Safe Chronic Suppurative Otitis Media
Reading File
Finding Sources
Searching PubMed
"chronic suppurative otitis media" AND management
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Searching Images
chronic suppurative otitis media tympanic membrane perforation
Loading Image
Finding Sources
Finding Sources
I have comprehensive content. Here is the complete, structured answer on Safe (Tubotympanic) CSOM.
Safe Chronic Suppurative Otitis Media (Tubotympanic Disease)
Definition & Terminology
CSOM is defined as chronic inflammation of the middle ear and mastoid with persistent or recurrent otorrhea through a tympanic membrane (TM) perforation lasting >6–12 weeks. It is classically divided into two types:
| Feature | Safe (Tubotympanic) | Unsafe (Atticoantral) |
|---|---|---|
| Also called | Mucosal disease, Benign type | Squamosal disease |
| TM perforation | Central (pars tensa) | Marginal / attic (pars flaccida) |
| Discharge | Mucoid / mucopurulent, odourless | Scanty, foul-smelling |
| Cholesteatoma | Absent | Present |
| Bone erosion | Rare | Common |
| Complications | Less frequent | Frequent |
| Prognosis | Good | Guarded |
The term "safe" reflects the absence of keratin-collecting cholesteatoma and the rarity of serious complications — it is a mucosal disease confined to the pars tensa and middle ear.
Epidemiology & Risk Factors
- Most prevalent in children < 2 years, low-income settings with limited healthcare access
- Global burden is significant — a 2025 systematic review estimated CSOM affects a substantial portion of children in lower-resource regions
- Risk factors:
- Multiple/recurrent episodes of acute otitis media (AOM)
- AOM in early infancy
- Chronic secretory OM
- Eustachian tube (ET) dysfunction
- Tympanostomy tubes or TM perforation allowing external contamination
- Genetic predisposition (Native Americans, Inuit, Native Australians, Māori)
- Nasopharyngeal reflux
(K J Lee's Essential Otolaryngology)
Pathogenesis
Eustachian Tube Dysfunction — Central Mechanism
- Abnormal ET function → decreased middle ear (ME) aeration
- Nitrogen-absorbing cells in mastoid reduce ME volume
- Negative ME pressure develops
- TM retraction — most susceptible area is pars flaccida (atticoantral); in tubotympanic disease, retraction confined to pars tensa
- Perforation acts as a compensatory mechanism for aeration
Role of Biofilms
Bacterial biofilms are central to the chronicity of CSOM:
- Highly organized networks of sessile bacteria enclosed in oligopolysaccharide matrix
- Escape phagocytosis and humoral immunity due to impenetrable matrix
- Gain protection from pH/temperature changes
- Decreased metabolic rate and altered gene expression
- Produce efflux pumps against antibiotics → high resistance
- Frequently polymicrobial — harder to target
- May be adherent to respiratory epithelium, within mucus, or intracellular (reservoir for persistent infection)
(K J Lee's Essential Otolaryngology)
Bacteriology
| Organism | Frequency |
|---|---|
| Pseudomonas aeruginosa | Most common in OM biofilms |
| Staphylococcus aureus | Common |
| Non-typeable H. influenzae | Common |
| Moraxella catarrhalis | Common |
| Anaerobes | Present in mixed infections |
| Candida spp. | Up to 35% of ears treated with topical ciprofloxacin |
Notably, fungal overgrowth (otomycosis) is surprisingly common — one prospective study found Candida in 10% of ears with purulent otorrhea and in 35% following 3 weeks of topical ciprofloxacin treatment.
(Cummings Otolaryngology Head and Neck Surgery)
Clinical Features
Symptoms
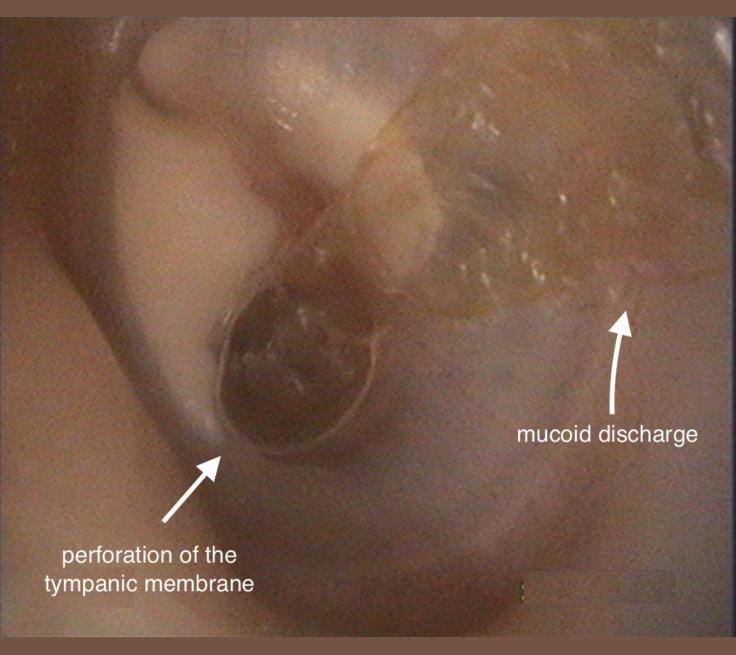
- Chronic or recurrent otorrhea — typically mucoid/mucopurulent, odourless (distinguishes from unsafe type)
- Conductive hearing loss — usually low-frequency; mixed hearing loss can occur
- Aural fullness
- Rarely: otalgia (suggests complication)
Signs
- Central TM perforation (pars tensa) — the hallmark; margins do not reach the annulus
- ME mucosal inflammation
- Granulation tissue / aural polyps (may obscure landmarks)
- No cholesteatoma — if keratin debris or foul odour is present, re-classify as unsafe
- Complicated CSOM may show facial nerve paresis, vertigo (labyrinthine fistula), or signs of intracranial infection — though these are far more common in the unsafe type
(K J Lee's Essential Otolaryngology)
Diagnosis
Key Principle
The primary diagnostic goal is to exclude cholesteatoma. An aural polyp should be considered cholesteatoma until proven otherwise.
Assessment Tools
| Investigation | Purpose |
|---|---|
| Otomicroscopy with pneumatic insufflation | Assess TM, identify perforation type, exclude retraction pocket |
| Audiometry | Quantify conductive hearing loss; identify sensorineural component |
| High-resolution CT temporal bones | Surgical planning; rule out cholesteatoma, bone erosion, tegmen/sigmoid sinus involvement; required in complicated cases, revision surgery |
| MRI with contrast | Suspected intracranial complications |
| Biopsy of granulation tissue | Unresponsive to topical therapy → exclude malignancy |
Treatment
Primary Goal
"Creation of a safe, dry ear"
- Dry = no otorrhea
- Safe = no keratin debris collection, reduced risk of suppurative complications
(K J Lee's Essential Otolaryngology)
Step 1: Aural Toilet
Meticulous suction clearance of discharge and debris is essential before any topical therapy. This removes biofilm and allows antibiotic penetration.
Step 2: Medical Management
Topical antibiotics (first-line):
- Fluoroquinolones (e.g., ciprofloxacin/ofloxacin ear drops) — preferred due to P. aeruginosa coverage and safety profile; 4–6 week course following debridement
- Polymyxin B or neomycin (±steroid)
- Note: biofilms frequently resist topical medication; multicellular strategies overcome even high antibiotic concentrations
Acetic acid / alcohol (antiseptic): effective against Pseudomonas and fungi; useful adjunct
Systemic antibiotics: A 2025 Cochrane review has evaluated systemic antibiotics for CSOM — evidence supports judicious use when topical therapy fails, but topical remains the primary modality
No role for adenoidectomy except in select cases
Step 3: Surgery
Indicated when medical treatment fails or hearing restoration is desired:
Tympanoplasty (Myringoplasty)
- Closure of TM perforation (pars tensa)
- Success rate: 60–90%
- Favourable predictor: patient able to insufflate air through the perforation (Valsalva manoeuvre)
- Timing in children: generally deferred until ~10 years — older children have better outcomes due to more mature ET function
- Earlier surgery if troublesome otorrhea or significant hearing loss
- Contralateral ear health is a more reliable predictor of success than age alone
- Graft materials: temporalis fascia, perichondrium, cartilage
Tympanomastoidectomy
Indicated for:
- Suspected or confirmed cholesteatoma
- Otorrhea refractory to medical treatment
- TM perforation closure rates are not increased by concomitant mastoidectomy alone
Goals:
- Remove all cholesteatoma
- Remove all granulation tissue
- Restore continuity between ME cleft and mastoid cavity
Surgical approaches:
- Atticotomy (transcanal)
- Canal wall up (CWU) — preferred in children; lower morbidity, no cavity maintenance required
- Canal wall down (CWD) with or without obliteration
- Modified radical / Bondy procedure
CWU vs CWD in children: CWU is preferred despite a higher second-look rate, as open cavities require regular debridement (often under GA in children) and meatoplasty causes cosmetic and hearing-aid fitting problems. (Cummings Otolaryngology)
Eustachian Tube Interventions
- Balloon tuboplasty, laser tuboplasty, ET implants (stenting) — no ET treatment has demonstrated long-term efficacy
Complications
Safe CSOM has fewer complications than the unsafe type, but can still cause:
Intratemporal:
- Conductive hearing loss (most common)
- Sensorineural hearing loss (toxins tracking to round window)
- Tympanosclerosis
- Facial nerve palsy (rare)
- Labyrinthitis
Intracranial (rare in safe type):
- Meningitis
- Brain abscess
- Sigmoid sinus thrombosis
- Subdural/extradural abscess
Special Situation: CSOM and Cochlear Implantation
Cochlear implantation was initially contraindicated in CSOM. Retrospective studies show OM prevalence/severity does not increase after implantation. Current practice:
- Implant if the ear is dry at time of surgery
- Multiple protocols exist: single-stage vs two-stage (mastoid obliteration first, then CI 2–6 months later)
- All patients receive perioperative antimicrobial prophylaxis (Cummings Otolaryngology Head and Neck Surgery)
Summary Comparison: Safe vs Unsafe CSOM
SAFE (Tubotympanic) UNSAFE (Atticoantral)
─────────────────────────── ──────────────────────────
Central perforation Marginal/attic perforation
Pars tensa Pars flaccida
Mucoid, odourless discharge Scanty, foul-smelling
No cholesteatoma Cholesteatoma present
Mucosal disease Squamosal disease
Medical ± tympanoplasty Surgery mandatory
Fewer complications Higher complication risk
Key References:
- K J Lee's Essential Otolaryngology, 11th ed.
- Cummings Otolaryngology Head and Neck Surgery, 7th ed.
- Harriet Lane Handbook, 23rd ed.
- Onifade et al. (2025) — Epidemiology of CSOM: global prevalence [PMID: 40178730]
- Chong et al. (2025) — Cochrane: Systemic antibiotics for CSOM [PMID: 40484405]
This is a shared conversation. Sign in to Orris to start your own chat.