. GERD – Definition, manifestations – Investigations (endoscopy/pH monitoring/manometry) – Complications (stricture/Barrett's/adenocarcinoma) – Homoeopathic therapeutics
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Searching the Web
homeopathic remedies for GERD gastroesophageal reflux disease therapeutics
Finding Sources
Reading Web Page
https://hchomeopathyfoundation.org/a-homeopathic-approach-to…
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from authoritative textbooks. Let me compile the complete, well-structured answer.
Gastroesophageal Reflux Disease (GERD)
1. Definition
GERD is a chronic disorder in which reflux of gastric acid (or bile) from the stomach into the esophagus becomes symptomatic or causes histopathological changes in the upper GI or respiratory tract. It results from an imbalance between the transdiaphragmatic pressure gradient and the valvular mechanism at the esophagogastric junction (EGJ). In the United States, symptomatic heartburn occurs in 10-20% of the population, making GERD one of the most common GI disorders.
- Rosen's Emergency Medicine, 9th ed.
- Sabiston Textbook of Surgery, 21st ed.
Asymptomatic reflux of gastric contents occurs several times daily as a normal physiologic event; it becomes GERD only when it is symptomatic or damages tissues.
Pathophysiology
The primary antireflux mechanism involves five components at the EGJ:
- Lower esophageal sphincter (LES) - a 3-4 cm smooth muscle high-pressure zone
- Crural diaphragm - pinches the esophagus, augmenting LES during inspiration/exertion
- Angle of His - the acute angle between esophagus and gastric fundus
- Gubaroff valve - mucosal thickening acting as a cushion at the EGJ
- Intraabdominal esophageal length - positive abdominal pressure compresses the esophageal wall
GERD occurs via three main mechanisms:
- Increased abdominal pressure (obesity, pregnancy, excessive abdominal training)
- Decreased thoracic pressure (obstructive pulmonary disease)
- Defective valve (hiatal hernia - the most common reason; also transient LES relaxations, generalized LES hypotension)
Drugs that reduce LES pressure: nitrates, calcium channel blockers, anticholinergics, albuterol, opioids, tricyclic antidepressants, anxiolytics, PDE5 inhibitors. Fatty meals and chocolate also reduce LES pressure.
- Sabiston Textbook of Surgery, 21st ed.
2. Clinical Manifestations
Typical (Esophageal) Symptoms
| Symptom | Description |
|---|---|
| Heartburn | Retrosternal burning, worse postprandially, lying flat, bending |
| Regurgitation | Effortless reflux of bitter/sour material into mouth or throat |
| Water brash | Hypersalivation reflex triggered by acid in the esophagus |
| Dysphagia | May indicate peptic stricture or Barrett's-associated carcinoma |
| Odynophagia | Painful swallowing if severe esophagitis present |
Atypical (Extraesophageal) Symptoms
- Respiratory: chronic cough, asthma-like wheeze, aspiration pneumonia, laryngitis (hoarseness), chronic sinusitis
- Ear, nose, throat: posterior laryngitis, globus sensation, subglottic stenosis in infants
- Dental: enamel erosion of palatal surfaces of maxillary teeth, dentinal hypersensitivity (irreversible)
- Cardiac-mimicking: non-cardiac chest pain
Alarm Features (requiring urgent endoscopy)
- Dysphagia / odynophagia
- Unexplained weight loss
- GI bleeding or iron-deficiency anemia
- Vomiting
- Age >55 with new-onset symptoms
3. Investigations
A. Upper GI Endoscopy (EGD)
Endoscopy is the primary investigation but is not required for typical symptoms without alarm features. It is indicated for:
- Alarm symptoms
- Screening of high-risk patients (long-standing GERD, male, >50 years, obese)
- Surveillance for Barrett's esophagus (BE)
Endoscopic findings range from:
- Normal appearance (does not exclude GERD)
- Minimal-change esophagitis: papillary elongation, basal cell hyperplasia, intercellular edema
- Erosive esophagitis (Los Angeles Classification grades A-D): mucosal breaks of increasing severity
- Ulceration and scarring
- Stricture formation (peptic stricture)
- Salmon-pink metaplastic tongues of Barrett's mucosa above the GEJ
Biopsy protocol in GERD:
-
Biopsies should be taken >2 cm above the GEJ to reliably diagnose esophagitis (lower 1-2 cm may show mild changes even in asymptomatic subjects)
-
For Barrett's screening: 4-quadrant biopsies every 2 cm (surveillance for dysplasia); every 1 cm if high-grade dysplasia suspected
-
Histology reveals: basal cell hyperplasia, papillary elongation, epithelial necrosis, intraepithelial eosinophils/neutrophils/lymphocytes, "balloon cells," and surface erosions
-
Clinical Gastrointestinal Endoscopy, 3rd ed.
B. Ambulatory 24-hour pH Monitoring
This is the gold standard for diagnosing GERD, quantifying acid exposure, and correlating symptoms with reflux events.
Methods:
- Transnasal pH catheter (most common): placed 5 cm above the LES (location confirmed by prior manometry); multiple sensors can detect height of reflux; more uncomfortable but cheaper and reliable
- Wireless Bravo capsule: clipped to esophageal mucosa endoscopically; allows 48-96 hour recording; better tolerated; risk of premature detachment or capsule-related chest pain; more expensive; data loss possible due to radio interference
Parameters measured:
- DeMeester score (composite score, normal <14.72)
- % time pH <4 (normal <4% upright, <2% supine, <4.5% total)
- Number of reflux episodes
- Symptom Index (SI) and Symptom Association Probability (SAP)
- Pattern: upright, supine, or combined
Indications (TABLE 83.3, Sabiston):
- Diagnose GERD when symptoms are suggestive
- Evaluate extraesophageal/atypical symptoms
- Assess GERD severity (DeMeester score)
- Pre-operative workup before antireflux surgery
- Post-operative evaluation of persistent symptoms
Important caveat: The pH catheter must be placed precisely 5 cm above the LES - which requires esophageal manometry to localize the LES accurately.
Impedance-pH monitoring: Detects both acid and non-acid (weakly acidic, alkaline/bile) reflux by measuring changes in intraluminal electrical resistance; particularly useful when symptoms persist despite PPI therapy (non-acid reflux).
C. Esophageal Manometry
Measures LES basal pressure, LES length, IRP (integrated relaxation pressure), and esophageal body peristalsis via a transnasal catheter; performed fasting without sedation.
Key points:
- Cannot diagnose GERD - a normal LES does not exclude GERD (abnormal transdiaphragmatic gradient may overcome it), and an abnormal LES is not synonymous with GERD
- Primary role: to localize the LES for precise pH catheter placement; to diagnose coexisting primary esophageal motility disorders (e.g., achalasia, ineffective esophageal motility); to evaluate before and after antireflux surgery
- Classifies EGJ types (I, II, III) based on whether LES and diaphragm pressures are coincident or separated (manometric hiatal hernia)
- Classified by Chicago Classification (v4.0)
Indications:
-
Localizing LES before pH monitoring
-
Evaluating dysphagia
-
Diagnosing primary esophageal motility disorders
-
Pre-operative assessment before antireflux surgery
-
Evaluating symptomatic patients after esophageal surgery
-
Sabiston Textbook of Surgery, 21st ed.
D. Barium Swallow / Upper GI Series
A fluoroscopic study; may demonstrate hiatal hernia, reflux, strictures, or ulcers. Less sensitive than endoscopy for early mucosal disease; useful pre-operatively to evaluate esophageal length and anatomy.
E. Empiric PPI Trial
A 4-8 week trial of a proton pump inhibitor (e.g., omeprazole 20-40 mg daily) with symptomatic relief is widely used as a pragmatic diagnostic approach in low-risk patients with typical symptoms.
4. Complications
A. Peptic (Reflux) Esophageal Stricture
Chronic acid exposure causes transmural inflammation, fibrosis, and scarring of the esophageal wall, leading to a benign peptic stricture - characteristically occurring in the distal esophagus. This presents with progressive dysphagia, initially for solids then liquids. Treatment: dilation (bougie or balloon) combined with PPI therapy to prevent recurrence.
B. Barrett's Esophagus (BE)
Definition: Replacement of the normal stratified squamous epithelium of the esophagus by intestinal metaplasia (columnar epithelium containing goblet cells), endoscopically visible as salmon-pink mucosa extending above the GEJ.
Epidemiology: Occurs in ~10-15% of GERD patients undergoing endoscopy; males > females; typically presents between ages 40-60; more common in Caucasians; associated with central obesity (OR 4.0 for Barrett's).
Diagnosis (ACG/AGA criteria):
- Endoscopic evidence of columnar metaplasia >1 cm above the GEJ (tongues or circumferential reddish mucosa)
- Histological confirmation of intestinal metaplasia (goblet cells on H&E staining - mucin vacuoles impart the "wine goblet" appearance)
- Both components required for diagnosis in North America (UK/Japan: IM not mandatory)
Anatomic landmarks:
- GEJ = most proximal aspect of gastric folds
- Squamocolumnar junction (SCJ/Z-line) = junction of squamous and columnar mucosa
- In BE, the SCJ is displaced proximally above the GEJ
Histopathology on H&E: Goblet cells with distinct mucin vacuoles; transition between esophageal squamous mucosa and metaplastic columnar mucosa visible at the GEJ.
Dysplasia classification: Low-grade dysplasia (LGD) and high-grade dysplasia (HGD) based on cytologic and architectural criteria.
Surveillance:
-
Non-dysplastic BE: endoscopy every 3-5 years
-
LGD: every 6-12 months
-
HGD or intramucosal carcinoma: therapeutic intervention (RFA, endoscopic mucosal resection, or esophagectomy)
-
Robbins & Kumar Basic Pathology, 10th ed.
-
Clinical Gastrointestinal Endoscopy, 3rd ed.
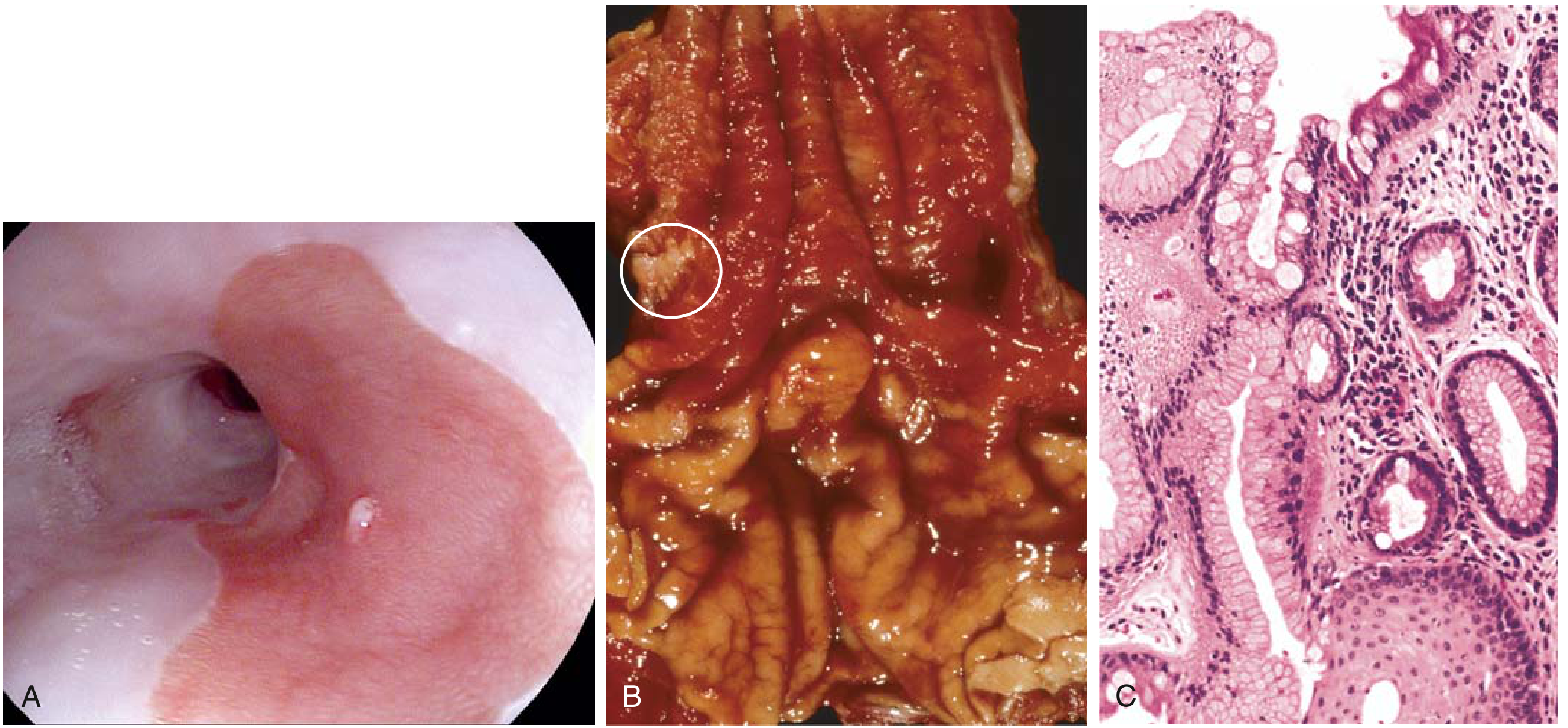
Barrett's esophagus. (A) Endoscopic salmon-pink mucosa. (B) Gross specimen. (C) Histology: goblet cells (metaplastic columnar epithelium) abutting squamous epithelium - Robbins Basic Pathology
C. Esophageal Adenocarcinoma
GERD - Barrett's metaplasia - dysplasia - adenocarcinoma represents a well-characterized stepwise progression.
Epidemiology:
- Adenocarcinoma now accounts for 50% of all esophageal cancers in Western countries (was <5% before 1970)
- 7x more common in men than women; predominantly Caucasian
- Risk factors: documented dysplasia, long-standing GERD, tobacco use, obesity (OR 2.4 men, 2.1 women), previous radiation therapy
- Annual incidence of progression from BE to dysplasia: 0.2-1%
Molecular pathogenesis: Stepwise accumulation of mutations in Barrett's clones - chromosomal abnormalities and TP53 mutations in early stages; subsequent genetic changes drive progression to invasive carcinoma.
Location: Distal third of the esophagus; may invade the gastric cardia.
Morphology:
- Early: flat or raised patches within intact mucosa
- Advanced: large exophytic masses, diffuse infiltration, or deep ulcerating lesions
- Microscopy: mucin-producing glands (back-to-back glands with blue-gray mucin)
Clinical features:
- Progressive dysphagia, odynophagia, weight loss, chest pain, vomiting
- Usually diagnosed at advanced stage (submucosal lymphatic invasion at presentation)
- 5-year survival <25% overall; ~80% if limited to mucosa
Treatment: Surgical resection (esophagectomy), chemoradiotherapy, endoscopic mucosal resection (EMR) for early lesions.
- Robbins & Kumar Basic Pathology, 10th ed.
5. Homoeopathic Therapeutics for GERD
Homoeopathic treatment in GERD is individualized - the remedy is selected based on the totality of symptoms (physical, mental, and constitutional), not just the diagnosis. The following are the most commonly prescribed remedies:
1. Robinia pseudoacacia
The most specific remedy for GERD with intense acidity.
- Keynote: Constant and profuse belching of intensely sour, acrid fluid; "acid fermentation"
- Sour vomiting, especially at night; burning in stomach and esophagus
- Headache from acidity; flatulence
- Worse: lying down at night
- Consider as a primary GERD remedy
2. Nux Vomica
The most frequently used remedy for acid reflux related to lifestyle excess.
- Keynote: GERD from overindulgence in food, alcohol, coffee, or spicy foods; sedentary lifestyle
- Heartburn 1-2 hours after eating; nausea in the morning
- Sour/bitter regurgitation; retching without full vomiting ("feels he could vomit if only he could")
- Waterbrash; sensation of pressure/heaviness in epigastrium
- Constitution: Irritable, impatient, Type A personality, overworked
- Worse: morning, after eating, mental exertion
- Better: after vomiting, rest
3. Iris versicolor
Particularly suited for GERD with profuse acid secretion and involvement of the pancreas/liver.
- Keynote: Burning of the entire GI tract from mouth to anus; "like fire"
- Profuse burning eructations; sour, acrid vomiting that excoriates the mouth and throat
- Frontal headache with GI symptoms; right-sided
- Worse: evenings; periodically (Sunday evenings); during rest
- Better: continued motion
4. Natrum Phosphoricum
The biochemic tissue salt for acid conditions; a first-line biochemic approach.
- Keynote: Neutralizes excess acid; "the acid-antidote"
- Sour belching, sour vomiting, sour-smelling stools
- Regurgitation of sour fluid; creamy yellow coating at the base of the tongue
- Heartburn after eating; waterbrash
- Useful in GERD associated with dyspepsia and worm infestation in children
5. Arsenicum Album
GERD with burning pain and anxiety.
- Keynote: Burning pain in stomach and esophagus, paradoxically better from warm drinks (distinguishes it from Phosphorus)
- Vomiting of food and water; nausea and retching; acrid regurgitation
- Intense thirst for small, frequent sips of water
- Constitution: Anxious, restless, perfectionistic, fastidious; worse midnight-2 AM
- Weakness disproportionate to illness
6. Pulsatilla
GERD from fatty/rich foods; suited to gentle constitutions.
- Keynote: Reflux and heartburn after fatty, rich, or indigestible foods; greasy taste in mouth
- No thirst; symptoms worse in a warm room; better in open air
- Late-evening aggravation; changeable/shifting symptoms
- Constitution: Mild, yielding, emotional, seeks sympathy; women and children
7. Lycopodium clavatum
GERD with bloating, flatulence, and liver/digestive weakness.
- Keynote: Burning heartburn and sour eructations; bloating immediately after eating even small amounts
- Sensation of fullness in upper abdomen; "everything ferments"
- Worse: 4-8 PM; flatulent colic; better after midnight, warm drinks, motion
- Constitution: Intellectual but weak physically; apprehensive; right-sided complaints
8. Phosphorus
GERD with burning that is better from cold drinks (opposite of Arsenicum).
- Vomiting of water/food as soon as it warms in the stomach
- Burning in esophagus and stomach; heartburn
- Waterbrash; thirst for cold water which is vomited when it becomes warm
- Constitution: Tall, slender, open, sympathetic
9. Carbo vegetabilis
GERD with marked flatulence and weakness.
- Burning heartburn; heaviness in stomach; "almost any food causes distress"
- Sour, rancid eructations; tremendous abdominal distension
- Worse: lying down; after eating fatty foods; better from belching
- Useful in elderly or debilitated patients with GERD
10. Calcarea carbonica
Constitutional remedy for GERD in overweight, fair-complexioned individuals.
- Sour eructations; sour vomiting; heartburn; waterbrash
- Craving for indigestible things (chalk, coal, pencil)
- Constitution: Obese, flabby, cold, sweaty; excessive perspiration on the head at night
Biochemic Approach
| Biochemic Salt | Indication |
|---|---|
| Natrum Phosphoricum 6X | Excess acidity, sour belching, yellow tongue coating |
| Natrum Muriaticum 6X | GERD with waterbrash; heartburn with salty taste |
| Kali Phosphoricum 6X | Nervous dyspepsia; GERD from anxiety and stress |
General Management (Integrated Approach in Homoeopathy)
Homoeopathic practitioners typically combine constitutional remedy selection with:
- Dietary modification: Elimination of trigger foods (spicy, fatty, acidic foods, alcohol, caffeine, chocolate); small frequent meals; avoiding meals 2-3 hours before bedtime
- Lifestyle: Head-of-bed elevation; weight loss in obesity; smoking cessation; avoiding tight clothing
- Supplementation: Probiotics to restore gut flora; avoidance of refined carbohydrates
- Classical homoeopathic treatment targets the root cause (constitutional weakness) rather than only suppressing acid
Summary Table
| Remedy | Key Indication |
|---|---|
| Robinia | Intense acidity, sour belching, worse night |
| Nux Vomica | Dietary excess, irritable constitution |
| Iris versicolor | Burning entire GI tract, periodic |
| Natrum Phos | Sour eructations, yellow tongue, biochemic |
| Arsenicum Album | Burning + anxiety, better warm drinks |
| Pulsatilla | Fatty food intolerance, gentle constitution |
| Lycopodium | Bloating, 4-8 PM worse, liver weakness |
| Phosphorus | Better cold drinks, vomiting when warm |
| Carbo veg | Flatulence, debility, elderly |
| Calcarea carb | Obese, sour vomiting, cold constitution |
Sources:
- Rosen's Emergency Medicine, 9th ed. - Rosen's EM
- Sabiston Textbook of Surgery, 21st ed. - Sabiston Surgery
- Clinical Gastrointestinal Endoscopy, 3rd ed. - Clinical GI Endoscopy
- Robbins & Kumar Basic Pathology, 10th ed. - Robbins Pathology
- Yamada's Textbook of Gastroenterology, 7th ed. - Yamada GI
- Homoeopathic therapeutics synthesized from classical materia medica (Boericke, Clarke) and contemporary homoeopathic practice resources
This is a shared conversation. Sign in to Orris to start your own chat.