Leukoplakia
Reading File
Finding Sources
Searching PubMed
leukoplakia oral AND malignant transformation
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
I now have enough content for a comprehensive answer. Let me compile everything.
Leukoplakia
Definition
Leukoplakia is a white patch or plaque on the oral mucosa that cannot be characterized clinically or pathologically as any other disease entity. It is an exclusionary, clinical diagnosis - not a histopathological one. Other recognizable causes of white oral lesions (candidiasis, lichen planus, leukoedema, white sponge nevus, hairy leukoplakia) must be ruled out before the diagnosis is applied.
It is the most common premalignant oral mucosal lesion, though the majority of cases remain benign.
- Cummings Otolaryngology Head and Neck Surgery, p. 1578
- K.J. Lee's Essential Otolaryngology, p. 67
Epidemiology
- Prevalence is approximately 1-2% in the US, up to 4.9% in India among adults over 15
- Most common in middle-aged and older men; uncommon under age 30; rises to ~30% in men over 80
- Rates are significantly higher where betel (areca) nut use is common
- 73-81% of affected patients have a history of tobacco use
Etiology and Risk Factors
The exact cause is unknown, but strongly associated habits include:
| Risk Factor | Notes |
|---|---|
| Tobacco (smoked and smokeless) | Single strongest association |
| Areca (betel) nut | With or without tobacco; important in South/Southeast Asia |
| Alcohol | Synergistic with tobacco |
| Chronic sun exposure | Particularly the lower lip (actinic cheilitis) |
| Sanguinaria (herbal extract in some mouthwashes) | Labial alveolar mucosa; reverses on withdrawal |
| Trauma/friction | Causes frictional keratosis - technically not true leukoplakia |
| Genetic disorders | Dyskeratosis congenita, Fanconi anemia (high-risk progression) |
- Cummings Otolaryngology, p. 1579; Goldman-Cecil Medicine, p. 4442
Clinical Features
The appearance is widely variable, ranging from thin translucent patches to thick opaque plaques:
| Type | Description | Risk |
|---|---|---|
| Homogeneous | Uniform white, smooth or finely textured, well-defined | Lower |
| Heterogeneous/speckled | Mixed white-red (erythroleukoplakia); irregular surface | Higher |
| Nodular | Small polypoid outgrowths | Higher |
| Verrucous/exophytic | Warty, projecting surface | Higher |
| Erosive/ulcerative | Surface breakdown present | Higher - rebiopsy mandatory |
Common sites (in descending frequency): lip vermilion > buccal mucosa > mandibular gingiva > tongue > floor of mouth > hard palate > maxillary gingiva > soft palate.
High-risk anatomical sites include the floor of mouth, ventral/lateral tongue, and retromolar trigone/soft palate complex - these carry greater dysplasia and malignancy risk.
- Cummings Otolaryngology, p. 1579-1580; K.J. Lee's Essential Otolaryngology, p. 71-72
Clinical Images
Hairy leukoplakia (EBV-associated, HIV/immunocompromised) on the tongue:

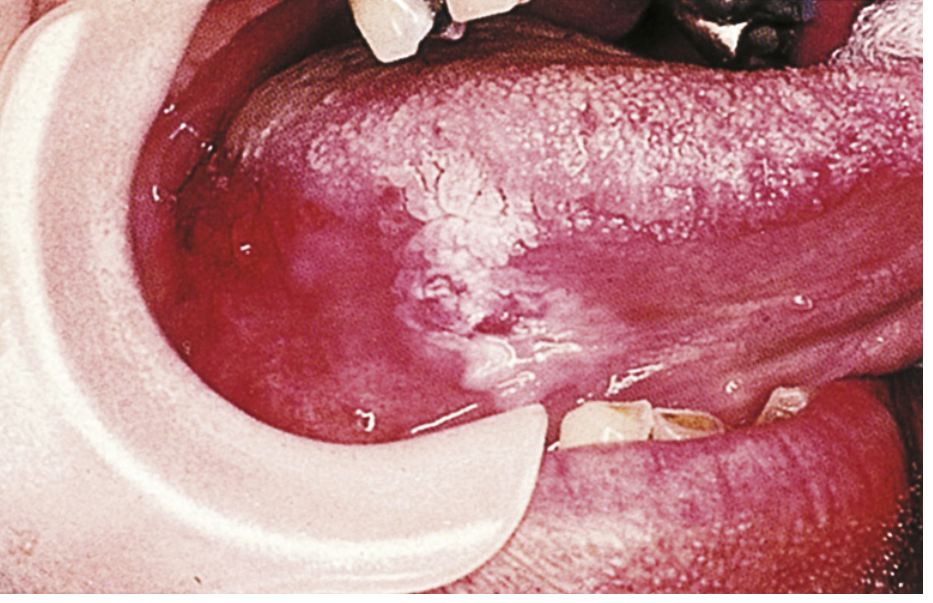
Oral leukoplakia with associated squamous cell carcinoma:
Histopathology
The spectrum of microscopic findings ranges from benign to malignant:
- Hyperkeratosis and acanthosis (no dysplasia) - most common finding
- Mild dysplasia - cytologic atypia confined to the lower epithelial strata
- Moderate dysplasia - several layers of atypical cells; upper half still normal
- Severe dysplasia / carcinoma in situ - full-thickness atypia without invasion
- Invasive squamous cell carcinoma (SCC)
Specific dysplasia features include: drop-shaped epithelial ridges, basal cell hyperplasia, irregular stratification, abnormal mitoses, individual cell keratinization (dyskeratosis), cellular pleomorphism, altered nuclear-to-cytoplasmic ratio, loss of intercellular adhesion, and loss of basal layer polarity.
Dysplasia is found in 3.7% to 28.7% of leukoplakia cases (some series up to 17-25%).
- Cummings Otolaryngology, p. 1580
Malignant Transformation Risk
-
Overall risk of malignant transformation: 0.13% to 17.5% (varies by series and lesion type)
-
Proliferative verrucous leukoplakia (PVL) transforms to SCC in 70-87% of cases
-
Risk is higher with:
- Heterogeneous, speckled, or nodular appearance
- Floor of mouth / ventral tongue location
- Female sex (for PVL)
- Loss of heterozygosity at chromosomal loci 3p and 9p: 3-8x risk; additional losses at 4p, 8p, 11q, 17p: 33-fold increased risk
-
Cummings Otolaryngology, p. 1790; K.J. Lee, p. 75
Proliferative Verrucous Leukoplakia (PVL)
A distinct, aggressive variant:
- More common in women and in patients without usual risk factors
- Occurs in areas less commonly affected by oral SCC
- Multifocal, persistent, high recurrence rate
- No demonstrated HPV association
- Progression: thin flat white patch → leathery thickened plaque → papillary/verrucous → verrucous carcinoma or SCC
- SCC develops in up to 74-87% of cases
Hairy Leukoplakia (Separate Entity)
Caused by Epstein-Barr virus (EBV), occurring in immunocompromised patients (HIV, transplant, cancer therapy, advanced age).
-
White, confluent, "fluffy" (hairy) hyperkeratotic patches on the lateral border of the tongue
-
Cannot be scraped off (unlike thrush)
-
Histology: hyperparakeratosis, acanthosis, "balloon cells" in upper spinous layer
-
In HIV: median time to AIDS onset ~24 months; median time to death ~41 months (pre-HAART)
-
Treatment: HAART (primary); acyclovir, topical retinoic acid, or podophyllum are optional; lesions often recur after stopping treatment
-
Robbins Pathologic Basis of Disease, p. 683; Sleisenger & Fordtran, p. 373-374
Diagnosis and Workup
- Exclude identifiable causes: rule out candidiasis (antifungal trial), lichen planus, hairy leukoplakia, white sponge nevus, leukoedema
- If the lesion does not resolve: incisional biopsy is mandatory
- With large lesions, multiple biopsies are required - target most suspicious areas (erythematous, granular, ulcerated, indurated)
- Serologic testing for HIV if hairy leukoplakia is suspected
- Risk stratification: loss of heterozygosity analysis can help stratify malignant risk
Management
Management depends on biopsy results:
| Histology | Management |
|---|---|
| Benign / no dysplasia | Periodic observation or elective excision |
| Mild dysplasia | Careful follow-up or removal (clinician/patient decision) |
| Moderate dysplasia or worse | Removal is mandatory |
| Invasive SCC | Oncologic resection |
Removal modalities: scalpel excision, laser ablation, electrocautery, cryoablation.
Chemoprevention (e.g., retinoids, beta-carotene): data limited; trials have not yet established clear RCT-level evidence for routine use.
Important caveat: Excision reduces malignant transformation risk but does not eliminate recurrence or transformation risk entirely.
- Cummings Otolaryngology, p. 1581; Sleisenger & Fordtran, p. 374
Recent Evidence (2024-2025)
Three recent systematic reviews are relevant:
- Pimenta-Barros et al., Oral Diseases 2025 (PMID 39314164): Comprehensive meta-analysis on malignant transformation rates in oral leukoplakia.
- Mohideen et al., BMC Oral Health 2025 (PMID 39893387): Meta-analysis showing malignant transformation of PVL is very high.
- Bhattarai et al., J Dent Res 2024 (PMID 39290142): Systematic review and network meta-analysis on recurrence rates after treatment.
Summary Table
| Feature | Detail |
|---|---|
| Definition | White oral plaque - exclusionary clinical diagnosis |
| Most common cause | Tobacco (smoked/smokeless) |
| Most common site | Lip vermilion, then buccal mucosa |
| Highest risk sites | Floor of mouth, ventral/lateral tongue |
| Dysplasia rate | 3.7-28.7% |
| Malignant transformation | 0.13-17.5% (ordinary); 70-87% (PVL) |
| Biopsy indication | If lesion persists after excluding other causes |
| High-risk appearance | Heterogeneous, speckled, nodular, erythroleukoplakia |
| Hairy leukoplakia | EBV, cannot be scraped off, lateral tongue, HIV-associated |
This is a shared conversation. Sign in to Orris to start your own chat.