What happens to pupils in general anaesthesia
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Here is a comprehensive overview of what happens to pupils during general anaesthesia.
Pupils in General Anaesthesia
Pupil changes are one of the classic clinical signs used to monitor depth of anaesthesia. The response depends on the stage/depth of anaesthesia, the agents used, and whether opioids are part of the regimen.
Guedel's Stages — Pupil Changes by Depth
The traditional framework comes from Guedel's classification of anaesthetic depth (originally described for ether, still conceptually applicable):
| Stage | Level | Pupil finding |
|---|---|---|
| I | Analgesia | Normal / slightly dilated |
| II | Excitement | Dilated (mydriasis), irregular eye movements |
| III (planes 1–4) | Surgical anaesthesia | Progressive changes: early miosis → mid-dilation → fixed dilation in deep planes |
| IV | Medullary depression | Maximally dilated, fixed — sign of impending cardiovascular collapse |
Stage III is divided into four planes based on ocular movements, eye reflexes, and pupil size. At light surgical depths the pupils are moderately constricted; as depth increases into the deeper planes they dilate again. Stage IV dilation with a fixed, unreactive pupil is a critical warning sign. — Katzung's Basic and Clinical Pharmacology, 16th Ed.
Effect of Specific Agents
Volatile Anaesthetics (Isoflurane, Sevoflurane, Desflurane)
- At moderate surgical depth: pupils are mid-position or slightly constricted.
- Pupil size and the pupillary light reflex are used as clinical endpoints to titrate depth, alongside other brainstem signs (respiration, lacrimation, laryngeal reflexes). — Miller's Anesthesia, 10th Ed.
Opioids (Morphine, Fentanyl, Remifentanil)
- Cause miosis (pupil constriction) — this is their characteristic and well-known pupillary effect.
- Mechanism: Mu-opioid receptor agonists block GABAergic inhibitory interneurons that normally suppress the Edinger-Westphal (EW) nucleus. With inhibition removed, the EW nucleus increases parasympathetic outflow via the ciliary ganglion → sphincter pupillae contracts → miosis.
- Opioids also block pupillary reflex dilation in response to nociceptive stimulation during anaesthesia — this is clinically useful as a sign of adequate analgesia.
- At very high doses or in the event of asphyxia/hypoxia, miosis reverses to mydriasis. — Goodman & Gilman's Pharmacological Basis of Therapeutics
Ketamine
- Causes sympathetic stimulation → pupil dilation (mydriasis) and nystagmus.
Atropine / Anticholinergics (used for premedication or bradycardia)
- Block the muscarinic parasympathetic pathway → mydriasis.
The Neural Pathway Behind Pupil Control in Anaesthesia
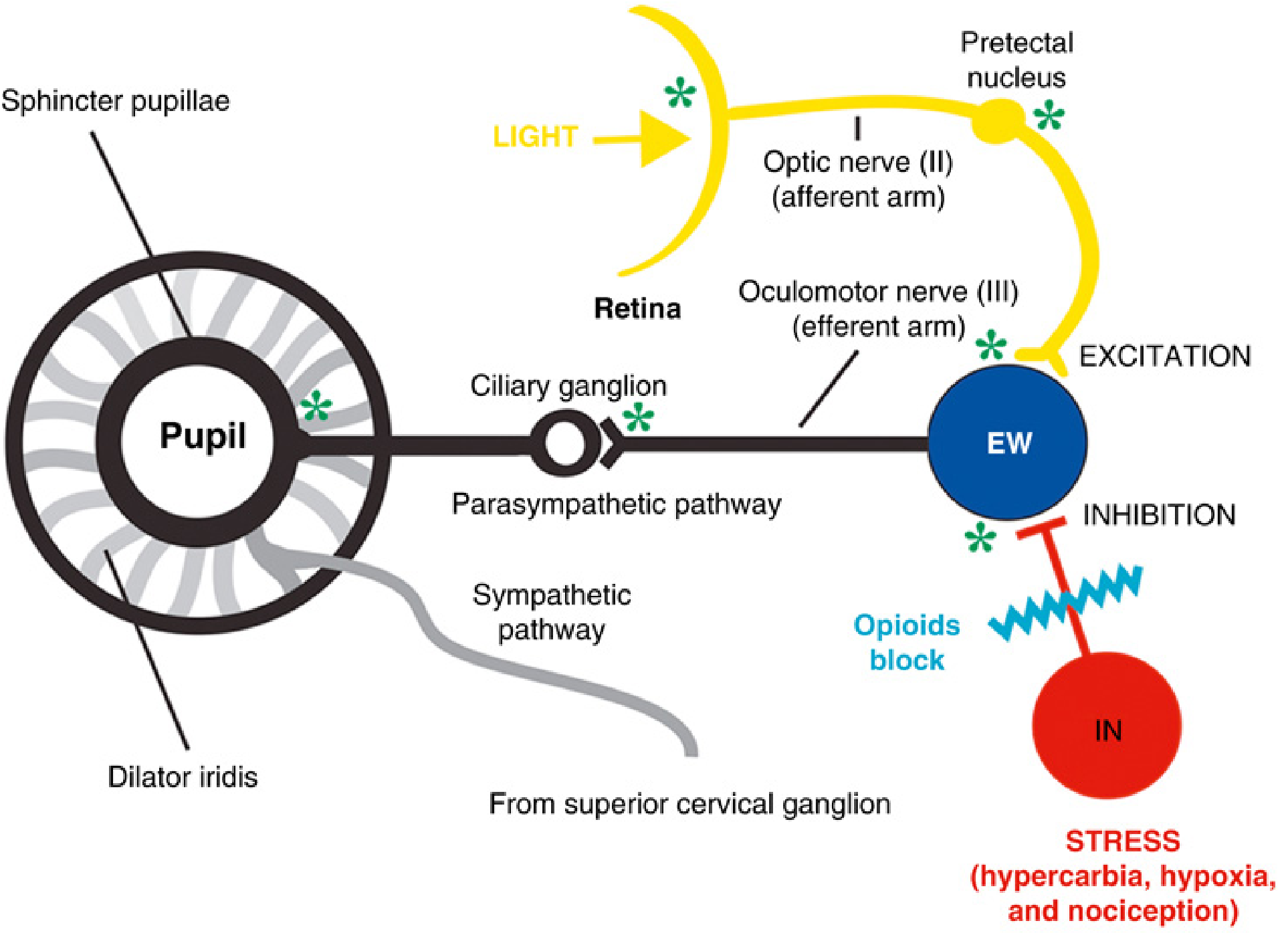
Fig. 22.14 — Miller's Anesthesia, 10th Ed. The EW nucleus neurons are pacemaker cells modified by excitatory (light reflex via optic nerve) and inhibitory inputs (GABAergic interneurons driven by nociception/stress). Opioids block the inhibitory interneuron, disinhibiting the EW nucleus and driving parasympathetic-mediated constriction. Hypercarbia, hypoxia, and nociception all stimulate the inhibitory interneuron and would tend to cause dilation.
Clinical Relevance
- Dilated, fixed pupils during anaesthesia suggest excessive depth (Stage IV), hypoxia, or use of atropine/ketamine.
- Pinpoint pupils suggest opioid excess or very deep opioid-based anaesthesia.
- Pupillary dilation in response to a surgical stimulus (pupillary reflex dilation) indicates inadequate analgesia — a useful monitor especially when neuromuscular blocking agents prevent somatic movement responses.
- Modern multimodal anaesthesia using neuromuscular blockade has made pupillary signs less reliable as sole indicators of consciousness, but they remain valuable as part of a composite assessment. — Miller's Anesthesia, 10th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.