Explain full ecg all cases related disease full interpretation also with Diagram
Reading File
Finding Sources
Searching the Web
ECG interpretation all disease patterns diagrams complete guide 2024
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Loading Image
Reading File
Complete ECG Interpretation Guide: All Cases & Related Diseases
Sources: Costanzo Physiology 7e, Braunwald's Heart Disease, Harrison's Principles of Internal Medicine 22e, ROSEN's Emergency Medicine, Tintinalli's Emergency Medicine, Washington Manual of Medical Therapeutics, Goldman-Cecil Medicine
Part 1: ECG Basics - The Normal Waveform
The ECG measures tiny potential differences on the body surface that reflect the electrical sequence of depolarization and repolarization throughout the myocardium.

Waves, Intervals & Segments
| Component | What it Represents | Normal Values |
|---|---|---|
| P wave | Atrial depolarization | Duration <120 ms, amplitude <2.5 mm |
| PR interval | Atrial depol → ventricular depol (AV node conduction) | 120-200 ms (0.12-0.20 s) |
| QRS complex | Ventricular depolarization | <120 ms (narrow = supraventricular) |
| ST segment | Between ventricular depol and repol (isoelectric) | At baseline (±0.5 mm) |
| T wave | Ventricular repolarization | Upright in I, II, V4-V6; inverted in aVR |
| QT interval | QRS + ST + T (full ventricular depol to repol) | Corrected QTc <440 ms men; <460 ms women |
Key principle: Intervals include waves; segments do not. A prolonged PR = AV conduction delay. A wide QRS = abnormal ventricular conduction.
Part 2: Standard 12-Lead ECG Layout
Limb leads: I, II, III (frontal plane)
Augmented: aVR, aVL, aVF (frontal plane)
Precordial: V1, V2, V3, V4, V5, V6 (horizontal plane)
Territorial Lead Groups (for localizing MI/ischemia)
| Territory | Leads Affected | Artery Involved |
|---|---|---|
| Anterior | V1-V4 | Left Anterior Descending (LAD) |
| Anterolateral | V1-V6, I, aVL | LAD proximal / diagonal |
| Lateral | I, aVL, V5-V6 | Left Circumflex (LCx) |
| Inferior | II, III, aVF | Right Coronary Artery (RCA; 80%) / LCx |
| Posterior | V7-V9 (tall R in V1-V2) | RCA or LCx |
| Right Ventricular | V3R-V6R (right-sided leads) | RCA proximal |
| Left Main / Proximal LAD | aVR elevation + diffuse ST depression | Left main coronary artery |
Part 3: Systematic ECG Interpretation Steps
Always read an ECG in this order to avoid missing diagnoses:
- Rate - Count R-R intervals. Normal: 60-100 bpm. 300 / (number of large boxes between R peaks)
- Rhythm - Regular or irregular? Is every P followed by a QRS?
- Axis - Normal: -30° to +90°. Left axis deviation (LAD) vs. Right axis deviation (RAD)
- P wave - Present? Morphology? Relationship to QRS?
- PR interval - Short (<120 ms = pre-excitation?) or long (>200 ms = AV block)?
- QRS duration - Narrow (<120 ms) vs. wide (>120 ms = BBB, aberrancy, ventricular origin)
- ST segment - Elevation? Depression? Morphology (convex/concave/saddle)?
- T wave - Upright, inverted, peaked, biphasic?
- QT interval - Corrected QTc (Bazett formula: QT / √RR)
- U wave - Present? (hypokalemia, bradycardia)
Part 4: ECG Patterns by Disease - Complete Reference
4.1 Sinus Rhythms
Normal Sinus Rhythm
- Rate: 60-100 bpm
- Upright P in I, II; inverted in aVR
- Every P followed by QRS (1:1)
- PR interval 120-200 ms, QRS <120 ms
Sinus Tachycardia
- Rate >100 bpm, identical morphology to NSR
- Causes: fever, pain, anxiety, hypovolemia, PE, anemia, hyperthyroidism, drugs
- NOT a primary arrhythmia - always look for the underlying cause
Sinus Bradycardia
- Rate <60 bpm, normal P-QRS-T morphology
- Causes: athletes (normal), hypothyroidism, hypothermia, vasovagal, beta-blockers, sick sinus syndrome, inferior MI (RCA occlusion affects SA node artery)
- Treat only if symptomatic (atropine, pacemaker)
Sinus Arrhythmia
- Rate varies with respiration (increases on inspiration)
- Normal in young people; phasic variation in R-R with preserved P wave morphology
4.2 Atrial Arrhythmias
Atrial Fibrillation (AF)
ECG hallmarks:
- Absence of discrete P waves (replaced by chaotic fibrillatory baseline, especially in V1)
- Irregularly irregular ventricular rate
- Narrow QRS (unless bundle branch block)
- Ventricular rate typically 100-180 bpm if uncontrolled
Associated diseases: hypertension, valvular heart disease (mitral stenosis/regurgitation), coronary artery disease, cardiomyopathy, hyperthyroidism, alcohol ("holiday heart"), COPD, pulmonary embolism, post-cardiac surgery
Key risks: stroke (CHA2DS2-VASc score), tachycardia-induced cardiomyopathy, hemodynamic instability
Atrial Flutter
- Regular sawtooth flutter waves at ~300 bpm, best seen in II, III, aVF, V1
- Typically 2:1 conduction → ventricular rate ~150 bpm (classic clue: any regular tachycardia at ~150 bpm = flutter until proven otherwise)
- Associated diseases: similar to AF; also after cardiac surgery, structural heart disease
Multifocal Atrial Tachycardia (MAT)
- At least 3 different P wave morphologies
- Irregularly irregular rhythm at 100-180 bpm
- PR intervals vary
- Frequently confused with AF
- Classic cause: COPD, hypoxia, hypomagnesemia
Premature Atrial Contractions (PAC)
- Early, abnormal P wave morphology
- Narrow QRS (unless aberrant conduction)
- Followed by incomplete compensatory pause
- Common triggers: caffeine, stress, alcohol
4.3 AV Conduction Blocks
The ECG from Rosen's/Washington Manual illustrates all degrees of AV block:

First-Degree AV Block
- PR interval >200 ms (>5 small squares) on every beat - no dropped beats
- Conduction delay usually within AV node
- Causes: vagal tone (athletes), inferior MI, digitalis, beta-blockers, calcium channel blockers, myocarditis, aging
- Usually benign; no treatment needed
Second-Degree AV Block - Mobitz Type I (Wenckebach)
- Progressive PR prolongation until one QRS is dropped
- After the dropped beat, PR resets to shortest interval
- RR intervals progressively shorten before the dropped beat
- Classic "group beating" pattern
- Block is in the AV node - relatively benign
- Causes: inferior MI, increased vagal tone, digitalis toxicity
- Rarely needs pacing (treat underlying cause)
Second-Degree AV Block - Mobitz Type II
- Fixed PR interval before an unexpected dropped QRS
- No warning - PR does not prolong
- QRS often wide (bundle branch block pattern)
- Block is infranodal (His-Purkinje) - more dangerous
- Causes: anterior MI, fibrosis of conduction system, myocarditis
- Always requires permanent pacemaker - high risk of sudden complete block
2:1 AV Block
- Every other P wave is blocked (2 P waves per 1 QRS)
- Cannot distinguish Mobitz I vs II on ECG alone
- If PR <160 ms + wide QRS = likely Mobitz II (infranodal)
- If PR >200 ms + narrow QRS = likely Mobitz I (nodal)
Third-Degree (Complete) AV Block
- Complete AV dissociation - P waves and QRS complexes march out independently
- Atrial rate > ventricular rate (P rate normal; QRS rate 20-40 bpm if ventricular escape, 40-60 bpm if junctional escape)
- Wide QRS = escape from ventricles (His-Purkinje) → unstable, urgent pacing needed
- Narrow QRS = escape from AV junction → more stable
- Causes: inferior MI (usually transient), anterior MI (usually permanent), Lyme disease, degenerative (Lenègre/Lev disease), congenital, digitalis toxicity
4.4 Myocardial Ischemia & Infarction
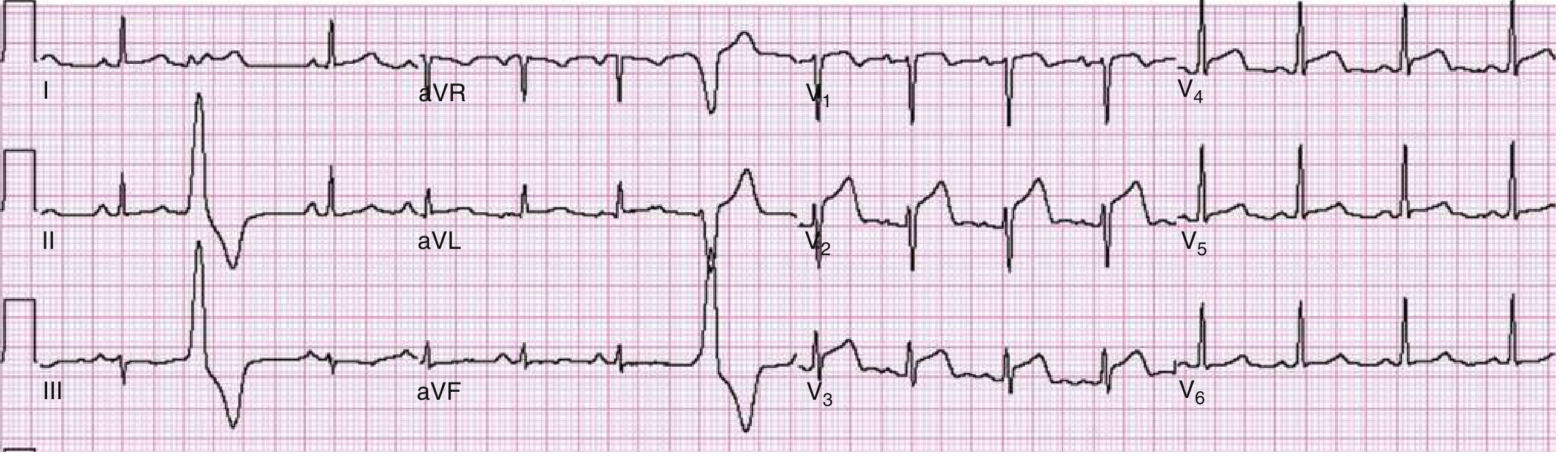
Acute STEMI - Anterior (V1-V4)
Acute STEMI - Anterolateral (V2-V6, I, aVL)
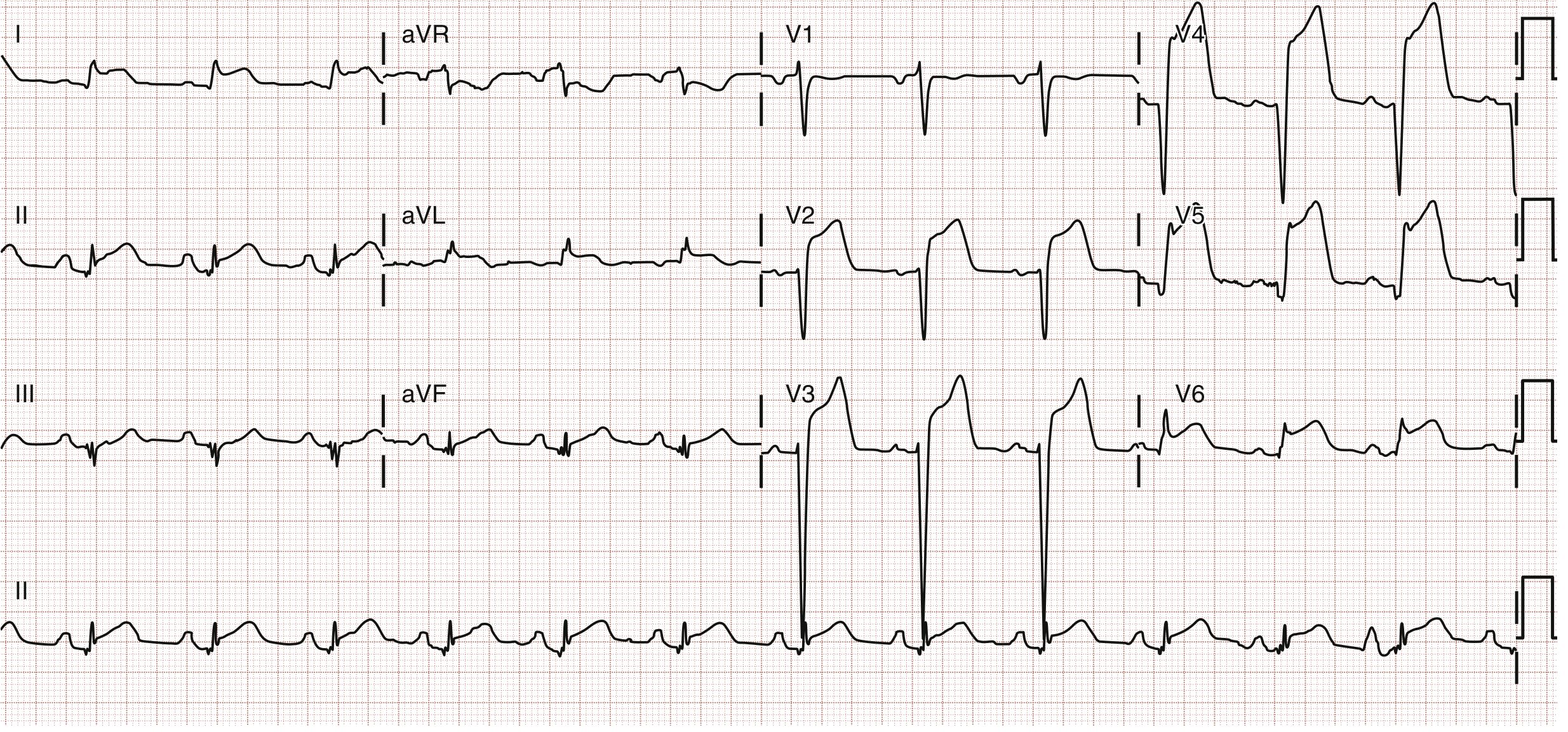
STEMI Diagnosis Criteria (Harrison's 22e, ROSEN's)
- New ST elevation at the J point in ≥2 contiguous leads:
- ≥2 mm in V2-V3 (men ≥40 yr); ≥2.5 mm (men <40 yr); ≥1.5 mm (women)
- ≥1 mm in all other leads
- New LBBB with symptoms = STEMI equivalent
- Posterior MI: tall R and ST depression in V1-V2 (mirror image)
ECG Evolutionary Changes in STEMI (temporal sequence)
| Timing | ECG Change |
|---|---|
| Minutes (hyperacute) | Tall, peaked T waves ("hyperacute T waves") |
| Hours (acute) | ST elevation, loss of R wave amplitude |
| Hours-days | Q wave formation (>40 ms or >25% of R wave height) |
| Days | ST elevation decreases, T wave inversion develops |
| Weeks-months | Q waves may persist permanently; T waves normalize |
NSTEMI / Unstable Angina
- ST depression ≥0.5-1 mm (horizontal or downsloping) in ≥2 leads
- T wave inversion (deep, symmetric)
- No Q waves, no ST elevation
- Diagnosis confirmed with rising troponin (NSTEMI) vs. no biomarker rise (UA)
Left Main / Proximal LAD Occlusion
- ST elevation in aVR (>1 mm) + diffuse ST depression in ≥6 leads
- ST elevation in aVR > ST elevation in V1 = left main disease
- ST elevation in V1 > aVR = proximal LAD
Right Ventricular Infarction
- Inferior STEMI (II, III, aVF) + ST elevation in V1
- Confirmed with right-sided leads: V4R most sensitive
- Clinical triad: hypotension + JVD + clear lungs in inferior MI
- Avoid nitrates (preload-dependent)
de Winter Pattern (LAD Equivalent)
- Upsloping ST depression at J point in precordial leads
- Tall, symmetric T waves
- ST elevation in aVR
- Equivalent to anterior STEMI - needs urgent PCI
Wellens Syndrome (LAD "warning")
- Type A: biphasic T wave in V2-V3 (small positive then negative)
- Type B: deep symmetric T wave inversion in V2-V3
- Represents reperfused LAD with critical stenosis - patient is pain-free during ECG
- Do NOT perform stress test - high risk of massive anterior MI
ST Elevation Mimics (non-MI causes)
| Condition | ECG Clue |
|---|---|
| Early repolarization (BER) | J-point notching, concave ST, diffuse, young patient |
| Pericarditis | Saddle-shaped ("saddleback") diffuse ST elevation; PR depression; no reciprocal changes |
| Left ventricular hypertrophy | Strain pattern in V5-V6 (down-sloping ST depression) |
| LBBB | Secondary ST/T changes (discordant) |
| Brugada syndrome | Coved or saddleback pattern in V1-V3 |
| Hyperkalemia | Wide QRS, peaked T, sine wave |
| Takotsubo (stress cardiomyopathy) | Diffuse ST elevation then deep T inversions |
4.5 Bundle Branch Blocks
Right Bundle Branch Block (RBBB)
- QRS ≥120 ms
- RSR' ("rabbit ears") in V1 - broad terminal R
- Wide S wave in I and V6 (slurred)
- T wave inversion in V1-V3 (secondary change, normal)
- Causes: normal variant, pulmonary embolism (new RBBB = PE until proven otherwise), RV strain, right heart disease, anterior MI, degenerative
Left Bundle Branch Block (LBBB)
- QRS ≥120 ms
- Broad, notched R in I, aVL, V5-V6 (M-shaped)
- No septal Q waves in I, V5-V6
- Deep S in V1 (QS or rS pattern)
- ST/T discordant (ST/T in opposite direction to main QRS deflection)
- Causes: hypertension, coronary artery disease, cardiomyopathy, anterior MI
- New LBBB with chest pain = STEMI equivalent
Left Anterior Fascicular Block (LAFB)
- Left axis deviation (QRS axis -45° to -90°)
- qR in I, aVL; rS in II, III, aVF
- QRS <120 ms (unless combined with RBBB)
- Causes: hypertension, coronary disease, anterior MI
Left Posterior Fascicular Block (LPFB)
- Right axis deviation (+90° to +180°)
- rS in I, aVL; qR in II, III, aVF
- Diagnosis of exclusion (must rule out RVH, lateral MI, PE)
Bifascicular Block
- RBBB + LAFB: most common bifascicular block
- RBBB + LPFB: less common, more serious
4.6 Ventricular Arrhythmias
Wide-Complex Tachycardia Algorithm
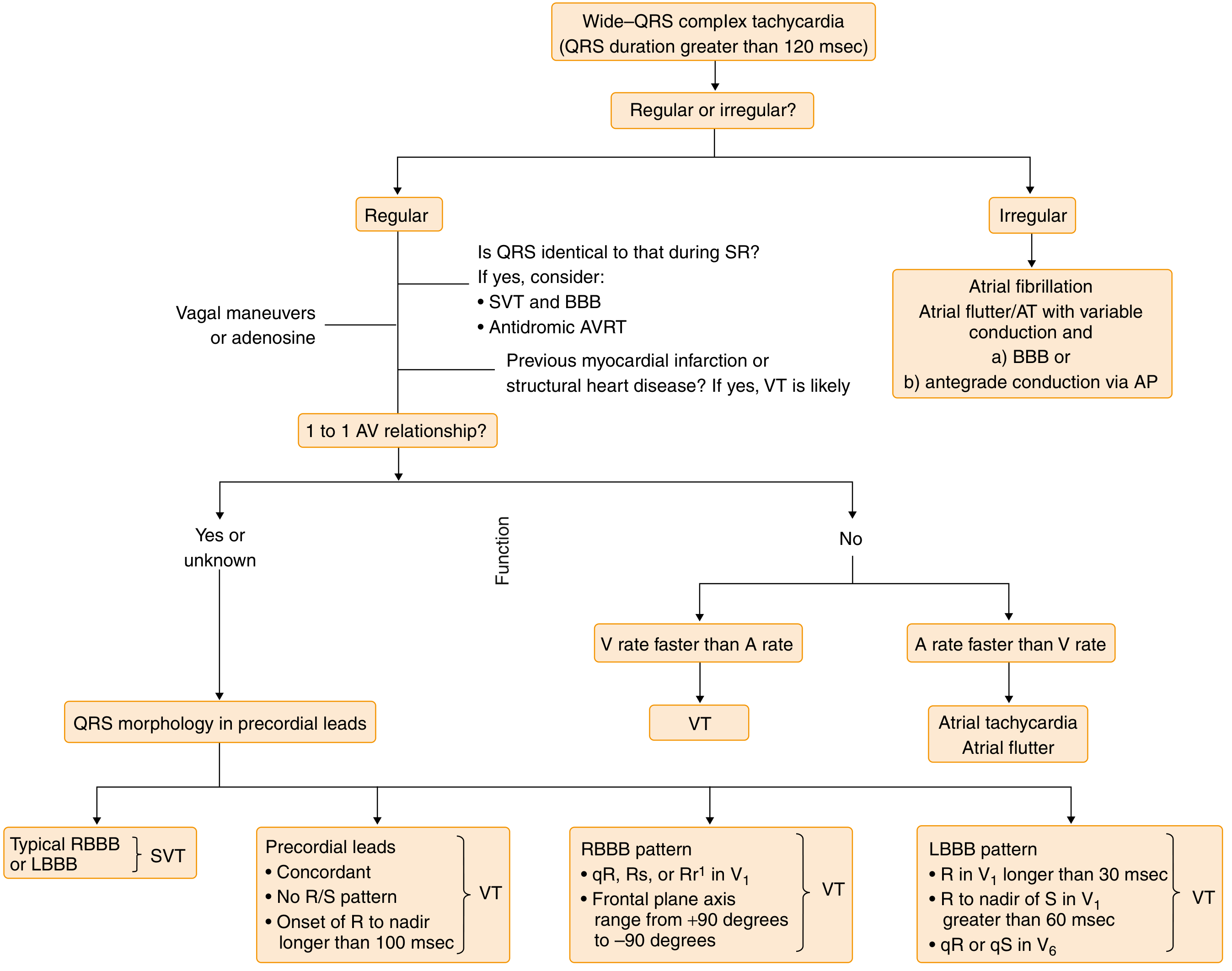
Ventricular Tachycardia (VT)
- Wide QRS >120 ms, rate >100 bpm, regular
- AV dissociation (P waves march through at different rate from QRS) - pathognomonic
- Fusion beats and capture beats (sinus QRS appears mid-tachycardia)
- Concordance in precordial leads (all positive or all negative)
- Brugada criteria, Josephson criteria, Vereckei criteria for VT vs SVT
- Causes: coronary artery disease (scar), cardiomyopathy, channelopathies, electrolyte disturbances
- Treat as VT until proven otherwise - hemodynamic instability → immediate cardioversion
Ventricular Fibrillation (VF)
- Chaotic, completely irregular, no identifiable waves
- Rate >300 bpm (undulations vary in amplitude and morphology)
- No effective cardiac output - cardiac arrest
- Immediate defibrillation + CPR
Torsades de Pointes (TdP)
- Polymorphic VT with QRS complexes that "twist" around the isoelectric axis
- Occurs on background of prolonged QT
- Causes: QT-prolonging drugs (antiarrhythmics, antipsychotics, antibiotics), hypokalemia, hypomagnesemia, congenital Long QT syndrome
- Treatment: IV magnesium, correct electrolytes, remove offending drug; not amiodarone (further prolongs QT)
Premature Ventricular Contractions (PVC)
- Wide, bizarre QRS with no preceding P wave
- Compensatory pause (full compensatory)
- T wave in opposite direction to QRS (discordant)
- Rule of bigeminy (PVC every other beat), trigeminy (every 3rd), couplets (2 in a row)
- Frequent PVCs (>10,000/day or >15%) can cause PVC-induced cardiomyopathy
4.7 Supraventricular Tachycardias (SVT)
AVNRT (most common SVT)
- Narrow complex tachycardia, rate 150-250 bpm, regular
- P waves buried in or just after QRS (retrograde P in V1 as pseudo-R')
- Abrupt onset and termination
- Mechanism: re-entry circuit in AV node
- Treatment: Valsalva, adenosine, calcium channel blockers
AVRT (Wolff-Parkinson-White - WPW)
- Orthodromic AVRT: narrow QRS (most common WPW tachycardia)
- Antidromic AVRT: wide QRS (uses accessory pathway anterograde)
- Delta wave + short PR + wide QRS in sinus rhythm = WPW pattern
- Pre-excited AF in WPW: irregular wide-complex tachycardia, very fast (>200 bpm), life-threatening - DO NOT give AV nodal blockers (adenosine, verapamil, digoxin) - use procainamide or cardioversion
Junctional Tachycardia
- Narrow QRS, rate 60-130 bpm
- Retrograde P waves (inverted in II, III, aVF) before, during, or after QRS
- Causes: digitalis toxicity, inferior MI, post-cardiac surgery
4.8 QT Interval Abnormalities
Long QT Syndrome (LQTS)
- QTc >440 ms (men), >460 ms (women)
- Risk of TdP and sudden cardiac death
- Congenital (LQT1, LQT2, LQT3, etc.) or acquired (drugs, electrolytes)
| Type | Gene | Trigger | T Wave |
|---|---|---|---|
| LQT1 | KCNQ1 | Exercise (swimming) | Broad-based T |
| LQT2 | HERG | Auditory triggers, sleep | Low-amplitude notched T |
| LQT3 | SCN5A | Sleep/rest | Late peaked T, long ST segment |
Short QT Syndrome
- QTc <340 ms
- Risk of VF and AF
- Tall, peaked T waves, short ST segment
4.9 Specific Disease-Related ECG Patterns
Pulmonary Embolism (PE) - "S1Q3T3"
- Sinus tachycardia (most common finding)
- S wave in lead I + Q wave in III + T wave inversion in III
- New RBBB or right axis deviation
- T wave inversion V1-V4 (right heart strain)
- P pulmonale (peaked P >2.5 mm in II)
Pericarditis
- Diffuse saddle-shaped ST elevation (concave upward) in most leads except aVR and V1
- PR depression (key finding - nearly pathognomonic)
- Reciprocal ST depression and PR elevation in aVR
- Evolves through 4 stages over weeks
- No reciprocal ST changes (unlike MI)
Hypertrophic Cardiomyopathy (HCM)
- Left ventricular hypertrophy (LVH) criteria (Sokolow-Lyon: S in V1 + R in V5 or V6 >35 mm)
- Deep, narrow Q waves in lateral leads (I, aVL, V5-V6) - "septal Q waves"
- Left axis deviation
- ST depression and T wave inversion (strain pattern)
Hyperkalemia
| K+ level | ECG Change |
|---|---|
| 5.5-6.5 mEq/L | Tall, peaked, narrow ("tent-shaped") T waves |
| 6.5-7.5 mEq/L | Prolonged PR, widened QRS |
| 7.5-8.5 mEq/L | Loss of P waves, further QRS widening |
| >8.5 mEq/L | Sine wave pattern, VF, asystole |
Hypokalemia
- Flattened/inverted T waves
- Prominent U waves (>1 mm or taller than T wave)
- ST depression
- Prolonged QU interval (mistaken for QT prolongation)
Hypercalcemia
- Short QT interval (shortened ST segment)
- Wide T waves
- Bradycardia, prolonged PR
Hypocalcemia
- Prolonged QT (long ST segment, T wave normal)
Digitalis Toxicity
- "Scooped" or "hockey-stick" ST depression (Salvador Dali mustache sign)
- Shortened QT
- Bradycardia, AV blocks, junctional rhythms, bidirectional VT (severe toxicity)
- Bidirectional VT (alternating QRS axis) is hallmark of severe digoxin toxicity
Hypothermia
- Osborn (J) wave: positive deflection at J point (junction of QRS and ST), best in V4-V6 and inferior leads
- Bradycardia, prolonged intervals (PR, QRS, QT)
- Atrial and ventricular arrhythmias
- Osborn waves increase in amplitude as temperature falls
Brugada Syndrome
- Type 1 (diagnostic): Coved-type ST elevation ≥2 mm with T wave inversion in V1-V2 (or V1-V3)
- Type 2/3: Saddleback pattern (less specific - may require sodium channel blocker provocation)
- Risk of VF and sudden death - ICD indicated
- Underlying mutation: SCN5A (sodium channel)
- Unmasked by: fever, cocaine, antiarrhythmic drugs, alcohol
Wolff-Parkinson-White (WPW) - Sinus Rhythm
- Short PR <120 ms
- Delta wave (slurred QRS upstroke - initial pre-excitation)
- Wide QRS (>120 ms)
- Pseudo Q waves in inferior leads can mimic inferior MI
4.10 Cardiomyopathy ECG Patterns
Dilated Cardiomyopathy
- Poor R wave progression in precordial leads
- LBBB pattern common
- Low voltage
- Non-specific ST-T changes
- AF common
Hypertrophic Cardiomyopathy (HCM)
- LVH pattern with strain
- Deep narrow septal Q waves in I, aVL, V5-V6
- Often confused with inferior or lateral MI
Arrhythmogenic RV Cardiomyopathy (ARVC)
- T wave inversion in V1-V3 (right precordial leads)
- Epsilon wave (small terminal notch after QRS in V1) - pathognomonic
- RBBB pattern
- QRS duration in V1 >110 ms (longer than in aVL/limb leads)
- PVCs with LBBB morphology (originate in RV)
Cardiac Amyloidosis
- Low voltage in limb leads despite LVH on echo ("voltage-mass discordance")
- Pseudo-infarct pattern (poor R wave progression, Q waves without infarction history)
- Conduction abnormalities (AV blocks, BBB)
4.11 Congenital and Channelopathy ECG Patterns
Catecholaminergic Polymorphic VT (CPVT)
- Normal resting ECG
- Exercise-induced bidirectional or polymorphic VT
- Ryanodine receptor mutation (RYR2)
Short QT Syndrome
- QTc <340 ms; tall, symmetric T waves
- Risk of AF, VF
Early Repolarization Syndrome
- J-point elevation ≥1 mm in ≥2 inferior or lateral leads
- Distinct notch or slur at J point
- Associated with idiopathic VF in some patients (inferior/lateral distribution highest risk)
Part 5: Quick-Reference Summary Table
| Condition | Rate | Rhythm | P Waves | PR | QRS | ST/T |
|---|---|---|---|---|---|---|
| Normal Sinus | 60-100 | Regular | Normal upright | 120-200 ms | <120 ms | Normal |
| Sinus Tachycardia | >100 | Regular | Normal | Normal | Normal | Normal |
| Sinus Bradycardia | <60 | Regular | Normal | Normal | Normal | Normal |
| Atrial Fibrillation | Variable | Irregular | Absent (fibrillatory) | None | Narrow* | - |
| Atrial Flutter | ~150 | Regular | Sawtooth 300/min | 2:1 block | Narrow* | - |
| 1° AV Block | Normal | Regular | Normal | >200 ms | Normal | Normal |
| Mobitz I | Normal | Irregular | Normal | Progressive ↑ | Narrow | Normal |
| Mobitz II | Normal | Irregular | Normal | Fixed then drop | Often wide | Normal |
| 3° AV Block | V<A | Irregular | Dissociated | None | Wide or narrow | Normal |
| Anterior STEMI | Normal/fast | Regular | Normal | Normal | Normal | ST↑ V1-V4 |
| Inferior STEMI | Normal/slow | Regular | Normal | Normal | Normal | ST↑ II,III,aVF |
| LBBB | Normal | Regular | Normal | Normal | >120 ms wide | Discordant |
| RBBB | Normal | Regular | Normal | Normal | RSR' in V1 | V1-V3 T inversion |
| VT | 100-250 | Regular | Dissociated | AV dissoc. | Wide >120 ms | Discordant |
| VF | >300 | Chaotic | None | None | None | Chaotic |
| PE | Fast | Regular | P pulmonale | Normal | RBBB/wide | S1Q3T3, T↓ V1-V4 |
| Pericarditis | Normal | Regular | Normal | Normal | Normal | Concave ST↑, PR↓ |
| Hyperkalemia | Slow | Variable | Absent (severe) | Long | Wide | Peaked T |
| Hypokalemia | Normal | Regular | Normal | Normal | Normal | Flat T, U wave |
| WPW | Variable | Variable | Normal | <120 ms (short) | Wide (delta) | ST/T secondary |
| Brugada | Normal | Normal | Normal | Normal | coved V1-V3 | ST↑ V1-V2, T↓ |
Part 6: Key Clinical Pearls
- Any regular tachycardia at ~150 bpm = suspect 2:1 atrial flutter until proven otherwise
- Wide-complex tachycardia = treat as VT unless you have absolute proof it is not - wrong treatment for VT (calcium channel blockers) can be fatal
- New LBBB + chest pain = STEMI equivalent - activate cath lab
- aVR ST elevation + diffuse depression = left main or proximal LAD occlusion
- Inferior STEMI + hypotension = get right-sided leads, suspect RV infarction - fluids, not nitrates
- PR depression = pericarditis (nearly pathognomonic)
- Osborn J waves = hypothermia (the colder, the bigger)
- Epsilon wave in V1 = ARVC
- Delta wave + short PR = WPW - do NOT give AV nodal blockers if AF is present
- Bidirectional VT = digitalis toxicity until proven otherwise
- Low voltage + pseudo-infarct + no coronary disease = think cardiac amyloidosis
- S1Q3T3 + sinus tachycardia = PE (though non-specific)
Sources: Costanzo Physiology 7e, p.149; ROSEN's Emergency Medicine (9e), Chapter 64; Braunwald's Heart Disease (11e); Harrison's Principles of Internal Medicine 22e, Chapter 252 & 286; Washington Manual of Medical Therapeutics, Chapter 7; Goldman-Cecil Medicine, Chapter 49 & 51; Tintinalli's Emergency Medicine, Chapter 18
This is a shared conversation. Sign in to Orris to start your own chat.