
IMG_1189.jpeg
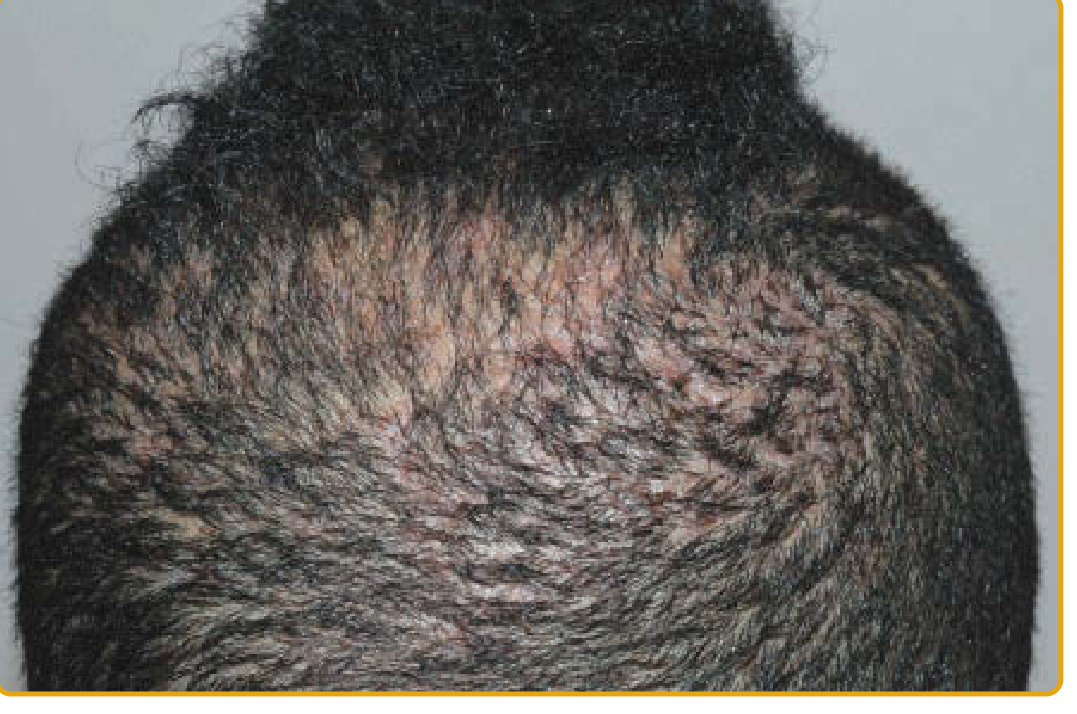
Small pustule like elevations throughout scalp and old goes and new arises, pain itching present, management
analyse_media
Reading File
Finding Sources
Finding Sources
Searching PubMed
scalp folliculitis treatment management
Finding Sources
Reading Article
PMID: 41146582
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
I now have all the information needed for a thorough answer. Here is the complete clinical response:
Likely Diagnosis: Folliculitis Decalvans (FD)
The clinical picture - recurring pustule-like follicular lesions throughout the scalp, pain, pruritus, with old ones resolving and new ones continuously arising - is the classic presentation of Folliculitis Decalvans, a neutrophilic primary cicatricial (scarring) alopecia. The image shows early-stage hair thinning/alopecia along the central scalp, consistent with early FD progression.
Below is a textbook image of more advanced FD showing the characteristic erythematous scarring patch with pustules at the active margin:

Key Clinical Features of Folliculitis Decalvans
| Feature | Detail |
|---|---|
| Who | Young/middle-aged adults, predominantly men |
| Sites | Vertex and occipital scalp most commonly |
| Lesions | Recurrent follicular pustules, perifollicular erythema, scaling, hemorrhagic crusts |
| Hallmark | "Tufted folliculitis" - 5-20 hairs emerging from one follicular unit |
| Course | Pustules arise and resolve cyclically; coalescence leads to scarring patches |
| Cause | Abnormal host immune response to follicular microbiome; Staphylococcus aureus isolated in 20-75% of cases |
- Dermatology 2-Volume Set 5e, p. 3836
Management
First-Line: Antibiotic Combination Therapy (Best Evidence)
Clindamycin + Rifampin is the regimen with the longest documented disease remission:
- Clindamycin 300 mg twice daily
- Rifampin 300 mg twice daily
- Duration: 8-10 weeks
- This combination may be repeated if disease relapses
Alternative antibiotics with shorter remission times:
-
Doxycycline (monotherapy or combination)
-
Trimethoprim-sulfamethoxazole (TMP-SMX 160/800 mg/day)
-
Azithromycin (shorter remission)
-
Long-term tetracyclines (sustained response reported)
-
Goldman-Cecil Medicine, p. 1474; Dermatology 5e, p. 3843; Andrews' Diseases of the Skin
Supplemental/Topical Therapy
- Topical corticosteroids - to reduce perifollicular inflammation
- Topical calcineurin inhibitors - supplemental anti-inflammatory
- Intralesional corticosteroids - for localized active areas
Second-Line / Refractory Cases
- Isotretinoin - sometimes effective but evidence remains controversial
- Cyclosporine - immunosuppressive option
- TNF-alpha inhibitors: adalimumab, infliximab (low evidence, biologic option)
- Secukinumab (IL-17 inhibitor)
- Apremilast (PDE4 inhibitor)
- JAK inhibitors - emerging evidence
- Photodynamic therapy
- Laser therapies
A 2025 systematic review of 728 patients (PMID 41146582) found that combination therapy (systemic antibiotics + topical and/or other systemic agents) outperforms antibiotic monotherapy, with biologics and laser therapy playing a growing role.
Practical Approach Summary
- Confirm diagnosis - swab pustules for bacterial culture/sensitivity (rule out MRSA)
- Start Clindamycin 300 mg BD + Rifampin 300 mg BD for 10 weeks
- Add topical potent corticosteroid (e.g. clobetasol) to active margins
- Trichoscopy at follow-up to assess response
- Warn patient: this is a chronic relapsing condition; repeat antibiotic courses are often needed, and scarred areas will not regrow hair
- If no response after two courses, escalate to isotretinoin or dermatology referral for biologic therapy
Differential Diagnoses to Consider
- Dissecting cellulitis of the scalp - painful boggy nodules with draining sinuses, also causes scarring alopecia
- Acne keloidalis nuchae - folliculitis at nape with keloid formation, overlaps in some patients
- Tinea capitis - fungal; look for broken hairs, KOH prep will confirm
- Lichen planopilaris - scarring alopecia without prominent pustules
- Bacterial furunculosis - isolated furunculosis without progressive cicatricial pattern
Note: If pustules are predominantly superficial and non-scarring without the cyclic recurrence pattern described, simple bacterial folliculitis (from S. aureus) is also possible and responds to shorter antibiotic courses (10-14 days).
Folliculitis Decalvans, management
Finding Sources
Searching PubMed
folliculitis decalvans treatment
Reading File
Reading File
Reading File
Reading Article
PMID: 40230058
Reading Article
PMID: 41146582
Reading File
Loading Image
Loading Image
I now have comprehensive data from 4 textbooks plus the 2025 EADV position statement and 2025 systematic review. Here is the full, structured management guide:
Folliculitis Decalvans (FD) - Management
The most common primary neutrophilic scarring alopecia (~11% of primary cicatricial alopecias). Course is chronic and relapsing - the goal of all therapy is to control inflammation and prevent further hair loss. Hair regrowth in scarred areas cannot be expected.
Clinical appearance - active disease with pustules, crusting, erythema, and early scarring patches:

Step 1: Initial Workup (Before Treatment)
- Bacterial swab of pustules - culture and sensitivity (to identify S. aureus and guide antibiotic choice, rule out MRSA)
- Intranasal swab - S. aureus nasal carriage is a reservoir for recurrence
- Trichoscopy to assess active vs. burned-out disease
- Scalp biopsy if diagnosis is uncertain
Treatment Algorithm (Based on 2025 EADV Position Statement + Textbooks)
Mild Active Disease (perifollicular erythema, hyperkeratosis, NO pustules or crusts)
- Oral isotretinoin - first-line for mild disease (0.5-1 mg/kg/day)
- Topical potent corticosteroids to active areas
- Add topical antibiotics (mupirocin, fusidic acid)
Moderate-to-Severe Active Disease (active pustules, crusts, expanding alopecia)
Best evidence: Clindamycin + Rifampin combination
| Drug | Dose | Duration |
|---|---|---|
| Clindamycin | 300 mg twice daily | 10 weeks |
| Rifampin | 300 mg twice daily | 10 weeks |
- This combination gives the longest period of disease remission of all antibiotic regimens
- Note: rifampin must never be used as monotherapy (promotes resistance)
- Courses may be repeated on relapse
Alternative systemic antibiotics (shorter remission times):
- Doxycycline 100 mg BD (long-term; antineutrophilic + antimicrobial action; long-term use sustains response)
- Minocycline, erythromycin, cephalosporins, TMP-SMX (160/800 mg/day)
- Azithromycin (shorter remission)
- Oral fusidic acid (alone or in combination)
- Oral zinc sulfate (adjunctive)
For highly active disease - add a short course of oral glucocorticosteroids to rapidly reduce inflammation while antibiotics take effect
Topical and Local Therapies (add to all systemic regimens)
- Topical antibiotics: mupirocin, 1.5% fusidic acid, 2% erythromycin
- Antibacterial cleansers / selenium sulfide shampoo
- Intralesional triamcinolone acetonide 10 mg/mL every 4-6 weeks - reduces itching, burning, pain at active margins
- Topical potent corticosteroids (e.g. clobetasol) to active areas
- Intranasal mupirocin - to eradicate S. aureus nasal carriage and reduce recurrence
Refractory / Persistent Disease
| Agent | Notes |
|---|---|
| Isotretinoin (oral) | Effective in some; also recommended for persistent inflammatory lesions post-antibiotics |
| Adalimumab (preferred biologic) | TNF-alpha inhibitor; 2025 EADV recommends as preferred biologic |
| Infliximab | Anti-TNF alternative |
| JAK inhibitors | Emerging evidence; growing role |
| Secukinumab | IL-17 inhibitor |
| Apremilast | PDE4 inhibitor |
| Cyclosporine | Immunosuppressive; low evidence |
| Dapsone (oral) | EADV 2025 recommends |
| Hydroxychloroquine | EADV 2025 recommends |
| Photodynamic therapy (PDT) | Low evidence but reported effective |
| Laser therapy | Useful adjunct |
| Topical tacrolimus 0.1% | Second-line topical; calcineurin inhibitor |
| Topical dapsone 5% | Second-line topical per EADV 2025 |
Long-Term / Maintenance Strategy
- Many patients need long-term low-dose antibiotics for years (especially doxycycline or tetracyclines) to prevent relapse
- "Treatment extended beyond resolution of active lesions" is recommended to avoid recurrence (2025 EADV position statement)
- Combination therapy (systemic + topical + local) consistently outperforms monotherapy in remission duration
Surgical Options (Inactive Disease Only)
- Hair transplantation - only in patients with proven inactive disease (no active pustules or inflammation for at least 1-2 years)
- Surgical excision of affected areas in localised cases
Patient Counselling Points
- This is a chronic relapsing condition - long-term management is necessary
- Scarred areas will NOT regrow hair - goal is to stop further loss
- Antibiotic courses are frequently repeated on relapse
- Compliance with topical + systemic treatment simultaneously is important
- Regular dermatology follow-up with trichoscopy to monitor disease activity
Sources: - Dermatology 2-Volume Set 5e, p. 3843 | Fitzpatrick's Dermatology Vol. 1-2, p. 1559 | Andrews' Diseases of the Skin, p. 3755 | Goldman-Cecil Medicine, p. 1474 | EADV Task Force Position Statement 2025 (PMID 40230058) | Systematic Review of FD Management, 728 patients, 2025 (PMID 41146582)
This is a shared conversation. Sign in to Orris to start your own chat.