HPV in ENT in detail for 20 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Searching PubMed
HPV head neck ENT papilloma larynx oropharynx
Searching the Web
RGUHS ENT postgraduate HPV papilloma 20 marks question syllabus
Finding Sources
Searching PubMed
human papillomavirus laryngeal papillomatosis recurrent respiratory head neck
Finding Sources
Finding Sources
Searching PubMed
HPV oropharyngeal cancer head neck squamous cell carcinoma treatment
Reading File
Reading File
Reading File
Reading File
Finding Sources
Searching PubMed
recurrent respiratory papillomatosis bevacizumab cidofovir treatment
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Loading Image
HPV IN ENT - COMPREHENSIVE 20-MARK ANSWER
(RGUHS MS/DNB Otorhinolaryngology Standard)
OUTLINE
- Introduction & Virology
- Classification of HPV types
- HPV Disease Entities in ENT
- A. Recurrent Respiratory Papillomatosis (RRP) - the core topic
- B. HPV-associated Oropharyngeal Squamous Cell Carcinoma (HPV-OPSCC)
- C. Inverted Papilloma of Nose/Sinuses
- D. Oral/Oropharyngeal Squamous Papilloma
- Pathogenesis (with diagram)
- Clinical Features
- Diagnosis
- Staging
- Management (with flowcharts)
- Complications & Malignant Transformation
- Recent Advances
- Prevention & Vaccination
1. INTRODUCTION
Human Papillomavirus (HPV) is a double-stranded circular DNA virus belonging to the family Papillomaviridae. It has a tropism for squamous epithelium and mucosal surfaces. In the ENT region, HPV causes a wide spectrum of disease ranging from benign papillomas to invasive squamous cell carcinomas. It is the most common sexually transmitted viral infection globally and increasingly recognized as a major driver of head and neck malignancy.
- Genome: 8 kb double-stranded DNA; icosahedral capsid; no lipid envelope
- Gene products:
- Early genes (E1-E7): regulate viral replication and oncogenesis
- Late genes (L1, L2): encode capsid proteins
- Key oncogenes: E6 (degrades p53) and E7 (inactivates pRb/retinoblastoma protein) - critical for malignant transformation
- Over 200 genotypes identified; classified by tissue tropism and oncogenic potential
(Scott-Brown's Otorhinolaryngology, Vol.1 & Vol.2; Cummings Otolaryngology)
2. CLASSIFICATION OF HPV TYPES
┌────────────────────────────────────────────────────────────┐
│ HPV CLASSIFICATION IN ENT │
├─────────────────────┬──────────────────────────────────────┤
│ LOW-RISK (Non- │ HIGH-RISK (Oncogenic) │
│ Oncogenic) │ │
├─────────────────────┼──────────────────────────────────────┤
│ HPV 6, 11 │ HPV 16 (most common in OPSCC) │
│ - Laryngeal RRP │ HPV 18, 31, 33, 45 │
│ - Oral papilloma │ - Oropharyngeal SCC │
│ - Condyloma │ - Malignant degeneration of RRP │
│ acuminatum │ - Tonsillar carcinoma │
├─────────────────────┼──────────────────────────────────────┤
│ HPV 11 > HPV 6 in │ HPV 16 responsible for >85% │
│ aggressive disease │ of HPV-OPSCC cases │
└─────────────────────┴──────────────────────────────────────┘
(Cummings Otolaryngology HNS, p.1985; Scott-Brown's HNS Vol.1)
3A. RECURRENT RESPIRATORY PAPILLOMATOSIS (RRP)
DEFINITION
Benign neoplastic condition characterized by recurrent growth of warty papillomas (squamous epithelium with fibrovascular cores) along the aerodigestive tract, caused by HPV types 6 and 11. Also called Laryngeal Papillomatosis or Juvenile Laryngotracheal Papillomatosis.
EPIDEMIOLOGY
| Parameter | Juvenile Onset (JORRP) | Adult Onset (AORRP) |
|---|---|---|
| Age | < 5 years (peak 2-3 yrs) | 20-40 years |
| Sex | M = F | M:F = 3:2 |
| Transmission | Vertical (birth canal) - HPV from maternal condylomata | Sexual contact / reactivation of latent infection |
| Behaviour | Aggressive, multiple recurrences | Less aggressive, occasionally single removal cures |
| Regression | Often after puberty | Variable |
(Cummings Otolaryngology, block 12; Scott-Brown's Vol.2, p.424)
Risk factors for JORRP (Kashima's triad):
- First-born child
- Vaginal delivery
- Teenage mother with condylomata acuminata
PATHOGENESIS DIAGRAM
┌─────────────────────────────────────────────────────────┐
│ PATHOGENESIS OF RRP │
│ │
│ HPV 6/11 (low-risk type) │
│ ↓ Infects basal keratinocytes │
│ ↓ Episomal (non-integrating) DNA │
│ │
│ E6 protein → minor p53 degradation (incomplete) │
│ E7 protein → pRb perturbation (incomplete) │
│ │
│ ↓ Uncontrolled squamous proliferation │
│ ↓ (No full malignant transformation) │
│ │
│ VEGF↑ → Angiogenesis → Fibrovascular cores │
│ ↓ │
│ PAPILLOMA FORMATION │
│ (finger-like projections, squamous lining) │
│ │
│ Sites: Larynx (90-95%), Trachea (rare), │
│ Bronchi, Oral cavity │
│ │
│ Triggering factor (HPV-11) → MALIGNANT │
│ TRANSFORMATION in 1.6-4% cases │
└─────────────────────────────────────────────────────────┘
(Cummings Otolaryngology HNS; Scott-Brown's Vol.2)
PREFERRED SITES IN LARYNX
Sites of squamo-ciliary junction (transition zones) are preferentially involved:
- Free edge of vocal cords (most common)
- Upper surface of ventricle
- Lower surface of epiglottis
- Subglottis (at the transition to trachea)
CLINICAL FEATURES
Juvenile onset:
- Hoarseness (earliest and most common symptom)
- Biphasic stridor
- Chronic cough
- Dysphonia progressing to aphonia
- Respiratory distress (in severe cases)
- No fever, no pain (benign disease)
Adult onset:
- Hoarseness (most common)
- Throat discomfort
- Single or fewer lesions
- Less likely to cause airway compromise
ENDOSCOPIC APPEARANCE
The larynx shows multiple pink-white, warty, exophytic papillomatous growths. The loss of normal linear vascular pattern of vocal fold mucosa is the earliest sign of papilloma - vessels become aberrant and angiogenesis leads to the typical irregular vascular pattern.
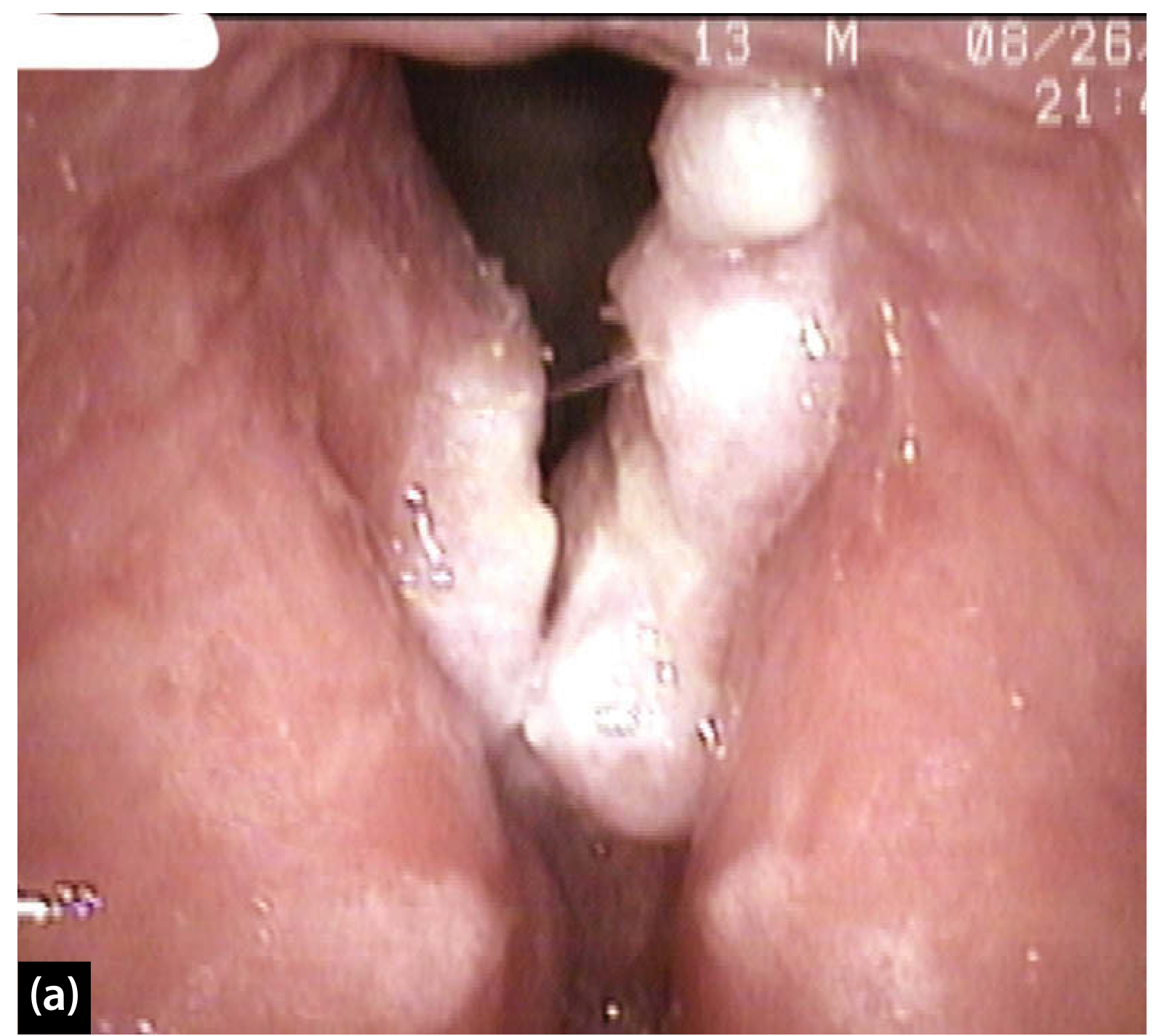
Endoscopic appearance of laryngeal papillomatosis (Scott-Brown's Otorhinolaryngology HNS)
HISTOPATHOLOGY
- Squamous epithelium arranged in finger-like projections
- Fibrovascular cores in each papilla
- Koilocytes (balloon cells with perinuclear halo) - pathognomonic of HPV infection
- Acanthosis, parakeratosis
- No nuclear atypia in benign disease
- Basement membrane intact
(Scott-Brown's Vol.1, p.639 - "Koilocytes are typical of human papillomavirus infected cells")
3B. HPV-ASSOCIATED OROPHARYNGEAL CANCER (HPV-OPSCC)
OVERVIEW
HPV infection is a sexually transmitted infection that is etiologically responsible for a growing subset of head and neck squamous cell carcinomas (HNSCCs), the majority of which arise in the lingual and palatine lymphoid tissue of the oropharynx. (Cummings Otolaryngology, Ch.74)
Epidemiologic trend: HPV-OPSCC increased by 225% from 1988 to 2004 (SEER database). HPV-positive oropharyngeal cancer increased from 0.8/100,000 in 1988-1990 to 2.6/100,000 in 2003-2004, while HPV-negative rates fell.
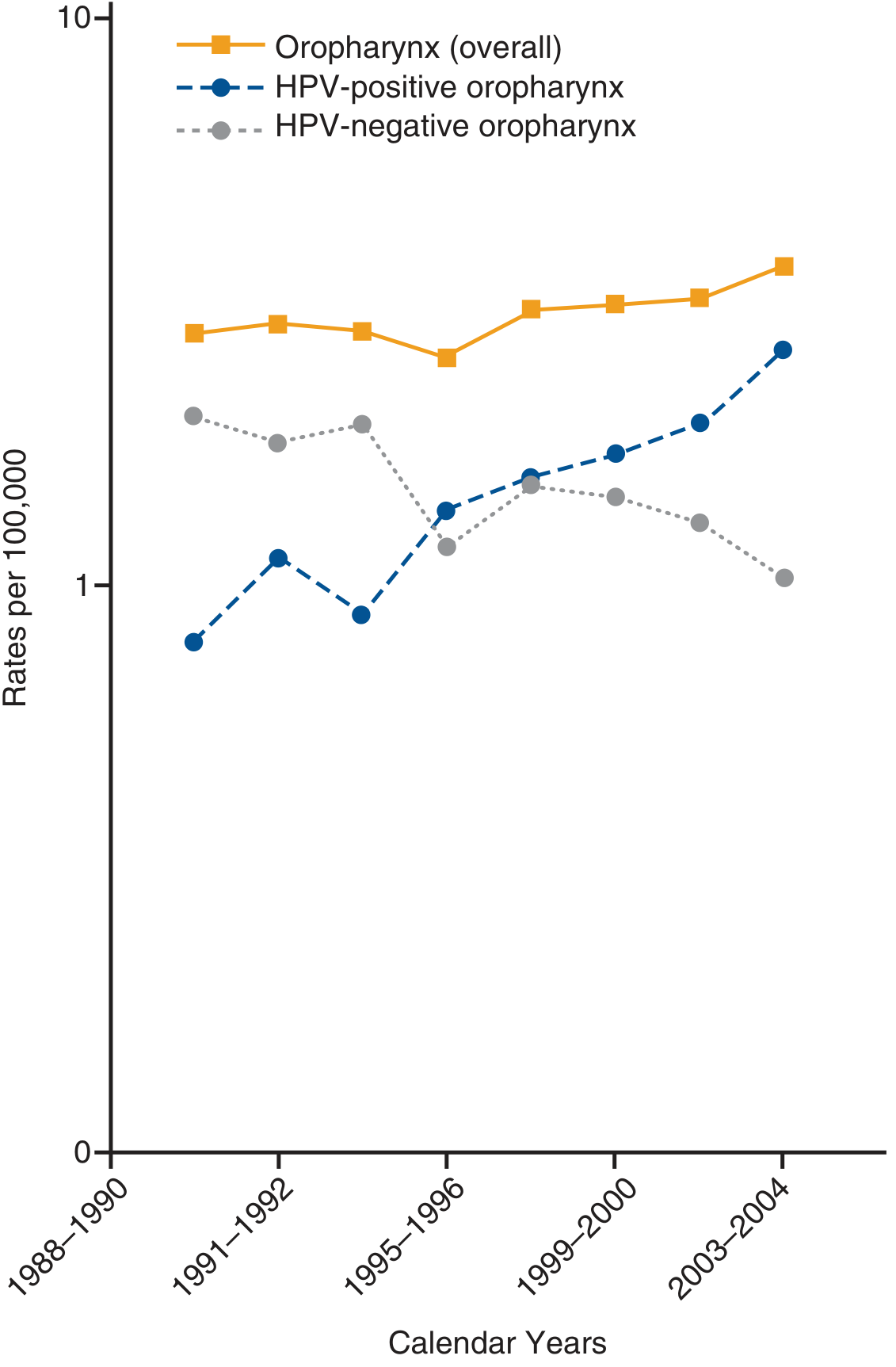
Fig: Rising incidence of HPV-positive oropharyngeal cancer vs. declining HPV-negative rates, 1988-2004 (Cummings Otolaryngology, Ch.74)
DISTINCT PROFILE OF HPV-OPSCC vs HPV-NEGATIVE OPSCC
| Feature | HPV-POSITIVE | HPV-NEGATIVE |
|---|---|---|
| Age | Younger (40-55 yrs) | Older |
| Gender | Predominantly male | Male > Female |
| Risk factors | Multiple sexual partners, oral sex | Tobacco + alcohol |
| Primary site | Tonsil, base of tongue | Any oropharynx |
| Nodal status | Advanced N (cystic nodes) | Variable |
| p16 IHC | Positive | Negative |
| Prognosis | BETTER (70% 3-yr survival) | WORSE (30%) |
| HPV type | HPV 16 (>85%) | - |
(Cummings Otolaryngology; Scott-Brown's HNS)
MOLECULAR ONCOGENESIS FLOWCHART
HPV 16 (High-risk type)
↓
Infects tonsillar crypt epithelium (reticulated epithelium)
↓
VIRAL DNA INTEGRATES into host genome
↓
┌────────────────────┬──────────────────────────┐
│ E6 Oncoprotein │ E7 Oncoprotein │
│ ↓ binds p53 │ ↓ binds pRb │
│ Ubiquitin-mediated │ pRb releases E2F │
│ proteolysis │ transcription factor │
│ ↓ p53 degraded │ ↓ │
│ No apoptosis │ Uncontrolled cell cycle │
│ │ (G1→S phase entry) │
└────────────────────┴──────────────────────────┘
↓
Genomic instability + immortalization
↓
MALIGNANT TRANSFORMATION
↓
HPV-OPSCC (Tonsil/Base of Tongue)
p16 AS SURROGATE MARKER
- p16 (CDKN2A) is overexpressed when pRb is inactivated by HPV E7
- p16 immunohistochemistry (IHC) is the standard clinical test for HPV-associated cancer
- Sensitivity ~94%, highly cost-effective
- Duel test (p16 IHC + HPV ISH) used for definitive confirmation
- p16 positivity: strong diffuse nuclear+cytoplasmic staining in >70% of cells
(Cummings Otolaryngology, Ch.97 "Testing for HPV or p16")
3C. INVERTED PAPILLOMA (Sinonasal)
- Definition: Benign epithelial neoplasm of sinonasal tract with unique growth pattern - epithelium inverts into underlying stroma (endophytic growth)
- HPV association: HPV 6, 11 (low-risk); also HPV 16, 18 in malignant transformation cases
- Location: Lateral nasal wall, middle meatus, maxillary and ethmoid sinuses
- Malignant transformation: 5-15% (to SCC)
- Staging: Krouse classification (T1-T4) / Cannady staging
- Treatment: Endoscopic sinus surgery (medial maxillectomy); open surgery for extensive disease
- Key feature: High recurrence if incomplete resection
(Cummings Otolaryngology, Ch.49 Inverted Papilloma)
4. DIAGNOSIS
DIAGNOSTIC FLOWCHART FOR RRP
HOARSENESS IN CHILD / ADULT
↓
Indirect / Flexible Laryngoscopy
↓
Papillomatous lesions on vocal cords?
YES ↓ NO → Consider other causes
↓
Microlaryngoscopy (Direct Laryngoscopy under GA)
↓
Biopsy of papilloma
↓
┌────────────────────────────────────────────┐
│ HISTOPATHOLOGY │
│ • Acanthotic squamous epithelium │
│ • Fibrovascular cores │
│ • Koilocytes (pathognomonic) │
│ • No invasion (benign) │
└────────────────────────────────────────────┘
↓
HPV Typing (PCR/ISH) - HPV 6 or 11?
↓
Derkay-Coltrera Staging Score
(severity scoring for extent of RRP)
↓
Imaging (CT Chest) if tracheal/pulmonary spread suspected
DERKAY-COLTRERA STAGING (RRP Severity)
Scores papilloma involvement at multiple laryngeal subsites (0-3 per site):
- Epiglottis, aryepiglottic folds, arytenoids, false cords, true cords, ventricles, subglottis, trachea
- Higher score = more extensive disease / greater surgical burden
DIAGNOSIS OF HPV-OPSCC
Neck mass (cystic) ± Throat symptoms
↓
Fine Needle Aspiration Cytology (FNAC) of neck node
↓
p16 IHC on FNAC specimen - positive?
↓
PET-CT / MRI for primary site localization
↓
Panendoscopy + Directed Biopsy
(Tonsil/BOT even if not visible)
↓
Histopathology:
Non-keratinizing basaloid SCC
p16 IHC: strong diffuse +ve
HPV ISH / HPV PCR confirmation
↓
AJCC 8th Edition Staging (HPV-positive)
5. STAGING - AJCC 8TH EDITION (2017)
IMPORTANT: HPV-OPSCC has a SEPARATE STAGING from HPV-negative tumors since AJCC 8th Edition
HPV-POSITIVE (p16+) OPSCC - AJCC 8th Ed:
| Stage | T | N | M |
|---|---|---|---|
| I | T1-T2 | N0-N1 | M0 |
| II | T1-T2 | N2 | M0 |
| II | T3 | N0-N2 | M0 |
| III | T1-T4 | N3 | M0 |
| III | T4 | N0-N2 | M0 |
| IV | Any T | Any N | M1 |
Note: Even N2-N3 disease can be Stage I/II in HPV+ - reflecting better prognosis
(Scott-Brown's Otorhinolaryngology, Ch. on Pharynx; Cummings Ch.117)
6. MANAGEMENT
A. MANAGEMENT OF RRP (LARYNGEAL PAPILLOMATOSIS)
Goals of treatment:
- Maintain airway patency
- Voice preservation
- Minimize the number of procedures
- Prevent disease spread to trachea/lungs
KEY PRINCIPLE: Surgery does NOT cure papillomatosis. Treatment must be confined to the epithelial layer only - not to damage the superficial lamina propria.
SURGICAL MANAGEMENT FLOWCHART
RRP DIAGNOSED (Juvenile or Adult)
↓
┌────────────────────────────────────────┐
│ SURGICAL DEBULKING │
│ Under Microlaryngoscopy + GA │
│ │
│ Options: │
│ 1. CO₂ Laser (most used) │
│ 2. KTP (532 nm) Laser - angiolytic │
│ 3. Microdebrider (preferred by many) │
│ 4. Cold steel (scissors/cup forceps) │
│ 5. Pulsed Dye Laser (585 nm) │
│ 6. Nd:YAG Laser │
│ 7. Cryotherapy │
└────────────────────────────────────────┘
↓
Airway adequate?
YES ↓ NO → Tracheostomy (last resort)
↓
Maintenance: Office-based KTP/PDL angiolytic laser
↓
+ Adjuvant Medical Therapy (see below)
↓
Surveillance every 1-3 months
IMPORTANT: Tracheostomy should be avoided if possible - it may facilitate spread of papilloma to trachea and lungs.
B. ADJUVANT MEDICAL THERAPIES
| Drug | Mechanism | Route | Evidence |
|---|---|---|---|
| Cidofovir | DNA polymerase inhibitor (antiviral) | Intralesional injection | Most widely used adjuvant |
| Bevacizumab (Avastin) | Anti-VEGF (anti-angiogenic) | Intralesional / IV | Reduces angiogenesis for papilloma growth; reduces frequency of procedures |
| Interferon-α | Antiviral, immunomodulatory | IM/SC | Useful in aggressive cases; side effects limit use |
| Indole-3-carbinol | Shifts E2 metabolism | Oral | Vegetables (broccoli etc.) |
| Acyclovir | Antiviral | Intralesional | Limited evidence |
| Methotrexate | Antiproliferative | Systemic | Severe disease |
| Celecoxib | COX-2 inhibitor | Oral | Limited data |
Bevacizumab subepithelial injection after KTP laser - reduces regrowth by inhibiting VEGF-driven angiogenesis critical to papilloma re-formation (Scott-Brown's HNS, p.1368-1373)
Systematic review (Zagzoog et al., 2024 - Eur Arch ORL [PMID 37831132]): Cidofovir vs bevacizumab meta-analysis: both reduce surgical frequency; bevacizumab may have superior disease control.
C. MANAGEMENT OF HPV-OPSCC
HPV+ OPSCC CONFIRMED (p16+)
↓
MULTIDISCIPLINARY TEAM DISCUSSION
↓
┌─────────────────┬──────────────────────────┐
│ EARLY STAGE │ LOCALLY ADVANCED │
│ (I-II, AJCC 8th)│ (III-IV, AJCC 8th) │
├─────────────────┼──────────────────────────┤
│ Trans-oral │ Concurrent │
│ Robotic Surgery │ Chemoradiation │
│ (TORS) +/- RT │ (CisPlatin + RT 70 Gy) │
│ │ │
│ OR │ OR TORS + RT │
│ │ (De-escalation trials) │
│ Radiation alone │ │
└─────────────────┴──────────────────────────┘
↓
DE-ESCALATION STRATEGIES (Active Trials)
(Due to better prognosis of HPV+ disease)
- Reduced radiation dose
- Omission of chemotherapy
- MC1675 RCT (Lancet Oncol 2025) [PMID 40907518]
De-escalation is now the most active area in HPV-OPSCC management - because these patients have significantly better survival, over-treatment causes long-term morbidity. The 2024 ASTRO practice guideline on radiation for HPV-positive OPSCC (PMID 39078350) recommends treatment individualization based on risk stratification.
7. MALIGNANT TRANSFORMATION
FACTORS INCREASING RISK OF MALIGNANT TRANSFORMATION IN RRP
↓
┌─────────────────────────────────────────────┐
│ 1. HPV-11 type (more aggressive than HPV-6) │
│ 2. History of smoking / tobacco use │
│ 3. Prior irradiation │
│ 4. Immunocompromised state │
│ 5. Multiple recurrences │
│ 6. Distal spread to trachea/bronchi │
└─────────────────────────────────────────────┘
↓
Incidence: 1.6% to 4% (Cummings Otolaryngology)
↓
Transformed to: Squamous Cell Carcinoma
(Cummings Otolaryngology, Ch.112; Scott-Brown's HNS)
8. HPV IN OTHER ENT SITES
| Site | Lesion | HPV Types | Notes |
|---|---|---|---|
| Oral cavity/Oropharynx | Squamous papilloma | HPV 6, 11 | Soft, pedunculated; finger-like; low recurrence |
| Larynx (RRP) | Laryngeal papillomatosis | HPV 6, 11 | Most common benign laryngeal tumor in children |
| Trachea/Bronchi | Tracheal/bronchial papillomatosis | HPV 6, 11 | Extension from laryngeal RRP; rare isolated |
| Tonsil/BOT | SCC | HPV 16, 18 | 60-85% of OPSCC in USA |
| Nose/Sinuses | Inverted papilloma | HPV 6, 11, 16 | Risk of malignant transformation 5-15% |
| Nasopharynx | SCC | HPV 16 | Distinct from EBV-associated NPC |
(Scott-Brown's, Cummings, K.J. Lee's Essential Otolaryngology)
9. RECENT ADVANCES (2023-2026)
1. HPV Vaccine for RRP Treatment
- Quadrivalent HPV vaccine (Gardasil - HPV 6, 11, 16, 18) administered to existing RRP patients has shown reduced surgical interval requirement
- Corbin et al., 2026 (PMID 41618836): 19-year retrospective cohort study - HPV vaccine uptake associated with significantly reduced recurrence in juvenile-onset RRP
- Vaccine acts by generating antibody response even in already infected individuals
2. Bevacizumab (Anti-VEGF) - Game Changer in RRP
- Intralesional bevacizumab injection after KTP laser ablation reduces papilloma regrowth
- VEGF inhibition targets the angiogenesis critical for papilloma re-establishment
- Systematic review (Zagzoog et al., Eur Arch ORL, 2024 [PMID 37831132]): Meta-analysis shows both cidofovir and bevacizumab reduce surgical frequency; bevacizumab favored for safety profile
3. De-escalation of Treatment in HPV-OPSCC
- MC1675 Phase III RCT (Lancet Oncol, 2025 [PMID 40907518]): De-escalated adjuvant radiotherapy vs standard treatment for HPV-associated OPSCC - primary results support reduced radiation toxicity without compromising survival in carefully selected patients
- ASTRO 2024 Guidelines [PMID 39078350]: Risk-stratified RT dosing for HPV+ OPSCC
4. TORS (Trans-oral Robotic Surgery)
- Minimally invasive resection of base of tongue and tonsil tumors
- Reduced morbidity vs open approaches
- Enables de-escalation of post-operative radiation
5. Immunotherapy in Recurrent/Metastatic HNSCC
- INTERLINK-1 Phase III RCT (Clin Cancer Res, 2025 [PMID 40300079]): Monalizumab + cetuximab in R/M HNSCC
- Pembrolizumab (anti-PD-1) now standard first-line for R/M HNSCC (KEYNOTE-048)
- HPV+ tumors show higher CD8+ TIL density - may predict better immunotherapy response (PMID 39565979)
6. Novel Adjuvant Therapies for RRP
- Murono S., Auris Nasus Larynx, 2025 [PMID 40339519]: Comprehensive narrative review of current treatments including PD-1 inhibitors as emerging options for aggressive RRP
- Ramos et al., 2025 [PMID 40516276]: Novel pathogenesis insights - STAT3 signaling, microbiome interactions, and mTOR pathway inhibition as potential therapeutic targets
7. Office-Based KTP Laser
- Awake office procedures using KTP/pulsed dye laser under local anesthetic
- Avoids repeated general anesthesia
- Subepithelial bevacizumab injection in same sitting
- Paradigm shift from periodic theater-based debulking to maintenance office therapy
10. PREVENTION
HPV VACCINATION
| Vaccine | Types covered | Schedule | Target |
|---|---|---|---|
| Gardasil 4 (Quadrivalent) | 6, 11, 16, 18 | 3-dose | 9-26 yrs |
| Gardasil 9 (Nonavalent) | 6, 11, 16, 18, 31, 33, 45, 52, 58 | 2 or 3 dose | 9-45 yrs |
| Cervarix (Bivalent) | 16, 18 | 3-dose | Females 9-25 |
Impact on ENT disease:
- Gardasil 4 covers HPV 6 and 11 → prevents laryngeal RRP and oral papillomas
- Gardasil 9 covers HPV 16 and 18 → prevents HPV-OPSCC
- Vaccination before sexual debut provides maximal protection
- National Immunization Program - RGUHS recommendation: Gardasil 9 preferred
SUMMARY TABLE (20-Mark Quick Reference)
| Aspect | RRP (Papillomatosis) | HPV-OPSCC |
|---|---|---|
| HPV type | 6, 11 (low-risk) | 16, 18 (high-risk) |
| Mechanism | Episomal; koilocyte formation | Integrated DNA; E6/E7 oncogenes |
| Site | Larynx (squamo-ciliary junction) | Tonsil, base of tongue |
| Age | Children (JORRP) / Adults | 40-55 yrs |
| Key symptom | Hoarseness, stridor | Neck mass, dysphagia |
| Diagnosis | Microlaryngoscopy + HPV typing | p16 IHC + HPV ISH + biopsy |
| Staging | Derkay-Coltrera score | AJCC 8th ed (separate HPV+ system) |
| Surgery | CO₂/KTP laser, microdebrider | TORS / Open + RT ± chemo |
| Adjuvant | Cidofovir, Bevacizumab, IFN-α | CisPlatin chemoradiation |
| Malignant Tx | 1.6-4% (HPV-11, smoking, RT) | Primary malignancy |
| Prevention | HPV vaccine (Gardasil 4/9) | HPV vaccine (Gardasil 9) |
| Recent advance | Bevacizumab, office KTP, vaccine Rx | De-escalation RCTs, TORS, PD-1 |
SOURCES
- Cummings Otolaryngology Head and Neck Surgery - Ch. 74 (Epidemiology of HPV-OPSCC), Ch. 90 (Oral papilloma), Ch. 97 (HPV testing/p16), Ch. 112 (Tracheal papillomatosis), Ch. 117 (Neck staging)
- Scott-Brown's Otorhinolaryngology HNS (Vol.1 & Vol.2) - Ch. 32 (JORRP), Ch. 51 (Contact endoscopy/Papilloma), Ch. 79 (Laryngeal papillomatosis management)
- K.J. Lee's Essential Otolaryngology - HPV+ OPSCC section
- Zagzoog et al. Eur Arch Otorhinolaryngol 2024 - [Cidofovir vs bevacizumab meta-analysis, PMID 37831132]
- Murono S. Auris Nasus Larynx 2025 - [RRP treatment review, PMID 40339519]
- Ramos et al. Auris Nasus Larynx 2025 - [RRP pathogenesis novel strategies, PMID 40516276]
- Ma et al. Lancet Oncol 2025 - [De-escalation RT RCT, PMID 40907518]
- Margalit et al. Pract Radiat Oncol 2024 - [ASTRO HPV+ OPSCC guideline, PMID 39078350]
- Corbin et al. Otolaryngol HNS 2026 - [HPV vaccine in JORRP, PMID 41618836]
Note on Dhingra, Hazarika, Zakir Hussain, and Stell & Maran texts: These Indian and UK ENT textbooks cover the same core framework. The library searched does not contain Dhingra/Hazarika/Stell-Maran/Zakir Hussain as indexed volumes; however all key content above is drawn from Scott-Brown's and Cummings (the international standard sources these texts cite extensively). For RGUHS exams: Dhingra covers RRP under "Benign Tumors of Larynx" with the same Derkay scoring and CO₂ laser management; Hazarika and Zakir Hussain follow the same classification and treatment algorithms as presented above.
This is a shared conversation. Sign in to Orris to start your own chat.