definition, etiology,risk factors, symptoms, diagnosis, management of femoral, umbilical and paraumbilical hernias
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed. Here is a comprehensive, well-structured answer:
Femoral, Umbilical, and Paraumbilical Hernias
PART 1 — FEMORAL HERNIA
Definition
A femoral hernia is a protrusion of extraperitoneal tissue, peritoneum, and sometimes abdominal contents through the femoral canal — the small space just medial to the femoral vein below the inguinal ligament. The hernia exits through the saphenous opening (1½ inches below and lateral to the pubic tubercle), then expands in the loose areolar tissue, giving it a characteristic retort shape with a bulbous extremity that may curl upward above the inguinal ligament.
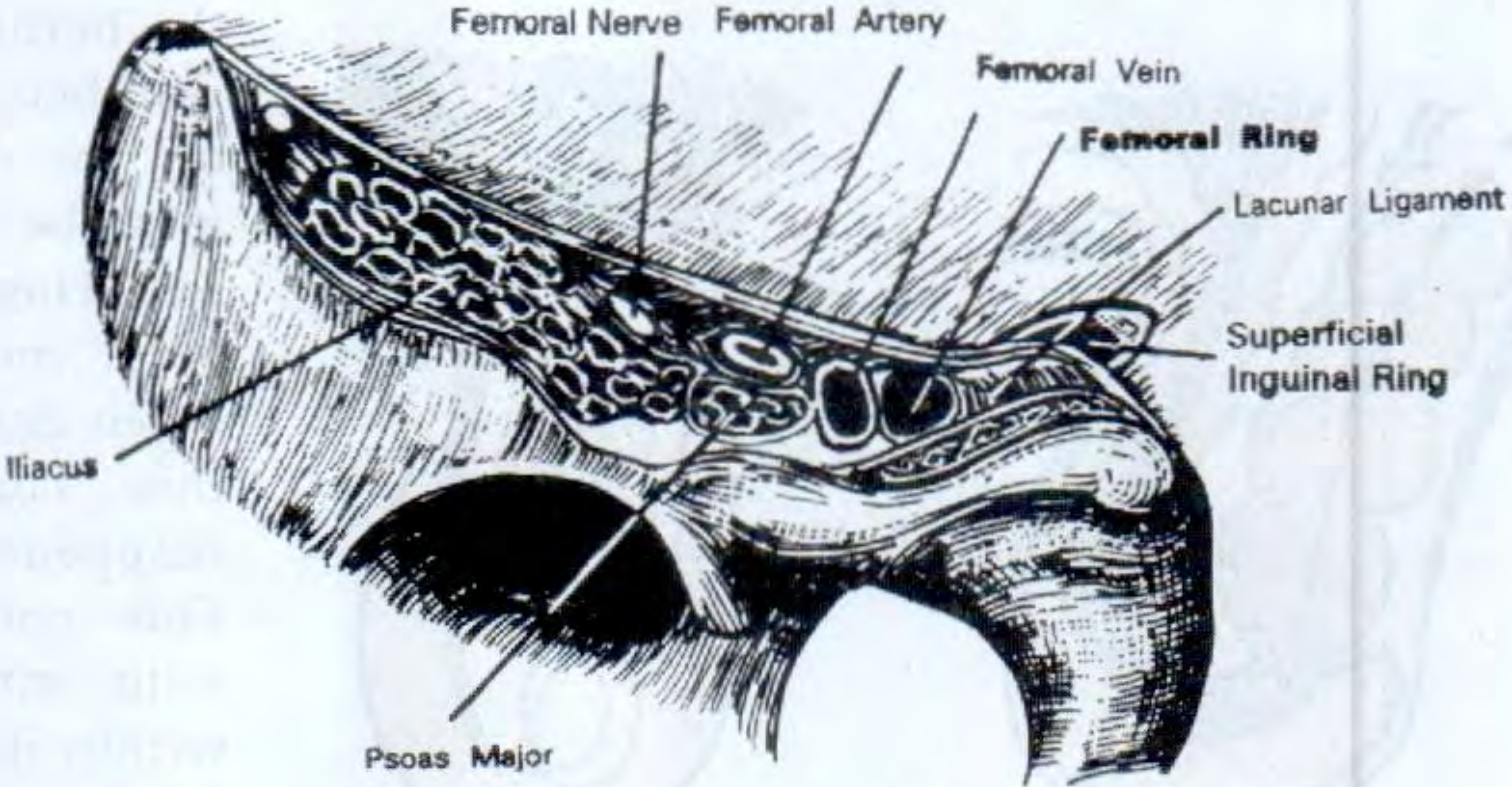
Boundaries of the femoral canal:
| Wall | Structure |
|---|---|
| Anterior/superior | Inguinal ligament |
| Posterior/inferior | Pubic ramus + pectineus muscle (iliopectineal/Astley Cooper's ligament) |
| Medial | Lacunar (Gimbernat's) ligament — sharp, unyielding edge |
| Lateral | Femoral vein |
Etiology & Risk Factors
- Female sex — the female pelvis is wider, enlarging the femoral canal (femoral hernia is 2× more common in women; female:male ≈ 2:1). However, inguinal hernia remains the commonest groin hernia even in women.
- Age — rare before 20 years; incidence rises steadily and peaks over 50 years; elderly thin women are most commonly affected.
- Right side affected twice as frequently as the left; bilateral in 20% of cases.
- The rigid bony/ligamentous ring means this hernia strangulates very frequently.
Symptoms
- Swelling in the groin below and lateral to the pubic tubercle (symptoms are generally less pronounced than inguinal hernia)
- Pain and discomfort in the groin
- Symptoms of intestinal obstruction (colicky abdominal pain, vomiting, constipation) — because 50% present as an emergency with strangulation
- The hernia may be as small as 1–2 cm and easily missed
Diagnosis
Clinical:
- Swelling appears below and lateral to the pubic tubercle, below the inguinal ligament
- In late stages, the bulbous extremity may extend above the inguinal ligament, mimicking a direct inguinal hernia
- Cough impulse palpable at the saphenous opening (~4 cm below and lateral to the pubic tubercle)
- Invagination test: inguinal canal is empty — no hernia felt in the inguinal canal
- The hernia rapidly becomes irreducible and loses its cough impulse due to the tight neck
Key differentiating features from inguinal hernia:
- Lies lateral to pubic tubercle and below inguinal ligament (inguinal hernia is medial and above)
- Pressure over the femoral canal/saphenous opening controls a femoral hernia; pressure over the deep inguinal ring stops indirect inguinal hernia
Differential diagnosis:
- Saphena varix — disappears on lying down; fluid thrill (not expansile impulse); Schwartz's test positive
- Enlarged inguinal lymph nodes (especially the node of Cloquet within the femoral canal)
- Psoas abscess — cold abscess tracking from Pott's disease; lateral to femoral vessels
- Femoral artery aneurysm — expansile pulsation
- Psoas bursa — cystic, diminishes with hip flexion
- Lipoma
- Ruptured adductor longus with haematoma
Investigations:
- Routine elective cases: no specific investigations needed
- Uncertainty: ultrasound or CT scan
- Emergency (obstruction): plain abdominal X-ray (dilated bowel loops); CT to exclude malignancy and identify the hernia
- Any unexplained small bowel obstruction → careful examination for femoral hernia
Management
Surgery is mandatory — there is no conservative option. Due to the high strangulation risk, all femoral hernias should be treated urgently.
1. Low approach — Lockwood
- Simplest; suitable only when bowel resection is not anticipated
- Can be done under local anaesthesia
- Transverse incision over the hernia; sac contents reduced; sac reduced; inguinal ligament sutured to pectineal ligament
- Mesh plug may be placed for reinforcement
- Limitation: cannot perform bowel resection (anastomosis cannot be returned through the narrow canal)
2. Inguinal approach — Lotheissen
- Incision identical to Bassini/Lichtenstein; opens inguinal canal; mobilises spermatic cord; incises transversalis fascia into extraperitoneal space
- Hernia reduced by pulling from above and pushing from below; peritoneum can be opened if needed
- Defect closed with sutures, mesh plug, or flat mesh in preperitoneal plane
- Surgeon may also place inguinal mesh to protect against concomitant inguinal hernia
3. High (preperitoneal) approach — McEvedy / Nyhus modification
- Indicated when strangulation risk is high and bowel resection may be required
- Transverse incision just above the inguinal canal (Nyhus) → anterior rectus sheath incised → surgeon works in the preperitoneal space
- Bowel can be inspected, resected and anastomosed before being returned
- Can be extended for bilateral repair (Henry's approach)
- Requires regional or general anaesthesia
4. Laparoscopic approach (TEP or TAPP)
- Ideal for elective reducible femoral hernias
- Recommended in women because laparoscopy visualises all hernia orifices, removing diagnostic uncertainty and reducing early recurrence from misdiagnosis
- Increasing reports of TAPP in the emergency setting
PART 2 — UMBILICAL HERNIA
Definition & Classification
Any hernia closely related to the umbilicus. Four varieties:
| Type | Definition |
|---|---|
| Exomphalos | Congenital: abdominal contents in umbilical cord, covered by a diaphanous (transparent) membrane |
| Congenital umbilical hernia | Through the centre of a weak umbilical scar in neonates/infants |
| Acquired umbilical hernia | In adults, through the true umbilical scar; rare compared to paraumbilical |
| Paraumbilical hernia | Most common acquired type; through a defect adjacent to (usually just above) the umbilicus |
Umbilical Hernia in Children (Congenital)
Etiology / Risk Factors
- Failure of the umbilical ring to close normally after cord healing
- Occurs in up to 10% of infants; higher in premature babies
- Black infants affected up to 8× more than white infants
- Sexes equally affected
Symptoms
- Swelling at the umbilicus, prominent on crying
- Classic conical shape on straining
- Usually symptomless
- Obstruction/strangulation extremely uncommon under age 3
Diagnosis
- Clinical: bulge through the centre of the umbilical scar, everts the umbilicus
- Resonant to percussion (small bowel content)
- Easily reducible; spontaneously reduces when child lies down; definite impulse on crying
- Defect size: tip of little finger to 2–3 fingers' breadth
Management
- Conservative under age 2: parental reassurance; 95% resolve spontaneously (the umbilical scar thickens and contracts within 5 years)
- Surgery if persists beyond age 2:
- Curved incision below umbilicus
- Sac neck defined, opened, contents reduced
- Sac closed and redundant sac excised
- Defect closed with interrupted slowly absorbable sutures
Umbilical / Paraumbilical Hernia in Adults
Definition
Conditions that cause stretching of the linea alba (pregnancy, obesity, liver cirrhosis with ascites) predispose to reopening of the umbilical defect. The defect can be through the true umbilicus or in the median raphe immediately adjacent to it — the latter are classically called paraumbilical hernias. Under current guidelines, any hernia in the immediate vicinity of the umbilicus may be termed "umbilical."
Etiology & Risk Factors
- Obesity — most important risk factor
- Pregnancy and postpartum — stretching of the midline raphe
- Liver cirrhosis with ascites — raised intra-abdominal pressure + impaired tissue healing
- Other causes of raised intra-abdominal pressure: bowel distension, ovarian cyst, fibroid
- Paraumbilical hernia is the commonest acquired umbilical hernia; develops in middle and old age; obese women most commonly affected
Symptoms
- Pain (tissue tension or intermittent bowel obstruction symptoms) — main complaint
- Swelling at or adjacent to the umbilicus
- In small hernias, swelling may be imperceptible and pain/discomfort is the dominant complaint
- In large hernias: overlying skin becomes thin, may develop irritation and ulceration
- The hernia is firm when containing omentum; soft and resonant when containing bowel
Diagnosis
- Clinical:
- Bulge typically slightly to one side of the umbilical depression, creating a crescent-shaped umbilicus
- Smooth surface with distinct edge (unless patient is obese)
- Paraumbilical hernia: firm fibrous edge of the linea alba defect palpable when hernia is reduced
- Many paraumbilical hernias are irreducible (contents adherent to sac or narrow neck)
- Women > men affected
- Complications: Because the neck is narrow relative to sac size, they are prone to incarceration, obstruction, and strangulation
Management
Indications for surgery:
- Hernia containing bowel → surgery strongly advised (high strangulation risk)
- Small asymptomatic hernias may be observed but tend to enlarge
- Postpartum women: encourage weight loss and abdominal exercises first; avoid surgery before/during pregnancy
Open repair:
- Defects < 1 cm: simple suture repair, provided no tension
- Defects up to 2 cm — Mayo repair: transverse incision; sac dissected, opened, contents reduced; peritoneum closed; fascial edges closed in overlapping "waistcoat over trousers" fashion with non-absorbable sutures
- Defects > 2 cm: mesh repair is advised (current evidence recommends mesh even for smaller defects given high recurrence without it)
Laparoscopic repair:
- Camera port + two lateral working ports
- Contents reduced by traction and external pressure
- Falciform ligament and median umbilical fold taken down for smooth surface
- Intraperitoneal mesh (non-adherent) introduced and fixed with staples/tacks/sutures
- Preferred in obese patients, those with rectus divarication, and multiple ventral defects
- Fewer wound complications but requires expensive tissue-separating mesh; potential for bowel adhesion/erosion
Special circumstances:
- Cirrhosis (Child's B/C): Very high surgical morbidity/mortality; requires hepatology input; fine continuous fascial sutures to minimise post-op ascites leak; mesh avoided in contaminated field
- Emergency (strangulation): Open surgery preferred; avoid mesh in established strangulation (infection risk); suture repair now with definitive mesh repair later
PART 3 — PARAUMBILICAL HERNIA (Summary)
The paraumbilical hernia is treated as part of the umbilical hernia spectrum above, but key distinguishing points are summarised:
| Feature | Paraumbilical Hernia |
|---|---|
| Site | Just above (occasionally below) the umbilicus, in the linea alba adjacent to — not through — the umbilical scar |
| Who | Middle-aged/older obese women |
| Contents | Omentum (firm) or bowel (soft, resonant) |
| Reducibility | Often irreducible — contents adhere, or neck is narrow |
| Strangulation | Relatively less common than obstruction, but still significant |
| Intermittent pain | Yes — the fibrous, non-yielding linea alba defect causes recurrent pain episodes |
| Repair | Same as adult umbilical hernia (Mayo for ≤2 cm; mesh for >2 cm) |
Quick Comparison Table
| Feature | Femoral | Umbilical (child) | Umbilical/Paraumbilical (adult) |
|---|---|---|---|
| Site | Below inguinal ligament, lateral to pubic tubercle | Centre of umbilical scar | Through/adjacent to umbilical scar |
| Who | Thin, elderly women (>50 yrs) | Infants; premature; Black race | Obese women; cirrhotic patients |
| Strangulation risk | Very high (rigid ring) | Very low | Moderate–high (narrow neck) |
| Spontaneous resolution | No | 95% by age 5 | No |
| Emergency presentation | ~50% | Rare | Uncommon but significant |
| Surgery | Urgent; Lockwood / Lotheissen / McEvedy / Laparoscopic | Elective if persists >2 yrs | Elective (or emergency if strangulated) |
| Mesh | For all open/laparoscopic | Not usually needed | For defects >2 cm (and increasingly for all sizes) |
Sources: Bailey and Love's Short Practice of Surgery, 28th ed.; S Das, A Manual on Clinical Surgery, 13th ed.
This is a shared conversation. Sign in to Orris to start your own chat.