DVT management
Reading File
Finding Sources
Searching PubMed
"deep vein thrombosis"[MeSH Terms] AND "anticoagulants"[MeSH Terms]
Finding Sources
Searching PubMed
"deep vein thrombosis" AND treatment
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed for a comprehensive DVT management answer. Let me compile the full response.
Deep Vein Thrombosis (DVT) - Management
Source: Harrison's Principles of Internal Medicine, 22nd Edition (2025)
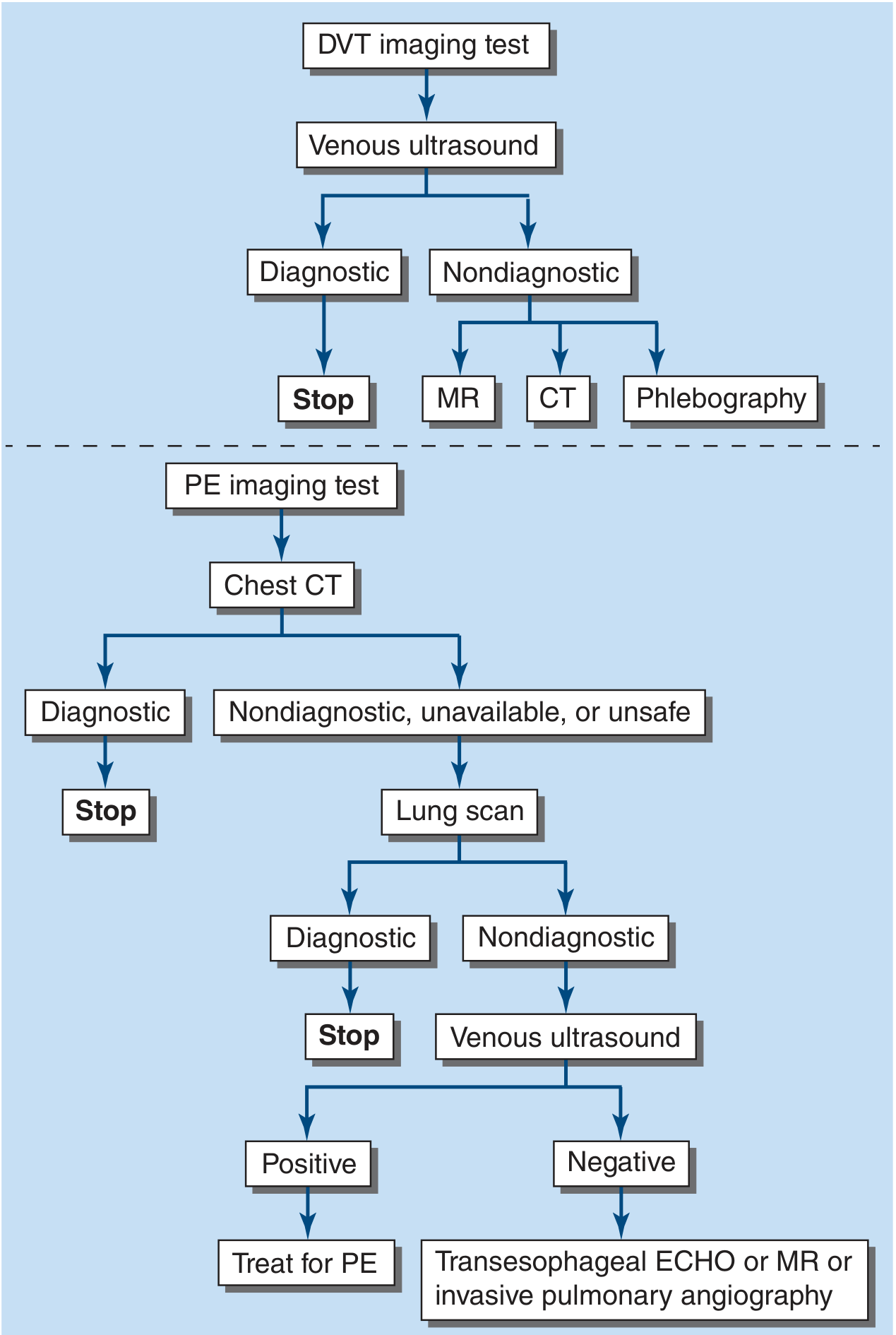
Diagnostic Imaging
First-line imaging is venous ultrasound. If non-diagnostic, proceed to MR venography, CT venography, or phlebography.
Anticoagulation - The Cornerstone of Treatment
Three major strategies exist (Harrison's 22E, pp. 2205-2207):
Strategy 1 - Parenteral then Warfarin ("Bridge")
Parenteral anticoagulation (UFH, LMWH, or fondaparinux) bridged to warfarin. This is the traditional approach (increasingly less used).
Strategy 2 - Parenteral then DOAC
5 days of parenteral anticoagulation, then switch to:
- Dabigatran 150 mg twice daily (CrCl >30 mL/min); 75 mg BID if CrCl 15-30 mL/min
- Edoxaban 60 mg once daily (normal renal function, weight >60 kg, no potent P-gp inhibitors); reduce to 30 mg OD if CrCl 15-50 mL/min, weight ≤60 kg, or P-gp inhibitors
Strategy 3 - Oral Monotherapy (preferred for most patients)
- Rivaroxaban: 15 mg twice daily for 3 weeks, then 20 mg once daily with dinner. (CrCl 15-50: 10 mg BID)
- Apixaban: 10 mg twice daily for 1 week, then 5 mg twice daily. Reduce to 2.5 mg BID if ≥2 of: age >80, weight <60 kg, creatinine >1.5 mg/dL
Parenteral Agents - Dosing Details
| Agent | Dose |
|---|---|
| UFH (IV) | Bolus 60 U/kg, then 18 U/kg/h; titrate to aPTT 60-80 s (or anti-Xa 0.3-0.7 U/mL) |
| Enoxaparin (LMWH) | 1 mg/kg SC twice daily OR 1.5 mg/kg SC once daily (adults) |
| Dalteparin | 200 U/kg once daily OR 100 U/kg twice daily |
| Tinzaparin | 175 U/kg once daily |
| Fondaparinux | Weight-based SC once daily; adjust for renal impairment |
HIT: If heparin-induced thrombocytopenia is suspected/confirmed, use argatroban (IV, hepatically metabolized), bivalirudin (IV, renally metabolized), or fondaparinux.
LMWH monitoring: Routine monitoring not needed. Check anti-Xa 4h post-dose (target 0.5-1 U/mL for BID dosing) in obesity, pregnancy, or CKD.
Duration of Anticoagulation
| Clinical Scenario | Duration |
|---|---|
| First provoked DVT (transient risk factor, e.g., surgery) | 3 months |
| First unprovoked proximal DVT | Minimum 3 months; consider extended therapy |
| Recurrent DVT or ongoing risk factors (cancer, thrombophilia) | Extended (indefinite) |
| Cancer-associated DVT | LMWH or DOAC preferred; indefinite duration while cancer active |
| Isolated distal (calf) DVT | Variable - 3 months or serial surveillance if no extension |
After completing initial treatment, the decision to continue must balance the annual risk of recurrence (~8% after provoked, ~25% after unprovoked DVT) against the annual major bleeding risk (~1-3% on anticoagulation).
Special Situations
Isolated Calf DVT
The GARFIELD-VTE Registry (2145 patients with isolated calf DVT vs 3846 proximal DVT) found that calf DVT patients were more likely to have had surgery or leg trauma, and less likely to have cancer or prior VTE. Nearly half received anticoagulation for at least 1 year. Anticoagulation vs. serial surveillance is an individualized decision. - Harrison's 22E, p. 2205
Upper Extremity DVT (PICC-related)
Rate can be reduced by: judicious PICC selection, single-lumen rather than multi-lumen PICCs, and smallest possible lumen size (4 Fr preferred over 5-6 Fr). Treat with anticoagulation similarly to lower extremity DVT.
Cancer-Associated DVT
LMWH has historically been standard; DOACs (especially edoxaban and rivaroxaban) are now acceptable alternatives, with the caveat that they carry higher GI/GU bleeding risk in certain cancer types (e.g., GI malignancies).
Pregnancy
DOACs are contraindicated. LMWH (weight-adjusted) is the agent of choice throughout pregnancy and postpartum. Warfarin is teratogenic in the first trimester and can cause fetal bleeding.
HIT (Heparin-Induced Thrombocytopenia)
Stop all heparin products immediately. Switch to argatroban, bivalirudin, or fondaparinux. Do not use warfarin until platelet count has recovered (warfarin can cause limb gangrene via protein C/S depletion in acute HIT).
Advanced Therapy Beyond Anticoagulation
Catheter-Directed Thrombolysis (CDT)
The ATTRACT trial (692 patients with femoral or iliofemoral DVT) randomized patients to CDT plus anticoagulation vs. anticoagulation alone. At 2 years, there was no overall reduction in post-thrombotic syndrome in the thrombolysis group. A trend toward benefit was seen in iliofemoral DVT subgroup (not femoral alone). CDT is therefore not routinely recommended but may be considered in selected patients with extensive iliofemoral DVT and low bleeding risk. - Harrison's 22E, p. 2205
A 2025 ESVM Practice Guideline (PMID 40587333) covers updated interventional treatment of VTE.
IVC Filters
Reserved for patients with documented DVT/PE who have absolute contraindications to anticoagulation (e.g., active major bleeding). Retrievable filters preferred. Filters do not treat DVT and do not replace anticoagulation once bleeding resolves.
Compression Stockings
For symptomatic swelling at DVT diagnosis: graduated compression stockings (30-40 mmHg or 20-30 mmHg) may be prescribed for patient comfort. Replace every 3-6 months (lose elasticity). However, prescribing compression stockings to asymptomatic newly diagnosed acute DVT patients does NOT prevent post-thrombotic syndrome. - Harrison's 22E, p. 2205
DVT Prophylaxis (In-Hospital)
All ICU and high-risk patients should receive prophylaxis if feasible:
- Pharmacologic: Low-dose UFH (5000 U SC BID/TID) or LMWH (enoxaparin 40 mg SC OD). LMWH is more effective in high-risk patients (e.g., post-orthopedic surgery) and has lower HIT risk.
- Mechanical: Sequential compression devices (SCDs) for patients with high bleeding risk.
- For renal dysfunction: LMWH use is limited; UFH or SCDs preferred.
Computerized reminder systems have been shown to increase prophylaxis use and reduce symptomatic VTE rates.
Post-Thrombotic Syndrome (PTS)
PTS occurs in 20-50% of patients after proximal DVT. Characterized by chronic leg pain, swelling, heaviness, and in severe cases venous ulceration. Adequate anticoagulation during acute DVT reduces clot propagation and recurrence, which reduces PTS risk. Graduated compression can help symptoms once PTS develops.
When DOACs Are NOT Standard Treatment
A 2024 JACC State-of-the-Art Review (PMID 38233019) outlines specific situations where DOACs should not be the default:
- Antiphospholipid Antibody Syndrome (APS) - Warfarin remains preferred, especially triple-positive APS
- Mechanical heart valves - DOACs are contraindicated
- Severe renal impairment (CrCl <15 mL/min) - Most DOACs not studied/approved
- Pregnancy - DOACs contraindicated
- Certain GI/GU malignancies - Higher bleeding risk with some DOACs
- Morbid obesity (BMI >40 or weight >120 kg) - LMWH or anti-Xa-monitored DOAC preferred
Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapter 290, pp. 2205-2208 | Harriet Lane Handbook, 23rd Edition (enoxaparin dosing)
This is a shared conversation. Sign in to Orris to start your own chat.