosclerosis | 32% (range 7-64%) | Most common structural complication; usually minimal hearing effect (4-5 dB HF loss) |
| Focal TM atrophy | 25% (range 1.6-75%) | 3-4 dB hearing loss; higher with persistent OME than from tubes per se |
| Persistent TM perforation | 4.8% overall (2.2% short-term; 16.6% long-term tubes) | Usually small; managed by myringoplasty once ET function confirmed adequate |
| Retraction pockets | 3.1% (range 0-22.7%) | May progress to cholesteatoma |
| Cholesteatoma | 0-6.5% | Whether caused by tubes or underlying pathology is debated; may result from epithelial ingrowth around tube |
| Granulation tissue | ~1% | Topical preparations; tube removal if persistent |
- Cummings Otolaryngology, pp. 3773-3775
- Scott-Brown's Otorhinolaryngology, Vol. 2, pp. 171-173
Persistent Perforation - Management
Before surgical closure:
- Ensure Eustachian tube function has improved
- Opposite ear TM should be intact and infection-free for at least 1 year
Surgical options:
- Myringoplasty with fat, surgical gel, paper patch, or reinforced skin closure strips
- Conventional tympanoplasty with fascia or perichondrium graft
Adjuvant Adenoidectomy
- Most beneficial in children ≥4 years (also considered ≥3 years per TARGET study)
- Reduces need for tube reinsertion by approximately 10% vs. tubes alone
- Acts by removing adenoid tissue that obstructs the ET orifice and serves as a bacterial reservoir
- Does not significantly improve hearing outcomes vs. tubes alone in the short term
Contraindications / Cautions
- Cleft palate: higher rates of early extrusion; T-tubes preferred
- Down syndrome: higher threshold for surgery in some guidelines; hearing aids may be first-line (UK) vs. tubes (US)
- Immunocompromise: higher infection risk post-insertion
- Single hearing ear: extra caution - risk of perforation or hearing damage
Recent Evidence Update
- PMID 38666491 (Lam et al., Laryngoscope 2024): Systematic review - quality of life outcomes after pediatric otitis media surgery; confirms benefit
- PMID 40673630 (Clementi et al., Laryngoscope 2025): Systematic review of complications with automated tympanostomy tube systems (iontophoresis-based office procedure) - a growing area
Sources:
- Cummings Otolaryngology Head and Neck Surgery (pp. 3774-3775)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 2 (pp. 169-173)
- K.J. Lee's Essential Otolaryngology (p. 217)
This is a shared conversation. Sign in to Orris to start your own chat.