Stages of shock physiology
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Now I have comprehensive content from multiple authoritative textbooks. Here is a complete synthesis:
Stages of Shock Physiology
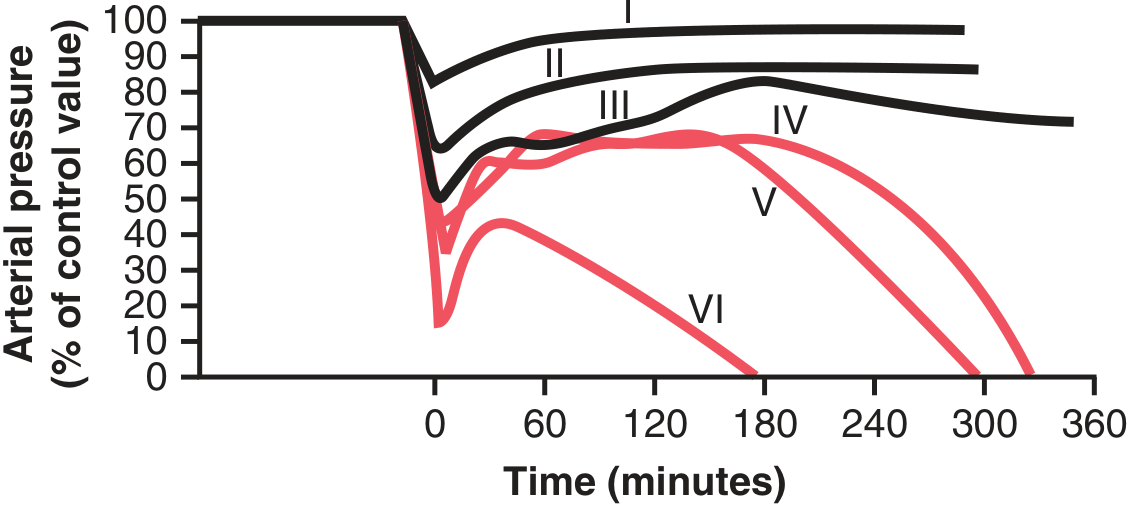
Shock is a progressive disorder of inadequate tissue perfusion and oxygen delivery. Unless the insult is immediately lethal, it evolves through three general stages, best characterized in hypovolemic shock but applicable to all types.
Stage 1 — Nonprogressive (Compensated) Shock
The body's neurohumoral mechanisms are activated to maintain cardiac output and blood pressure. At this stage there is no overt organ dysfunction, though laboratory values may show mild creatinine elevation or lactate rise.
Compensatory mechanisms activated:
| Mechanism | Effect | Time to activation |
|---|---|---|
| Baroreceptor reflex | Sympathetic activation → ↑HR, vasoconstriction | Seconds |
| CNS ischemic response | Intense sympathetic outflow (triggered when MAP <50 mmHg) | Seconds–minutes |
| Catecholamines (adrenal medulla) | ↑HR, peripheral vasoconstriction, venoconstriction | 30 seconds |
| Renin-angiotensin-aldosterone | Arteriolar constriction, Na⁺/water retention | 10–60 min |
| ADH (vasopressin) | Arteriolar and venous constriction, renal water retention | 10–60 min |
| Reverse stress-relaxation | Blood vessels contract around reduced volume | 10–60 min |
| Fluid shifts | Interstitial → intravascular reabsorption, ↑thirst | 1–48 hrs |
Net effect: Tachycardia, peripheral vasoconstriction, renal fluid conservation. Blood is shunted away from skin, gut, and kidneys toward the heart and brain (which are less sensitive to sympathetic constriction).
Clinical sign: Cool, pale, clammy skin. Exception: Early septic shock causes cutaneous vasodilation → warm, flushed skin.
Guyton & Hall: Sympathetic reflexes extend the tolerable blood loss from ~15–20% (without reflexes) to ~30–40% of blood volume before death.
Stage 2 — Progressive Shock
When the underlying insult is not corrected and compensatory mechanisms are overwhelmed, a vicious cycle of cardiovascular deterioration begins. Key positive feedback loops drive the condition toward irreversibility.
The Positive Feedback Cascade
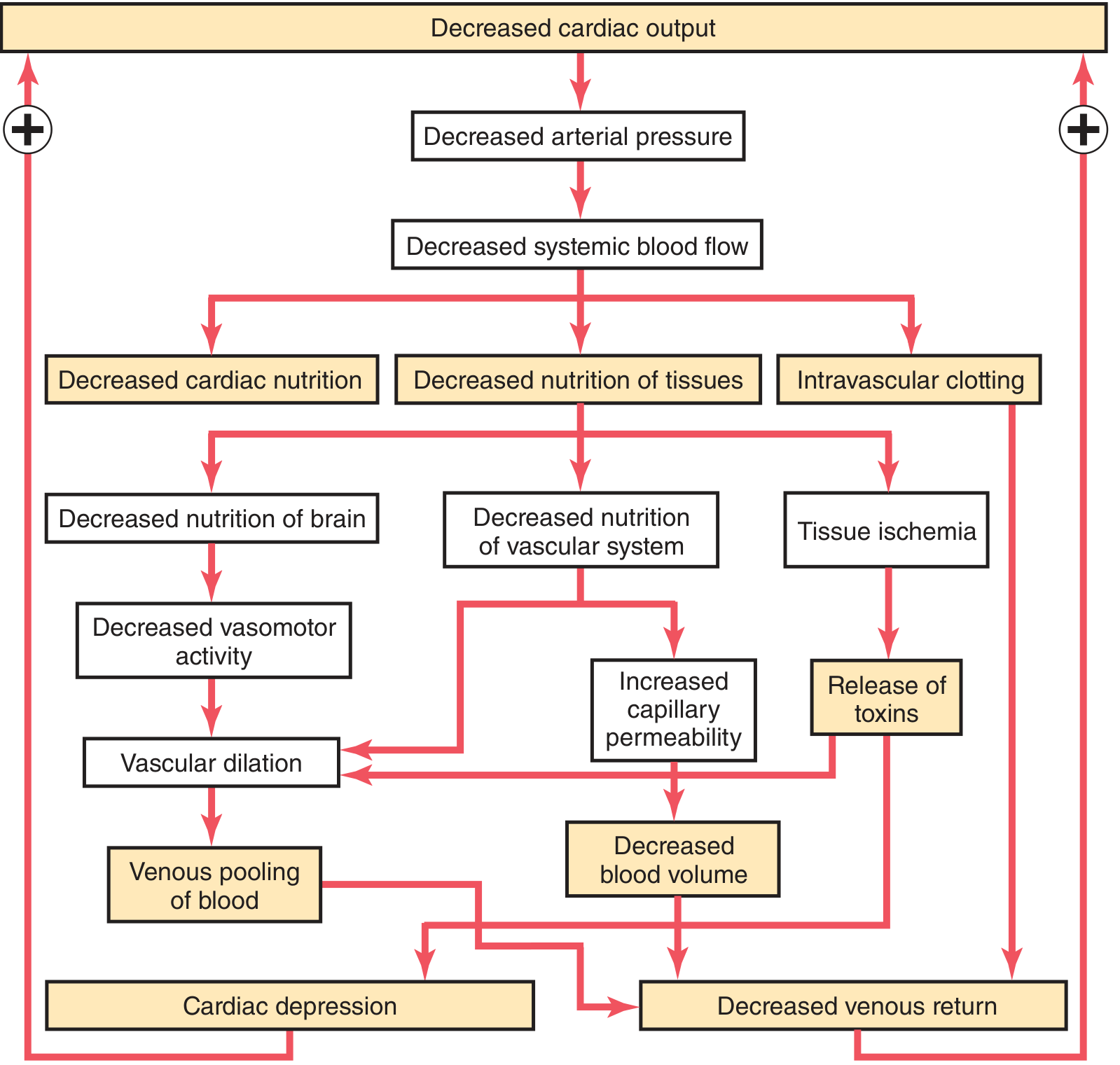
Key pathophysiological events:
-
Anaerobic glycolysis & lactic acidosis
- Persistent O₂ deficit → aerobic respiration fails → lactic acid accumulates
- Lactic acidosis lowers tissue pH → arteriolar vasomotor response is blunted → vasodilation and blood pooling in microcirculation
-
Cardiac depression
- ↓Coronary perfusion → myocardial ischemia → ↓contractility → ↓CO → further ↓coronary flow
- Guyton & Hall: Little cardiac deterioration in first ~2 hrs; by 4 hrs, ~40% deterioration; then rapid complete deterioration
-
Vasomotor failure
- Prolonged hypoperfusion of the vasomotor center in the brainstem → loss of sympathetic tone → further vascular dilation → venous pooling
-
Microvascular sludging & DIC
- Sluggish flow + acidosis → blood cell agglutination → microthrombi → ↑capillary resistance
- Endothelial ischemic injury triggers disseminated intravascular coagulation (DIC)
-
Increased capillary permeability
- Prolonged capillary hypoxia → fluid transudes into interstitium → further ↓blood volume
-
Release of inflammatory mediators
- Ischemic tissues release histamine, serotonin, cytokines (TNF, IL-1, IL-6), and lysosomal enzymes
- Endotoxin absorption from ischemic gut causes further cardiac depression (particularly in septic shock)
-
Generalized cellular deterioration
- Na⁺/K⁺-ATPase pump fails → intracellular Na⁺ and water accumulate → cell swelling
- Mitochondrial dysfunction → ↓ATP production
- Lysosomal membranes break down → autolysis begins
Stage 3 — Irreversible Shock
Cellular and tissue injury is so widespread that survival is not possible even if hemodynamic parameters are temporarily restored.
Hallmarks of irreversibility:
- ATP depletion: Creatine phosphate and ATP are nearly completely degraded. Adenosine diffuses out of cells and is converted to uric acid, which cannot re-enter cells. New ATP synthesis proceeds at only ~2%/hr — insufficient to restore function.
- Lysosomal enzyme leakage → autocatalytic cell destruction
- Myocardial contractile failure progresses (worsened by ↑NO synthesis in sepsis)
- Bacterial translocation: Ischemic bowel allows intestinal flora to enter the bloodstream → superimposed bacteremic/septic shock
- Multi-organ failure: Kidneys (acute tubular necrosis), lungs ("shock lung" — diffuse alveolar damage), liver (centrilobular necrosis), brain, adrenals
- Death follows despite aggressive resuscitation
Hemorrhagic Shock Classification (ATLS)
For clinical staging of hemorrhagic shock, the ATLS classification is used alongside the three physiological stages:
| Class | Blood Loss | BP | HR | Urine output | Mental status |
|---|---|---|---|---|---|
| I | <750 mL (<15%) | Normal | <100 | >30 mL/h | Slightly anxious |
| II | 750–1500 mL (15–30%) | Normal | >100 | 20–30 mL/h | Mildly anxious |
| III | 1500–2000 mL (30–40%) | ↓ | >120 | 5–15 mL/h | Anxious, confused |
| IV | >2000 mL (>40%) | ↓ | >140 | Negligible | Confused, lethargic |
— Schwartz's Principles of Surgery, 11th ed.
Organ Morphology in Shock
| Organ | Finding |
|---|---|
| Kidney | Acute tubular necrosis; fibrin thrombi in glomeruli |
| Liver | Centrilobular (perivenular) necrosis |
| Lung | "Shock lung" = diffuse alveolar damage (esp. sepsis/trauma) |
| Adrenals | Cortical lipid depletion (↑steroid utilization) |
| GI tract | Mucosal ischemia → bacterial translocation |
| Brain/Heart | Neuronal and cardiomyocyte loss (irreversible) |
Note: Most affected tissues recover fully if the patient survives, except neurons and cardiomyocytes.
Key Clinical Markers of Shock Progression
- Serum lactate: Rises with anaerobic metabolism; normalizes with adequate resuscitation
- Base deficit: >8 mmol/L implies ongoing cellular shock
- Urine output: Best early marker of renal perfusion; target >0.5 mL/kg/hr
- ScvO₂/SvO₂: Reflects oxygen extraction; low values indicate inadequate oxygen delivery
Sources:
- Robbins & Kumar Basic Pathology (Robbins Pathology), p. 75
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 120
- Guyton and Hall Textbook of Medical Physiology, Ch. 24
- Harrison's Principles of Internal Medicine, 22E (2025), p. 2355
- Schwartz's Principles of Surgery, 11th ed., p. 220
This is a shared conversation. Sign in to Orris to start your own chat.